Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Essential Neurology 4Th Ed PDFDocument290 pagesEssential Neurology 4Th Ed PDFPutu 'yayuk' Widyani WiradiraniPas encore d'évaluation
- Food and Drug InteractionsDocument4 pagesFood and Drug InteractionsClararida RiawanPas encore d'évaluation
- Coffee Basics - A Quick and Easy Guide - Kevin Knox Julie Sheldon HuffakerDocument226 pagesCoffee Basics - A Quick and Easy Guide - Kevin Knox Julie Sheldon HuffakerFernanda Campos100% (8)
- Cafe Coffee DayDocument47 pagesCafe Coffee DayJitender Singhal100% (6)
- Starbucks Organizational AnalysisDocument14 pagesStarbucks Organizational Analysispurelypisces83Pas encore d'évaluation
- Why Dunkin Donuts Is Taking On Starbucks and Betting On Coffee?Document2 pagesWhy Dunkin Donuts Is Taking On Starbucks and Betting On Coffee?kaikoPas encore d'évaluation
- Product Cataloque - 12Document14 pagesProduct Cataloque - 12Ahmed DhiebPas encore d'évaluation
- Acute Complication of Diabetes Mellitus: Laksmi SasiariniDocument43 pagesAcute Complication of Diabetes Mellitus: Laksmi SasiariniClararida RiawanPas encore d'évaluation
- Starbucks Case Study: How Big Data and AI Boost PerformanceDocument10 pagesStarbucks Case Study: How Big Data and AI Boost PerformanceS S DesaiPas encore d'évaluation
- Self - Assessmnet Guide Barista NC IIIDocument5 pagesSelf - Assessmnet Guide Barista NC IIIMac Dareel UrianoPas encore d'évaluation
- The Espresso Lane To Global Markets Case StudyDocument7 pagesThe Espresso Lane To Global Markets Case StudyDavid Alvarez Miranda100% (1)
- ND Terminology (Clinical Domain)Document1 pageND Terminology (Clinical Domain)Clararida RiawanPas encore d'évaluation
- Tinea Infection DX and Management BMJ 7 2012Document10 pagesTinea Infection DX and Management BMJ 7 2012AgaipPas encore d'évaluation
- Nfs Journal: Fangfang Song, Jieun Oh, Kyungwon Lee, Mi Sook ChoDocument6 pagesNfs Journal: Fangfang Song, Jieun Oh, Kyungwon Lee, Mi Sook ChoClararida RiawanPas encore d'évaluation
- Nfs Journal: Fangfang Song, Jieun Oh, Kyungwon Lee, Mi Sook ChoDocument6 pagesNfs Journal: Fangfang Song, Jieun Oh, Kyungwon Lee, Mi Sook ChoClararida RiawanPas encore d'évaluation
- Nfs Journal: Fangfang Song, Jieun Oh, Kyungwon Lee, Mi Sook ChoDocument6 pagesNfs Journal: Fangfang Song, Jieun Oh, Kyungwon Lee, Mi Sook ChoClararida RiawanPas encore d'évaluation
- Kuliah Hyper and Hypothyroid - 2014Document66 pagesKuliah Hyper and Hypothyroid - 2014Clararida RiawanPas encore d'évaluation
- Guideline Stroke Perdossi 2007Document15 pagesGuideline Stroke Perdossi 2007Saut 'tetZ' PurbaPas encore d'évaluation
- Guideline Stroke Perdossi 2007Document15 pagesGuideline Stroke Perdossi 2007Saut 'tetZ' PurbaPas encore d'évaluation
- Nfs Journal: Fangfang Song, Jieun Oh, Kyungwon Lee, Mi Sook ChoDocument6 pagesNfs Journal: Fangfang Song, Jieun Oh, Kyungwon Lee, Mi Sook ChoClararida RiawanPas encore d'évaluation
- Penatalaksanaan Hipertensi Pada Lanjut Us1a (DR Ra Tuty K)Document6 pagesPenatalaksanaan Hipertensi Pada Lanjut Us1a (DR Ra Tuty K)Ayu Isyana WardhaniPas encore d'évaluation
- 4572 14986 1 PBDocument21 pages4572 14986 1 PBSastra WijayaPas encore d'évaluation
- Water - The Component of FoodDocument25 pagesWater - The Component of FoodIndah RatnasariPas encore d'évaluation
- Pathophysiology of Muscle Dysfunction in COPDDocument13 pagesPathophysiology of Muscle Dysfunction in COPDClararida RiawanPas encore d'évaluation
- IFRJ 19 (03) 2012 AzharDocument6 pagesIFRJ 19 (03) 2012 AzharClararida RiawanPas encore d'évaluation
- Menu NLCDocument3 pagesMenu NLCClararida RiawanPas encore d'évaluation
- DM 2Document3 pagesDM 2Clararida RiawanPas encore d'évaluation
- Menu TugasDocument2 pagesMenu TugasClararida RiawanPas encore d'évaluation
- Pages From Volume2-6Document4 pagesPages From Volume2-6Clararida RiawanPas encore d'évaluation
- Early Registration Form NLT 2015Document4 pagesEarly Registration Form NLT 2015Clararida RiawanPas encore d'évaluation
- Low Gi.2015 PDFDocument27 pagesLow Gi.2015 PDFClararida RiawanPas encore d'évaluation
- Special Nutritional Concerns For The Female Athlete: Kathe A. Gabel, PHD, RD, LDDocument5 pagesSpecial Nutritional Concerns For The Female Athlete: Kathe A. Gabel, PHD, RD, LDClararida RiawanPas encore d'évaluation
- Journal 1Document4 pagesJournal 1Clararida RiawanPas encore d'évaluation
- Karavidas - 2010 - Aging and The Cardiovascular SystemDocument7 pagesKaravidas - 2010 - Aging and The Cardiovascular SystemFábio CahuêPas encore d'évaluation
- Adesso ManualDocument12 pagesAdesso ManualLeoPas encore d'évaluation
- Global Marketing Environment For Coffee ShopsDocument5 pagesGlobal Marketing Environment For Coffee ShopsAtiqah Ismail100% (1)
- Manual SIEMENS-EQ.7 PDFDocument116 pagesManual SIEMENS-EQ.7 PDFEugeniu StadnicPas encore d'évaluation
- English Practice Paper QuestionsDocument4 pagesEnglish Practice Paper QuestionsVenkataramana SridharPas encore d'évaluation
- Proposal For Launching A Tea Brand New Leaf: Marketing ManagementDocument21 pagesProposal For Launching A Tea Brand New Leaf: Marketing ManagementZeeshan BravePas encore d'évaluation
- Cafeit Business Plan for Mobile Coffee CartDocument15 pagesCafeit Business Plan for Mobile Coffee CartShane BagaporoPas encore d'évaluation
- ISM003 Sample Report (B)Document20 pagesISM003 Sample Report (B)Thomas NganPas encore d'évaluation
- Virtuoso Plus Overall DatasheetDocument11 pagesVirtuoso Plus Overall Datasheetapi-529798489Pas encore d'évaluation
- NutritionDocument34 pagesNutritionOluwachidiPas encore d'évaluation
- Facts About CoffeeDocument1 pageFacts About Coffeegeni1961Pas encore d'évaluation
- Anlamca en Yakın Cümleyi BulmaDocument7 pagesAnlamca en Yakın Cümleyi BulmamaliPas encore d'évaluation
- Group2 06TP1Document12 pagesGroup2 06TP1Sheila Mae Dinong BaresPas encore d'évaluation
- Mam Stepani MidDocument10 pagesMam Stepani MidanggiPas encore d'évaluation
- A Project Report: "Consumer Perception & Sales Promotion in Regard To Cafe Coffee Day New Delhi"Document9 pagesA Project Report: "Consumer Perception & Sales Promotion in Regard To Cafe Coffee Day New Delhi"shashankPas encore d'évaluation
- Spain CoffeeDocument8 pagesSpain CoffeeAlexandra Castro-SamsonPas encore d'évaluation
- Perancangan Ulang Tata Letak Fasilitas Di Café "Home 232" CinereDocument17 pagesPerancangan Ulang Tata Letak Fasilitas Di Café "Home 232" CinereRatna AzarinPas encore d'évaluation
- Packaging Unwrapped 2011Document48 pagesPackaging Unwrapped 2011Guillaume DryPas encore d'évaluation
- Café Mocha: Case StudyDocument25 pagesCafé Mocha: Case StudyAneesh BajajPas encore d'évaluation
- Storm in a Coffee Cup - The Barista StoryDocument23 pagesStorm in a Coffee Cup - The Barista StoryKuldip BarmanPas encore d'évaluation
- Social Media Audit AssignDocument4 pagesSocial Media Audit Assignbalvinder singhPas encore d'évaluation
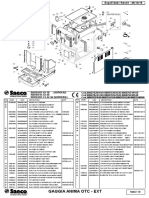
- Gaggia Anima Prestige Parts DiagramDocument8 pagesGaggia Anima Prestige Parts DiagramKanen Coffee, LLC.Pas encore d'évaluation
- Elektra Coffee GrinderDocument6 pagesElektra Coffee Grinderינון שיPas encore d'évaluation