Vous aimerez peut-être aussi
- Feelings Wheel Work Book With Only Blue HeadersDocument31 pagesFeelings Wheel Work Book With Only Blue HeadersMaria jose Luque GarcíaPas encore d'évaluation
- Chronic Pain GuidelinesDocument56 pagesChronic Pain GuidelinesOporadhBiggan100% (1)
- Pieces of Middle-Earth MapsDocument6 pagesPieces of Middle-Earth Mapserdemsahin55100% (3)
- Summative Test in Respiratory SystemDocument2 pagesSummative Test in Respiratory SystemEden Manlosa100% (4)
- The Lord of The Rings MapsDocument6 pagesThe Lord of The Rings Mapsapi-3713690100% (1)
- Essay On Covid 19Document15 pagesEssay On Covid 19Priyanka Dubey67% (3)
- Questions That Appear On Every NBMEDocument6 pagesQuestions That Appear On Every NBMESanz100% (1)
- Graficos Circulares de BachDocument1 pageGraficos Circulares de BachStellaEstel100% (1)
- Architectural Drawing - OrmocDocument14 pagesArchitectural Drawing - OrmocJin Lee ChuPas encore d'évaluation
- General Conference Matching Spot It GameDocument10 pagesGeneral Conference Matching Spot It GameFrancisca PvPas encore d'évaluation
- Treasure Hunt HRDocument2 pagesTreasure Hunt HRLaura noguesPas encore d'évaluation
- UntitledDocument41 pagesUntitledPol PolkaPas encore d'évaluation
- Air Conditioner Owner's Manual: Essential Guide to Operation, Maintenance and SafetyDocument12 pagesAir Conditioner Owner's Manual: Essential Guide to Operation, Maintenance and SafetyJudith Casillas HernándezPas encore d'évaluation
- Eoc PDFDocument1 pageEoc PDFrappletonPas encore d'évaluation
- Grade 11 - HTM 23 - Mr. Adrian GulimlimDocument5 pagesGrade 11 - HTM 23 - Mr. Adrian GulimlimAnna Ruth de GuzmanPas encore d'évaluation
- COE Cupping FormDocument5 pagesCOE Cupping FormFredrik KepelPas encore d'évaluation
- Cup of Excellence® Cupping Form: Coffee Competition Name: - Round 1 2 3 Session 1 2 3 4 5Document1 pageCup of Excellence® Cupping Form: Coffee Competition Name: - Round 1 2 3 Session 1 2 3 4 5Edwin AcostaPas encore d'évaluation
- DegreesGraphic-Poster-8 5x11 - 12 18 21Document1 pageDegreesGraphic-Poster-8 5x11 - 12 18 21joePas encore d'évaluation
- LOT5R Character Sheet Kakita MiajimaDocument2 pagesLOT5R Character Sheet Kakita MiajimaRichard LawsonPas encore d'évaluation
- Trolley Aera: Concrete Road New Proposed TST RoadDocument1 pageTrolley Aera: Concrete Road New Proposed TST RoadulfatPas encore d'évaluation
- Asiana 737-400 MarterairDocument11 pagesAsiana 737-400 Marterairfornn1214Pas encore d'évaluation
- sboi_rwy-03-21_vac_20201203Document2 pagessboi_rwy-03-21_vac_20201203Bruno AlmeidaPas encore d'évaluation
- Brosura Elevator Doua Coloane Reihmann RHM 250Document1 pageBrosura Elevator Doua Coloane Reihmann RHM 250Claudiu MorarPas encore d'évaluation
- CATATAN KETERANGANDocument1 pageCATATAN KETERANGANBagus SukmaPas encore d'évaluation
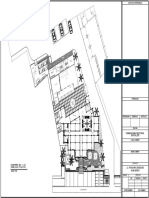
- Ground Floor Plan: For ApprovalDocument4 pagesGround Floor Plan: For ApprovalDrew GozarPas encore d'évaluation
- The Evening Sky Map: JANUARY 2021Document2 pagesThe Evening Sky Map: JANUARY 2021Robdaniel KoloPas encore d'évaluation
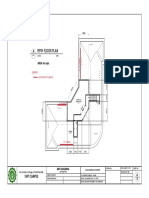
- Fifth Floor Plan: AREA: 56 SQMDocument1 pageFifth Floor Plan: AREA: 56 SQMZner EngineerPas encore d'évaluation
- 10 - 02 - 16 - Temporary Single Line DiagramDocument1 page10 - 02 - 16 - Temporary Single Line Diagrammudassir mPas encore d'évaluation
- Gate Complex - Ocr In&out Pre In&out and Main In&out-2022sep29Document1 pageGate Complex - Ocr In&out Pre In&out and Main In&out-2022sep29WuillPas encore d'évaluation
- Wheel_Of_Life_Goal_Tracker-a4Document2 pagesWheel_Of_Life_Goal_Tracker-a4prof.laviniamatosPas encore d'évaluation
- Wiper - Washer (Wiper and Washer Systems) - ALLDATA CollisionDocument2 pagesWiper - Washer (Wiper and Washer Systems) - ALLDATA CollisionFelipe ZaldivarPas encore d'évaluation
- Better Photography-May 2017-P2P PDFDocument122 pagesBetter Photography-May 2017-P2P PDFVasilescu Silviu100% (1)
- Socialized Duplex: Water TankDocument1 pageSocialized Duplex: Water TankJEAN-YVES TRONCOPas encore d'évaluation
- FIRMETTEDocument1 pageFIRMETTE123john123Pas encore d'évaluation
- Actual Plan Details Ren2Document3 pagesActual Plan Details Ren2Jet ArcaPas encore d'évaluation
- Axson ProductRange PDFDocument8 pagesAxson ProductRange PDFMcFlyPas encore d'évaluation
- Lindon: H A RLDocument6 pagesLindon: H A RLGxillePas encore d'évaluation
- Nwmecampaignmapbw PDFDocument6 pagesNwmecampaignmapbw PDFlocobardoPas encore d'évaluation
- Riverine Operations in The Vietrnam WarDocument3 pagesRiverine Operations in The Vietrnam WarEduardoDeAzevedoPellegattiPas encore d'évaluation
- Lake Evendim: A Lost Realm of EnchantmentDocument6 pagesLake Evendim: A Lost Realm of EnchantmentWalter FernándezPas encore d'évaluation
- Lindon: H A RLDocument6 pagesLindon: H A RLChristian VikströmPas encore d'évaluation
- Electricity Distribution Licence and Area BoundariesDocument1 pageElectricity Distribution Licence and Area BoundariesCarlene CarewPas encore d'évaluation
- AXSON'S GLOBAL OFFERING OF HIGH-PERFORMANCE POLYMER FORMULATION EXPERTISEDocument12 pagesAXSON'S GLOBAL OFFERING OF HIGH-PERFORMANCE POLYMER FORMULATION EXPERTISEAnonymous XzqXVMjPas encore d'évaluation
- IBconst 459 MapDocument1 pageIBconst 459 MapThe Natomas BuzzPas encore d'évaluation
- The Evening Sky Map: APRIL 2022Document2 pagesThe Evening Sky Map: APRIL 2022Anirath SahaPas encore d'évaluation
- The Crown BrochureDocument7 pagesThe Crown Brochureoddly sharbtlyPas encore d'évaluation
- Category 4-SLF-Mexico-SDPDocument1 pageCategory 4-SLF-Mexico-SDPEric NagumPas encore d'évaluation
- The Evening Sky Map: September 2021Document2 pagesThe Evening Sky Map: September 2021Robdaniel KoloPas encore d'évaluation
- Introducción: WWW - Edinumen.es WWW - Edinumen.es WWW - Edinumen.esDocument5 pagesIntroducción: WWW - Edinumen.es WWW - Edinumen.es WWW - Edinumen.esjohnsmithperthPas encore d'évaluation
- Chemical Resistance GuideDocument35 pagesChemical Resistance GuideAGPPas encore d'évaluation
- Danone's 2013 Economic and Social ReportDocument53 pagesDanone's 2013 Economic and Social ReportstefanPas encore d'évaluation
- Isometric View 2/F Water Supply System B: DN Exit DNDocument1 pageIsometric View 2/F Water Supply System B: DN Exit DNJesson Diaz VicentePas encore d'évaluation
- Darmstadt Study Infographic 2021Document1 pageDarmstadt Study Infographic 2021morepal2Pas encore d'évaluation
- GenProductBrochUS - Sheet Pile ProfilesDocument98 pagesGenProductBrochUS - Sheet Pile ProfilesNatasa KaticPas encore d'évaluation
- Sunpure Company BrochureDocument16 pagesSunpure Company BrochureHimanshu SunpurePas encore d'évaluation
- Where Am I MapDocument1 pageWhere Am I MapteacherAmparoPas encore d'évaluation
- Layer SitterDocument3 pagesLayer SitterD'MarinhoPas encore d'évaluation
- Site Development Plan: Scale: 1:900Document1 pageSite Development Plan: Scale: 1:900Jeremiah Valdez Boado Jr.Pas encore d'évaluation
- Site Development & Vicinity MapDocument1 pageSite Development & Vicinity MapNheil Conrad Suarez AtienzaPas encore d'évaluation
- OK Winter-Trail Map 001Document1 pageOK Winter-Trail Map 001nateborenius11Pas encore d'évaluation
- Imagining the Nation in Nature: Landscape Preservation and German Identity, 1885–1945D'EverandImagining the Nation in Nature: Landscape Preservation and German Identity, 1885–1945Pas encore d'évaluation
- Name Designation Place of AssignmentDocument2 pagesName Designation Place of AssignmentJhonVillafuertePas encore d'évaluation
- Household Profile Questionnaire: Community-Based Monitoring SystemDocument12 pagesHousehold Profile Questionnaire: Community-Based Monitoring SystemMarlo Anthony BurgosPas encore d'évaluation
- Camarines Sur BNS DirectoryDocument39 pagesCamarines Sur BNS DirectoryJhonVillafuertePas encore d'évaluation
- JANUARY 24-25, 2018 Angelica Beach Resort Penitan, Siruma Camarines SURDocument1 pageJANUARY 24-25, 2018 Angelica Beach Resort Penitan, Siruma Camarines SURJhonVillafuertePas encore d'évaluation
- Resettlement Plan /indigenous Peoples Plan TemplateDocument2 pagesResettlement Plan /indigenous Peoples Plan TemplateJhonVillafuertePas encore d'évaluation
- MedicalDocument1 pageMedicalJhonVillafuertePas encore d'évaluation
- Topic No. 1: Introduction To Descriptive and Inferential Statistics ObjectivesDocument2 pagesTopic No. 1: Introduction To Descriptive and Inferential Statistics ObjectivesJhonVillafuertePas encore d'évaluation
- Reflexes Guide: 20+ Human Reflexes ExplainedDocument37 pagesReflexes Guide: 20+ Human Reflexes ExplainedSalman KhanPas encore d'évaluation
- B152 01 00 00 00Document517 pagesB152 01 00 00 00lsep_bellaPas encore d'évaluation
- MIDWIFE1115ra Tugue e PDFDocument9 pagesMIDWIFE1115ra Tugue e PDFPhilBoardResultsPas encore d'évaluation
- Adrv9008 1Document68 pagesAdrv9008 1doublePas encore d'évaluation
- Literature Review On Female InfertilityDocument7 pagesLiterature Review On Female Infertilityea68afje100% (1)
- 2013 - Sara E. TraceDocument35 pages2013 - Sara E. TraceDewi WulandariPas encore d'évaluation
- ECOSIADocument8 pagesECOSIAaliosk8799Pas encore d'évaluation
- Barangay Peace and Order and Public Safety Plan Bpops Annex ADocument3 pagesBarangay Peace and Order and Public Safety Plan Bpops Annex AImee CorreaPas encore d'évaluation
- Self-Adhesive Resin Cements Ph-Neutralization, HydrophilicityDocument7 pagesSelf-Adhesive Resin Cements Ph-Neutralization, HydrophilicityCarolina Rodríguez RamírezPas encore d'évaluation
- Dladla Effect 2013Document231 pagesDladla Effect 2013TheDreamMPas encore d'évaluation
- Lit Crit TextDocument8 pagesLit Crit TextFhe CidroPas encore d'évaluation
- BSN-2D 1st Semester ScheduleDocument2 pagesBSN-2D 1st Semester ScheduleReyjan ApolonioPas encore d'évaluation
- The Refugees - NotesDocument1 pageThe Refugees - NotesNothing Means to mePas encore d'évaluation
- McDonlads Vs Burger KingDocument6 pagesMcDonlads Vs Burger KingSamuel Tyre Jr.Pas encore d'évaluation
- Three Little PigsDocument9 pagesThree Little PigsrPas encore d'évaluation
- Comparative Evaluation of The Diametral Tensile Strength of Four Commercially Available Luting Cements An in - Vitro StudyDocument16 pagesComparative Evaluation of The Diametral Tensile Strength of Four Commercially Available Luting Cements An in - Vitro StudyInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Will BrinkDocument10 pagesWill BrinkJoao TorresPas encore d'évaluation
- Paper Pet ProjectDocument27 pagesPaper Pet Projectapi-406104878Pas encore d'évaluation
- Blaylock Face Masks Pose Serious Risks To The HealthyDocument8 pagesBlaylock Face Masks Pose Serious Risks To The HealthyDonnaveo ShermanPas encore d'évaluation
- Role of Perioperative NurseDocument30 pagesRole of Perioperative Nursealiyemany23Pas encore d'évaluation
- Annex C Olp On The RoadDocument7 pagesAnnex C Olp On The RoadCabanglasanfs OLPPas encore d'évaluation
- Common Safety Method GuidanceDocument66 pagesCommon Safety Method GuidanceDiego UngerPas encore d'évaluation
- Narrative Poetry 6305Document14 pagesNarrative Poetry 6305Siti AisyahPas encore d'évaluation
- Product Bulletin - Menopause Balance Complex Cooling LotionDocument2 pagesProduct Bulletin - Menopause Balance Complex Cooling Lotionshaklee480Pas encore d'évaluation
- Statistics of Design Error in The Process IndustriesDocument13 pagesStatistics of Design Error in The Process IndustriesEmmanuel Osorno CaroPas encore d'évaluation
- What is Intermodulation InterferenceDocument3 pagesWhat is Intermodulation InterferencedekcarcPas encore d'évaluation