Vous aimerez peut-être aussi
- Clinical Trial of Targeted Treatment of Systemic Lupus Erythematosus With BelimumabDocument4 pagesClinical Trial of Targeted Treatment of Systemic Lupus Erythematosus With BelimumabCandy SwiftPas encore d'évaluation
- Biolabs - St-Stem Cell-Based Gene Therapy Successfully Treats 6 Patients With Rare Hematological DiseasesDocument2 pagesBiolabs - St-Stem Cell-Based Gene Therapy Successfully Treats 6 Patients With Rare Hematological DiseasesCandy SwiftPas encore d'évaluation
- CAR-NK Cell TherapySafer Choice To Treat TumorsDocument2 pagesCAR-NK Cell TherapySafer Choice To Treat TumorsCandy SwiftPas encore d'évaluation
- Antibodies Types Formats Creative BiolabsDocument1 pageAntibodies Types Formats Creative BiolabsCandy SwiftPas encore d'évaluation
- The Points To Consider For Vaccine Development of SARS-CoV-2 (Part Two)Document2 pagesThe Points To Consider For Vaccine Development of SARS-CoV-2 (Part Two)Candy SwiftPas encore d'évaluation
- CAR T Cell Based Immunotherapy Basic PrinciplesDocument1 pageCAR T Cell Based Immunotherapy Basic PrinciplesCandy SwiftPas encore d'évaluation
- How Bispecific Antibody Treat Cancer TherapyDocument2 pagesHow Bispecific Antibody Treat Cancer TherapyCandy SwiftPas encore d'évaluation
- Biolabs - Gt-Progress of Gene Therapy in Hereditary Optic Nerve Injury and Related DiseasesDocument2 pagesBiolabs - Gt-Progress of Gene Therapy in Hereditary Optic Nerve Injury and Related DiseasesCandy SwiftPas encore d'évaluation
- Will Oncolytic Virotherapy Be The Winner Fighting Against Breast CancerDocument2 pagesWill Oncolytic Virotherapy Be The Winner Fighting Against Breast CancerCandy SwiftPas encore d'évaluation
- Five Things You Should Know About Systemic Lupus ErythematosusDocument2 pagesFive Things You Should Know About Systemic Lupus ErythematosusCandy SwiftPas encore d'évaluation
- Virus Like Particles Based Vaccine Development ServicesDocument1 pageVirus Like Particles Based Vaccine Development ServicesCandy SwiftPas encore d'évaluation
- CAR T Cell Based Immunotherapy Clinical Applications and ChallengesDocument1 pageCAR T Cell Based Immunotherapy Clinical Applications and ChallengesCandy SwiftPas encore d'évaluation
- GMP Vaccine ProductionDocument1 pageGMP Vaccine ProductionCandy SwiftPas encore d'évaluation
- VLP Based VaccinesDocument1 pageVLP Based VaccinesCandy SwiftPas encore d'évaluation
- BispecificDocument2 pagesBispecificCandy SwiftPas encore d'évaluation
- Transcription ToxinsDocument1 pageTranscription ToxinsCandy SwiftPas encore d'évaluation
- Cancer VaccineDocument2 pagesCancer VaccineCandy SwiftPas encore d'évaluation
- DSS-Induced IBD Mice ModelDocument1 pageDSS-Induced IBD Mice ModelCandy SwiftPas encore d'évaluation
- CD19 CAR-T CellDocument2 pagesCD19 CAR-T CellCandy SwiftPas encore d'évaluation
- Breakthrough ADC Therapy For Treatment of Bladder Cancer Shows Positive DataDocument2 pagesBreakthrough ADC Therapy For Treatment of Bladder Cancer Shows Positive DataCandy SwiftPas encore d'évaluation
- Overview On Antibody Drug ConjugateDocument2 pagesOverview On Antibody Drug ConjugateCandy SwiftPas encore d'évaluation
- Electroporation TransferDocument8 pagesElectroporation TransferCandy SwiftPas encore d'évaluation
- Anti-Lymphocyte Tumor Mechanism of CD19-CART CellsDocument2 pagesAnti-Lymphocyte Tumor Mechanism of CD19-CART CellsCandy SwiftPas encore d'évaluation
- Virus Like ParticlesDocument10 pagesVirus Like ParticlesCandy SwiftPas encore d'évaluation
- Analysis of CD19 CAR-T Cell Therapy Clinical TrialsDocument2 pagesAnalysis of CD19 CAR-T Cell Therapy Clinical TrialsCandy SwiftPas encore d'évaluation
- R&D Trends and Challenges of ADC DevelopmentDocument2 pagesR&D Trends and Challenges of ADC DevelopmentCandy SwiftPas encore d'évaluation
- Antibody Drug Conjugate Progress AnalysisDocument2 pagesAntibody Drug Conjugate Progress AnalysisCandy SwiftPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- PowerpointDocument25 pagesPowerpointBhoomika sardanaPas encore d'évaluation
- FOUNDATION OF CONTROL QUESTIONS OF EXAM 2020-2021 General MedicineDocument7 pagesFOUNDATION OF CONTROL QUESTIONS OF EXAM 2020-2021 General MedicineSoz P. KawaniPas encore d'évaluation
- CR Lab ReportDocument6 pagesCR Lab ReportslowteePas encore d'évaluation
- BIO104E-Laboratory Activity. (The Cell)Document5 pagesBIO104E-Laboratory Activity. (The Cell)Stephen AzaresPas encore d'évaluation
- CAPE 2003 BiologyDocument22 pagesCAPE 2003 BiologyTravis Satnarine33% (3)
- Final Single Cell ProteinDocument13 pagesFinal Single Cell Proteinsharmamaddy32Pas encore d'évaluation
- Sample Ch05Document53 pagesSample Ch05mb_13_throwawayPas encore d'évaluation
- Life Science Evidence 1Document5 pagesLife Science Evidence 1Cintia Mtz0% (1)
- Kalyan Sir - Quick Look-3 (Science) PDFDocument7 pagesKalyan Sir - Quick Look-3 (Science) PDFR Aditya Vardhana ReddyPas encore d'évaluation
- ANTIOXIDANT MEXIDOL-The Main Neuropsychotropic EffectDocument21 pagesANTIOXIDANT MEXIDOL-The Main Neuropsychotropic Effectmatsapo100% (1)
- Eul 0515 202 00 Covid19 Coronavirus Real Time PCR Kit IfuDocument28 pagesEul 0515 202 00 Covid19 Coronavirus Real Time PCR Kit IfuashishvaidPas encore d'évaluation
- General Biology 2: Quarter 1 - Module 1: Recombinant DNADocument28 pagesGeneral Biology 2: Quarter 1 - Module 1: Recombinant DNACayessier ViernesPas encore d'évaluation
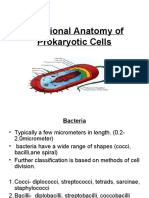
- Functional Anatomy of Prokaryotic CellsDocument28 pagesFunctional Anatomy of Prokaryotic CellsGabz GabbyPas encore d'évaluation
- Unusual Infec, Ous Agents: Lecture 24 Biology W3310/4310 Virology Spring 2013Document61 pagesUnusual Infec, Ous Agents: Lecture 24 Biology W3310/4310 Virology Spring 2013Neo Mervyn MonahengPas encore d'évaluation
- Evolution of Social BehaviorDocument48 pagesEvolution of Social BehaviorNaniPas encore d'évaluation
- Karyotyping: A Test to Examine ChromosomesDocument16 pagesKaryotyping: A Test to Examine ChromosomesIan MaunesPas encore d'évaluation
- Neuroscience: Science of The Brain in FrenchDocument72 pagesNeuroscience: Science of The Brain in FrenchInternational Brain Research OrganizationPas encore d'évaluation
- Nres1dm-Chapter I and IIDocument35 pagesNres1dm-Chapter I and IImlmmandapPas encore d'évaluation
- Fish Diseases and Disorders - Volume 3 - Viral, Bacterial and Fungal Infections (PDFDrive)Document941 pagesFish Diseases and Disorders - Volume 3 - Viral, Bacterial and Fungal Infections (PDFDrive)SARANYA A P SATHIAH SATHIAHPas encore d'évaluation
- General Biology 2: Quarter 3: Week 5 and 6 - Module 5 Taxonomy and SystematicsDocument20 pagesGeneral Biology 2: Quarter 3: Week 5 and 6 - Module 5 Taxonomy and Systematicscristina maquinto83% (6)
- My Copyprotein Folding Virtual ActivityDocument7 pagesMy Copyprotein Folding Virtual Activityapi-521781723Pas encore d'évaluation
- 50 Create A Face LabDocument10 pages50 Create A Face LabmrsginsburgPas encore d'évaluation
- 1.plant Physiological EcologyDocument16 pages1.plant Physiological EcologyNunung PratiwiPas encore d'évaluation
- Etextbook 978 0078096945 Essentials of The Living World 5th EditionDocument61 pagesEtextbook 978 0078096945 Essentials of The Living World 5th Editionmark.dame383100% (44)
- 4 Nucleic Acid HybridizationDocument23 pages4 Nucleic Acid HybridizationBalaji Paulraj100% (1)
- Psyc1001 Sample QuestionsDocument7 pagesPsyc1001 Sample QuestionsRishie RamlalPas encore d'évaluation
- Grade 4 Life Science Structures and FunctionsDocument9 pagesGrade 4 Life Science Structures and Functionszeinab ahmedPas encore d'évaluation
- Biology 20 Course OutlineDocument3 pagesBiology 20 Course Outlineapi-427321002Pas encore d'évaluation
- Course Schedule2016172Document66 pagesCourse Schedule2016172kartavya jainPas encore d'évaluation