Vous aimerez peut-être aussi
- Daun Jambu Biji TabletDocument6 pagesDaun Jambu Biji Tabletrachelsantoso5259Pas encore d'évaluation
- FORT MCCLELLAN VA S-C Decision Favorable To FT McClellan Vet (Citation #1108696)Document6 pagesFORT MCCLELLAN VA S-C Decision Favorable To FT McClellan Vet (Citation #1108696)Agent Orange Legacy100% (2)
- Jurnal Rumus Kadar AbuDocument5 pagesJurnal Rumus Kadar AbualyanuraPas encore d'évaluation
- Textbook On Clinical Ocular Pharmacology & Therapeutics (079-117)Document39 pagesTextbook On Clinical Ocular Pharmacology & Therapeutics (079-117)Claudia Alejandra Varon100% (1)
- JurnalDocument4 pagesJurnallailaPas encore d'évaluation
- Mind Mapping Obat Anti VirusDocument1 pageMind Mapping Obat Anti VirusocepPas encore d'évaluation
- Jurnal Jambu BijiDocument6 pagesJurnal Jambu Bijireni100% (2)
- Artikel Karakterisasi Simplisia PDFDocument17 pagesArtikel Karakterisasi Simplisia PDFSilva ApryllPas encore d'évaluation
- Study of Adverse Drug Reactions Associated With Chemotherapy of Breast CancerDocument7 pagesStudy of Adverse Drug Reactions Associated With Chemotherapy of Breast CancerInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Jurnal Interaksi ObatDocument20 pagesJurnal Interaksi ObatFadhil Muhammad Awaluddin100% (1)
- Erythromycin Dry SyrupDocument7 pagesErythromycin Dry SyrupAufa HamidahPas encore d'évaluation
- SudomoDocument12 pagesSudomoAji Dwi SPas encore d'évaluation
- Review JurnalDocument3 pagesReview JurnalSri Mentari ManurungPas encore d'évaluation
- 5a. Mekanisme Imunitas Seluler Dan HumoralDocument32 pages5a. Mekanisme Imunitas Seluler Dan HumoralGaluh Apsari SyafranPas encore d'évaluation
- Typhoid Management Guidelines - 2019 - MMIDSPDocument14 pagesTyphoid Management Guidelines - 2019 - MMIDSPhasnah shintaPas encore d'évaluation
- Algoritma Terapi IHDDocument1 pageAlgoritma Terapi IHDrenybejoPas encore d'évaluation
- Grafik Pertumbuhan AnakDocument6 pagesGrafik Pertumbuhan AnakIrfa MudarwatiPas encore d'évaluation
- The Essential Facts of FungusDocument2 pagesThe Essential Facts of FungusCantika Quita100% (2)
- Dapus Umum LengkapDocument6 pagesDapus Umum LengkapDhewiantyPas encore d'évaluation
- Dapus Hadis Lengkap SuspensiDocument4 pagesDapus Hadis Lengkap SuspensiPrahedi Setya Ibrahim IIPas encore d'évaluation
- Bio Evailabilitas Dan Bioekivalensi Aciclovir BABEDocument13 pagesBio Evailabilitas Dan Bioekivalensi Aciclovir BABERian Nurdiana100% (1)
- Jurnal MigrainDocument39 pagesJurnal Migrainsandyriaaa100% (1)
- MIC MBC MokrobiologiDocument38 pagesMIC MBC MokrobiologiAtharia Refi KhairaniPas encore d'évaluation
- A Series of in Vitro and Human Studies of A Novel Lip Cream FormulationDocument16 pagesA Series of in Vitro and Human Studies of A Novel Lip Cream FormulationDummy CipawPas encore d'évaluation
- Jurnal Formulasi Krim Gentamisin SulfatDocument15 pagesJurnal Formulasi Krim Gentamisin SulfatNandea Zulfana HendrawanPas encore d'évaluation
- Glasgow Antipsychotic Side-Effect Scale (GASS)Document2 pagesGlasgow Antipsychotic Side-Effect Scale (GASS)psikiatrifile 2017Pas encore d'évaluation
- Meropenem LengkapDocument9 pagesMeropenem Lengkapnoor281982Pas encore d'évaluation
- Jurnal Internasional KLTDocument4 pagesJurnal Internasional KLTAnonymous 52dM3jCJMPas encore d'évaluation
- 1-3 SPOB TeKos Kulit (Skin Care Product)Document113 pages1-3 SPOB TeKos Kulit (Skin Care Product)Gemino Valendra PratamaPas encore d'évaluation
- Stabilitas Obat - OksidasiDocument46 pagesStabilitas Obat - OksidasiFadila FadilaPas encore d'évaluation
- Daun Gatal PDFDocument7 pagesDaun Gatal PDFIswandi AzisPas encore d'évaluation
- Jurnal Ekstrak Etanol Kayu Manis (Cinnamomum Burmannii)Document4 pagesJurnal Ekstrak Etanol Kayu Manis (Cinnamomum Burmannii)DeEo OnoPas encore d'évaluation
- (JDS) Journal of Syiah Kuala Dentistry SocietyDocument11 pages(JDS) Journal of Syiah Kuala Dentistry SocietyDindaPas encore d'évaluation
- TonisitasDocument31 pagesTonisitasMuhammad Azmi AzizPas encore d'évaluation
- Contoh Soal FarmakokinetikDocument3 pagesContoh Soal FarmakokinetikAina AzkiaPas encore d'évaluation
- Bisolvon Solution Product InfoDocument10 pagesBisolvon Solution Product InfoFara EsterPas encore d'évaluation
- Materi 3 - Sifat FisikokimiaDocument61 pagesMateri 3 - Sifat Fisikokimiaashley vechtersbaasPas encore d'évaluation
- Uji Aktivitas Antibakteri Kombinasi Minyak Atsiri Daun Gelam Putih (Melaleuca Leucadendra) Dan Rimpang Jahe (Zingiber Officinale) Terhadap Bakteri Staphylococcus Aureus Dan Escherichia Coli Secara inDocument74 pagesUji Aktivitas Antibakteri Kombinasi Minyak Atsiri Daun Gelam Putih (Melaleuca Leucadendra) Dan Rimpang Jahe (Zingiber Officinale) Terhadap Bakteri Staphylococcus Aureus Dan Escherichia Coli Secara inberliana faradisaPas encore d'évaluation
- A Review On Water Used in Pharma Industry: European Journal of Pharmaceutical and Medical ResearchDocument11 pagesA Review On Water Used in Pharma Industry: European Journal of Pharmaceutical and Medical ResearchDinesh babuPas encore d'évaluation
- PDF DipiroDocument16 pagesPDF DipiroYolandaFandraIIPas encore d'évaluation
- Daftar PustakaDocument3 pagesDaftar PustakaIndrasti BanjaransariPas encore d'évaluation
- Jurnal A Kel 1Document7 pagesJurnal A Kel 1Pratiwi IshakPas encore d'évaluation
- Epidemiology and Control of Acute Diarrheal Diseases: Dr. Anish KhannaDocument21 pagesEpidemiology and Control of Acute Diarrheal Diseases: Dr. Anish KhannaHans Chester Rirao CapindingPas encore d'évaluation
- Dosis Insulin Subkutan Dari I.VDocument2 pagesDosis Insulin Subkutan Dari I.VHazrati UmmiPas encore d'évaluation
- Cara Pemberian ObatDocument35 pagesCara Pemberian ObatRisna ClaraPas encore d'évaluation
- Pengembangan Formulasi Tablet Prednison Secara Kempa Langsung Dengan Teknik Dispersi PadatDocument6 pagesPengembangan Formulasi Tablet Prednison Secara Kempa Langsung Dengan Teknik Dispersi PadatKavitha Sree KanayyaPas encore d'évaluation
- Journal Reading Morbus HansenDocument29 pagesJournal Reading Morbus HansenyoantamaraPas encore d'évaluation
- Jamur OkDocument18 pagesJamur OkdinimusmanPas encore d'évaluation
- Dipiro24 Drug Induced Hematologic Disorder PDFDocument16 pagesDipiro24 Drug Induced Hematologic Disorder PDFPradhani Fakhira DhaneswariPas encore d'évaluation
- Farmasi Fisika KinematikaDocument48 pagesFarmasi Fisika KinematikaLeonardo ImmanuelPas encore d'évaluation
- History of Genetic Manipulation: Recombinant DNA TechnologyDocument69 pagesHistory of Genetic Manipulation: Recombinant DNA TechnologyEmia BarusPas encore d'évaluation
- Alat Dan Bahan Praktikum FTS PadatDocument14 pagesAlat Dan Bahan Praktikum FTS PadatNofran Putra PratamaPas encore d'évaluation
- Plantacare 2000upDocument2 pagesPlantacare 2000upShivon LamPas encore d'évaluation
- Deskripsi MahoniDocument11 pagesDeskripsi MahoniDimas ArieyadiPas encore d'évaluation
- A Review On Film Forming Gel FFGDocument10 pagesA Review On Film Forming Gel FFGEditor IJTSRDPas encore d'évaluation
- Skin and NailsDocument2 pagesSkin and NailsJosé Henríquez GalánPas encore d'évaluation
- Assigment Unit 6 and Unit 20Document5 pagesAssigment Unit 6 and Unit 20Galuh ChanPas encore d'évaluation
- Regulasi Dan Mekanisme EndokrinDocument121 pagesRegulasi Dan Mekanisme Endokrinluthfiyya syafiqaPas encore d'évaluation
- The Journal of Pathology CR - 2016 - Motwani - Novel Translational Model of Resolving Inflammation Triggered by UV Killed EDocument12 pagesThe Journal of Pathology CR - 2016 - Motwani - Novel Translational Model of Resolving Inflammation Triggered by UV Killed EJoshy innitPas encore d'évaluation
- Efficacy of Local Conjunctival Immunotherapy in Allergic ConjunctivitisDocument5 pagesEfficacy of Local Conjunctival Immunotherapy in Allergic ConjunctivitisDyah Kurnia FitriPas encore d'évaluation
- IndianJOphthalmol6791400-3383915 092359Document5 pagesIndianJOphthalmol6791400-3383915 092359diancahyaPas encore d'évaluation
- Jurnal Retinopati DiabetikDocument7 pagesJurnal Retinopati DiabetikPutriIffahPas encore d'évaluation
- Presentasi Trauma ToraksDocument22 pagesPresentasi Trauma ToraksPutriIffahPas encore d'évaluation
- HHS 792 WDocument5 pagesHHS 792 WPutriIffahPas encore d'évaluation
- Leveling Up Part2Document144 pagesLeveling Up Part2PutriIffahPas encore d'évaluation
- XSL FO: Original PaperDocument18 pagesXSL FO: Original PaperPutriIffahPas encore d'évaluation
- Hemangioma, Aneurysmal Bone CystDocument59 pagesHemangioma, Aneurysmal Bone CystPutriIffahPas encore d'évaluation
- Cellulitis & Skin InfectionsDocument6 pagesCellulitis & Skin InfectionsPutriIffahPas encore d'évaluation
- Praktikum Anatomi 3 (Muscle of Head and NeckDocument36 pagesPraktikum Anatomi 3 (Muscle of Head and NeckPutriIffahPas encore d'évaluation
- 04.tulang AxialDocument24 pages04.tulang AxialPutriIffahPas encore d'évaluation
- PhlebitisDocument4 pagesPhlebitisPutriIffahPas encore d'évaluation
- Fasting Blood SugarDocument5 pagesFasting Blood SugarKhamron BridgewaterPas encore d'évaluation
- Learning Objectives Operating RoomDocument3 pagesLearning Objectives Operating RoomAnthony Seth Aguilando100% (1)
- CELYN H. NATURAL MAPEH LESSON PLAN (MR - Gepitulan)Document6 pagesCELYN H. NATURAL MAPEH LESSON PLAN (MR - Gepitulan)Celyn NaturalPas encore d'évaluation
- Law and Med - 2Document9 pagesLaw and Med - 2Anirudh RanaPas encore d'évaluation
- Alternative MedicineDocument306 pagesAlternative MedicineDamir Brankovic100% (3)
- Treatment With Kinesio Taping On The Shoulder Injuries in Water Polo Players: Pilot StudyDocument2 pagesTreatment With Kinesio Taping On The Shoulder Injuries in Water Polo Players: Pilot StudyAna Lu LoboPas encore d'évaluation
- Bedlam Times Article PhotosDocument18 pagesBedlam Times Article PhotosMarcusFelsmanPas encore d'évaluation
- - أسئلة التغذيةDocument52 pages- أسئلة التغذيةMicheal Mikhail YoussefPas encore d'évaluation
- Q2-PPT-PE10-Module1.2 (Running As Exercise)Document30 pagesQ2-PPT-PE10-Module1.2 (Running As Exercise)Gericho MarianoPas encore d'évaluation
- Republic Act No. 11223 or The Universal Health Care ActDocument2 pagesRepublic Act No. 11223 or The Universal Health Care ActChristine Joy MolinaPas encore d'évaluation
- Food Security: A PrimerDocument4 pagesFood Security: A PrimerjournalPas encore d'évaluation
- General Principles of Toxicology-1Document37 pagesGeneral Principles of Toxicology-1Musa yohanaPas encore d'évaluation
- Guided Self-Help Exercise Program in Total laryngectomy-RCT PDFDocument9 pagesGuided Self-Help Exercise Program in Total laryngectomy-RCT PDFazharbattooPas encore d'évaluation
- CHN 2 Module3Document22 pagesCHN 2 Module3divinePas encore d'évaluation
- Studentsworksheets PbirevisedDocument8 pagesStudentsworksheets Pbirevisedapi-246444495Pas encore d'évaluation
- Dental JurisprudenceDocument6 pagesDental JurisprudenceDeepuPas encore d'évaluation
- SPJ Kerja BaktiDocument54 pagesSPJ Kerja BaktiRafi IrvaPas encore d'évaluation
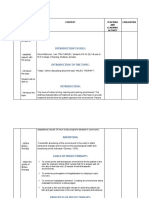
- Introduction To Self:: Time Specific Objective Content Teaching AND Learning Activity EvaluationDocument20 pagesIntroduction To Self:: Time Specific Objective Content Teaching AND Learning Activity EvaluationKiran Kour100% (2)
- Puerperal SepsisDocument45 pagesPuerperal SepsisKalo kajiPas encore d'évaluation
- CIA4001 - FE Answer Scheme - Sem2 - 20192020Document9 pagesCIA4001 - FE Answer Scheme - Sem2 - 20192020Divya TharshiniPas encore d'évaluation
- Root Cause Analysis Template 3Document14 pagesRoot Cause Analysis Template 3Timmo KekelwaPas encore d'évaluation
- Preterm Infant Growth Velocity Calculations - A Systematic ReviewDocument12 pagesPreterm Infant Growth Velocity Calculations - A Systematic ReviewLeonardo CardozoPas encore d'évaluation
- Swimming Is The Self-Propulsion of A Person Through WaterDocument3 pagesSwimming Is The Self-Propulsion of A Person Through WaterKryzler KayePas encore d'évaluation
- Dobutamine It Stimulates Heart Muscle and Improves Blood Flow by Helping The Heart Pump BetterDocument3 pagesDobutamine It Stimulates Heart Muscle and Improves Blood Flow by Helping The Heart Pump BetterJinky Nacar DomingoPas encore d'évaluation
- Female Incontinence: DR Alin CiopecDocument51 pagesFemale Incontinence: DR Alin CiopecalinciopecPas encore d'évaluation
- CPM UtiDocument21 pagesCPM UtiAgnes BastonPas encore d'évaluation
- Developing Bridging Leadership Capital WorksheetDocument1 pageDeveloping Bridging Leadership Capital WorksheetAlodia FarichaiPas encore d'évaluation
- SchizophreniaDocument14 pagesSchizophreniaapi-546705901Pas encore d'évaluation
- ORC ICF Audit Checklist Jan 2017Document6 pagesORC ICF Audit Checklist Jan 2017Ita afrika sariPas encore d'évaluation