Académique Documents
Professionnel Documents
Culture Documents
Uveitis Anterior PDF
Transféré par
Annisa RahmadhaniaTitre original
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Uveitis Anterior PDF
Transféré par
Annisa RahmadhaniaDroits d'auteur :
Formats disponibles
Background
T
wo cases of acute anterior
uveitis (AAU) are presented;
one involving a 24-year-old
Caucasian female, and the
other affecting a 48-year-old Hispanic
female. These cases cover one of the most
common forms of ‘red eye’ that prompts
patients to seek eye care urgently, and
illustrate the clinical decision-making
process arriving at the diagnosis and ap-
propriate management. The condition
Anterior Uveitis:
is relatively common, with many third-
and fourth-year optometry interns en-
countering it at least once during their
Teaching Case Reports clinical rotations. Thorough case histo-
ry, careful slit lamp biomicroscopy and
complete posterior segment examina-
Len V. Hua, PhD, OD, FAAO tion are essential to correctly diagnose
Lorne B Yudcovitch, OD, MS, FAAO and treat this ocular condition. In addi-
tion, lab testing, imaging and referral to
an internist and/or rheumatologist are
called for in some cases.
AAU is an acute intraocular inflamma-
tion of the iris and ciliary body due to
a breakdown in the blood-aqueous bar-
rier, leading to presence of “cells and
flare” in the anterior chamber (AC).1
Abstract The diagnosis of AAU is relatively
Acute anterior uveitis (AAU) is the most common form of intraocular inflam- simple due to the plethora of clinical
mation seen by eye care professionals that affects relatively younger patients, with symptoms, such as photobia and pain-
ful eye, and signs, such as limbal flush,
significant distress and potentially long-lasting sight-threatening complications.
posterior synechiae, and AC cells and
The diagnosis of AAU is relatively simple for clinicians because of multiple pre- flare observed on slit lamp biomicros-
senting signs and symptoms; however, the etiology is often much more difficult copy. In contrast, the challenge is in
to elucidate. Therefore, it is critical for interns and practicing clinicians to have determining the etiology because AAU
an extensive understanding of the pathogenesis of AAU. Judicious yet effective could be a result of trauma or iatrogenic
dosage of topical corticosteroid and cycloplegic agents are the mainstay of AAU sources, an infectious agent, medica-
treatment. Depending on the presentation and cause, other medications, lab tions, a systemic autoimmune condi-
tests and tertiary procedures may be necessary. Finally, coordination with other tion or idiopathic cause. Consequently,
specialists (i.e., ophthalmologists, rheumatologists) may be critical in diagnosis the differentials for the etiology of AAU
and treatment. Eye care providers play a key role in the interdisciplinary man- can be lengthy, and a thoughtful list of
questions is important in narrowing the
agement of the patient with AAU.
causative suspects. For instance, ques-
Key Words: Anterior uveitis, iritis, iridocyclitis, cells and flare, HLA-B27, tions related to recent soft contact lens
corticosteroids, cycloplegics wear, injury or ocular surgery can rule
out their corresponding association.
Whereas age-related macular degenera-
tion and glaucoma tend to affect older
patients, AAU is a condition that affects
Dr. Hua is an Assistant Professor at Pacific University College of Optometry and Chief of Medical relatively younger patients more fre-
Eyecare. He teaches pharmacology, biochemistry and ocular emergencies in addition to being an quently, with significant distress and po-
attending for primary care and ocular disease clinics.
tentially long-lasting sight-threatening
Dr. Yudcovitch is an Associate Professor at Pacific University College of Optometry and served for complications.2 Therefore, it is critical
several years as Clinic Director of the college’s Northeast and Southeast Eye Centers. He instructs
in ocular disease, therapeutics and patient care courses as well as in several clinic areas. for interns and practicing clinicians to
have an extensive understanding of the
pathogenesis of AAU and its prompt
and appropriate treatment, including
Optometric Education 92 Volume 36, Number 2 / Winter/Spring 2011
interdisciplinary co-management as in-
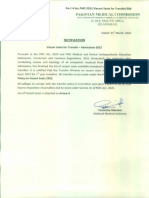
dicated. Figure 1A (Case 1)
Anterior uveitis OD with fibrous deposits on the lens
Student Discussion Guide
Case 1 description
A 24-year-old Caucasian female pre-
sented to the University Eye Clinic on
June 16, 2010 with a complaint of a red,
watery and painful right eye for about a
day. She also mentioned that this was
the third episode she had experienced
on an annual basis over the past three
years, with the past two episodes lasting
approximately 40 days with treatment.
Her medical history was unremarkable,
without any ocular injury or surgery. In
addition, she had denied any joint pain
or bowel disease when questioned. She
reported that her sister has an ‘eye turn’
and had been treated with an eye patch,
and that her maternal uncle was recently Figure 1B (Case 1)
diagnosed with glaucoma. She currently High magnification (40X) shows cells (representative
takes multivitamins and an oral contra- arrows) in the AC OD
ceptive. Her last eye exam two months
ago revealed normal exam findings.
At the current visit, her distance visual
acuity (VA) without correction was
20/20-1 OD and 20/20+1 OS. Both
eyes showed smooth, accurate, full and
equal extraocular muscle movements
in all fields of gaze. No pupillary de-
fect was observed, and no notable pho-
tophobia was reported in either eye.
Finger counting confrontation visual
fields were full OD and OS. Anterior
segment findings, as observed with bio-
microscopy, demonstrated 1+ circum-
limbal flush with trace cells and flare
OD (Figures 1A and 1B). Goldmann
applanation tonometry was 13 mmHg
OD and 14 mmHg OS at 10:48 a.m.
Dilated fundus examination showed
a normal retina with healthy maculae was recurrent, she was also referred for She was referred to a local rheumatol-
and vasculature and optic nerve cup-to- blood workup, human leukocyte anti- ogist-ophthalmologist for further con-
disc ratios of 0.45H /O.40V OU, with gen (HLA) testing and spinal X-ray to sultation. Her recent spinal X-ray and
healthy optic nerve head rims and dis- explore a possible systemic cause. A re- blood workup were normal, with the
tinct disc margins in both eyes. view of her chart records revealed that exception that she was HLA-B27 posi-
The patient was diagnosed with recur- her blood workup two years ago was tive. The specialist concluded that the
rent, but mild, acute anterior uveitis of normal. inflammation has affected only the pa-
her right eye and educated about her Follow-up # 1: June 23, 2010 tient’s eye so far, but in the future she
findings, prognosis and treatment op- will have a higher risk for arthritis, and
tions. She was treated with Pred Forte A week later, the patient felt that her that long-term nonsteroidal anti-in-
(PF; prednisolone acetate 1% ophthal- eye condition was slightly worse, al- flammatory drug (NSAID) treatment
mic suspension) igt q2h and homatro- though her VA was still 20/20-1 OD may be beneficial.
pine 5% (H) ophthalmic solution igt qhs and 20/20+1 OS. Moderate circumlim-
bal injection, 2+ cells and 2+ flare, was Case 2 description
OD. She was recommended to return
to clinic a week later, or sooner if her seen in the AC. The PF was increased to A 48-year-old Hispanic female pre-
symptoms get worse. Since the uveitis igt q1h OD and the H to igt bid OD. sented to the University Eye Clinic on
Feb 2, 2010 with a chief complaint of
Optometric Education 93 Volume 36, Number 2 / Winter/Spring 2011
painful red eye, severe photophobia
and tearing OD for the past few days. Figure 2A (Case 2)
She had tried an over-the-counter anti- Anterior uveitis OD with fibrous membrane and
allergy drop, but it did not help. Medi- posterior synechiae
cal history was positive for depression
and hand tremors, for which she had
been taking oral vitamin B6 and Flex-
eril (cyclobenzaprine), respectively. She
reported no joint/back pain and no
pain on urination or bowel movement.
Her last eye exam was many years ago,
and she reported no history of ocular
injury or surgery. Family medical his-
tory was negative for diabetes, hyper-
tension, glaucoma or blindness.
At the current visit, her uncorrected
distance VA was 20/150 OD and
20/150 OS, with pinhole improvement
to 20/60-2 OD and 20/60+1 OS. Both
eyes showed smooth, accurate, full and
equal extraocular muscle movements in
all fields of gaze. No afferent pupillary
defect was observed; however, the pa- Figure 2B (Case 2)
tient was photophobic in her right eye. Anterior uveitis OD. Fibrous membrane resolved with
Finger counting confrontation visual topical steroid treatment
fields were full OD and OS. Anterior
segment findings, as observed with bio-
microscopy, demonstrated 2+ circum-
limbal injection and 2+ cells in the AC
in the right eye. No vitreal cells or haze
were seen in either eye. Posterior poles
appeared normal OU with healthy mac-
ulae, vasculature, and cup-to-disc ratios
of O.30H/0.30V both eyes. Goldmann
applanation tonometry was 16 mmHg
OD and 15 mmHg OS at 5:46 p.m.
Acute anterior uveitis with posterior
synechiae OD was diagnosed, and the
patient was educated about her find-
ings, prognosis and treatment options.
She was treated with a prescription regi-
men of PF igt q1h OD and H bid OD.
The patient was recommended to return
to clinic the next day for follow-up.
contact tonometry was 10 mmHg OD and a rheumatological consult was also
Follow-up # 1: Feb 03, 2010 and 12 mmHg OS at 9:47 a.m. One recommended.
The patient reported slight improve- drop of phenylephrine 10% and one Follow-up # 2: Feb 05, 2010
ment in her comfort after taking the drop of atropine 1% were instilled in-
office to attempt to break the posterior The patient appreciated further im-
drops as prescribed, but she was still
synechiae. As before, no vitreal cells or provement over the next two days, al-
tearing and photophobic in her right
haze were seen OU. Posterior poles also though she still felt some discomfort
eye. Her uncorrected VA was worse at
were normal OU with healthy macu- and tearing. Her VA had improved to
20/400 OD and the same at 20/150
lae, vasculature, and cup-to-disc ratios 20/80-1 (pinhole 20/40+1) OD and
OS, but pinhole improved the VAs to
of O.30H/0.30V both eyes. was unchanged OS (20/150; pinhole
20/100- OD, 20/60 OS. Anterior seg-
20/60). Anterior segment findings, as
ment findings, as observed with biomi- The patient was instructed to continue observed with biomicroscopy, demon-
croscopy, demonstrated 2+ circumlim- the PF igt q1h OD and H igt bid OD strated mild circumlimbal injection, 1+
bal injection, 2+ cells and 3+ flare in and to return to clinic in two days. A cells and 1+ flare in the AC with poste-
the AC with posterior synechiae and fi- letter with request for a blood workup rior synechiae at 7 o’clock, and resolv-
brin membrane OD (Figure 2A). Non- was sent to her primary care provider, ing fibrin membrane OD (Figure 2B).
Optometric Education 94 Volume 36, Number 2 / Winter/Spring 2011
Noncontact tonometry was 12 mmHg had not filled her spectacle prescription and demographics
OD and 14 mmHg OS at 3:16 p.m. from the prior visit, and her VA was 6. Discuss the importance of the
The patient was instructed to continue still 20/80 (pinhole 20/40-1) OD and presence of HLA-B27
the PF igt q2h OD for two days and 20/100 (pinhole 20/50) OS. She was
educated on her recent uveitis condi- 7. Discuss systemic inflammatory
then taper to igt q4h OD for the sub- diseases that have high associa-
sequent three days, continue H igt bid tion and warned that it might recur in
the future. tion with AAU
OD, and to return to the clinic in five
days with her blood workup results. Key concepts 8. Describe the mechanisms of ac-
tion of drugs used in manage-
Follow-up # 3: Feb 10, 2010 1. Common etiologies of acute ante- ment of AAU
Five days later, the patient felt that her rior uveitis
9. Discuss the potential side-effects
symptoms were worse, with more pain 2. Thorough case history for patients of steroid use
and photophobia. Her VA was reduced with acute anterior uveitis
at 20/150 (pinhole 20/50) OD and B. Generating questions, hypothesis,
3. The use of epidemiology in differ- and diagnosis
20/200 (pinhole 20/60) OS. Anterior entiating possible causes
segment findings, as observed with bio- 1. What are important questions
microscopy, demonstrated moderate 4. Clinical findings in differential di- relevant to AAU?
circumlimbal injection, 2+ cells and 1+ agnosis of acute anterior uveitis
2. How is AAU diagnosed?
flare in the AC with posterior synechiae 5. Treatment of acute anterior uveitis
at 7 o’clock OD. Noncontact tonom- 3. What age group does AAU
4. The importance of patient educa- tend to affect?
etry was 10 mmHg OD and 15 mmHg
tion and regular follow-up
OS at 9:59 a.m. 4. What are the potential differ-
5. The essentials of appropriate sys- ential diagnoses?
The patient was advised to increase the
temic workup and specialist con-
PF to igt q2h OD and H bid OD. In 5. Why is pupil dilation neces-
sultations
addition, she was prescribed oral pred- sary?
nisone (60mg/day for one week). She Learning objectives
was also promptly referred to see a lo- 6. What laboratory tests are help-
1. To ask intelligent questions in help- ful in identifying the etiology?
cal rheumatologist. Her blood workup ing with differential diagnoses
there showed high white blood cell and 7. Is the diagnosis valid?
platelet counts, low hematocrit and 2. To understand the signs and symp-
toms of ocular inflammation C. Management
positive presence of HLA-B27.
3. To relate patient demographics to 1. What are the different topical
Follow-up # 4: Feb 17, 2010 corticosteroids available for
known epidemiology of the AAU
A week after the combined topical and ocular inflammation? How are
oral steroid treatment, the patient felt 4. To rule out posterior segment in- they ranked in terms of po-
much better, with only mild discom- volvement of ocular inflammation tency?
fort. Her VA was 20/80 (pinhole 20/40- 5. To provide appropriate patient ed- 2. Why are cycloplegics needed?
) OD and 20/150 (pinhole 20/50) OS. ucation and optimal medical man-
Refraction was performed, giving -3.00 agement 3. Should oral NSAIDs be used?
-1.00 x 164 to 20/25- OD and -2.50 6. To collaborate with other health 4. When is laboratory workup
-1.25 x 021 to 20/25 OS with near ad- care professionals in management advised?
dition of +1.50 OU. Anterior segment of possible systemic cause 5. What is the follow-up sched-
findings, as observed with biomicros-
Discussion questions ule?
copy, demonstrated mild circumlimbal
injection, with no cells and trace flare A. Knowledge, concepts, facts, infor- 6. What course of action is neces-
in the AC OD. mation required for critical review sary when symptoms get worse
of the cases with treatment?
The rheumatologist concluded that she
has HLA-B27-associated uveitis, and 1. Describe the signs and symptoms 7. When should the patient be
maintained her on oral steroid as pre- of anterior uveitis vs. other in- referred to a specialist?
scribed. She was recommended to taper flammation/injury 8. What specialists are indicated?
off her oral and topical steroid gradu-
2. Describe the different types of 9. Why is it necessary to taper the
ally over the next two weeks and to dis-
uveitis based on anatomy steroid?
continue the homatropine.
3. Discuss the cause of cells and D. Critically assessing implications,
Follow-up # 5: Mar 03, 2010
flare in the anterior chamber patient management and psycho-
At this visit (almost three weeks later), social issues
4. Discuss the risk factors for
the patient was off all prescribed uveitis
uveitis 1. What are the implications of
medication, and she felt that her eye
condition had completely resolved. She 5. Determine causality based on standard treatment vs. modi-
patient case history, risk factors fied/no treatment? Consider
Optometric Education 95 Volume 36, Number 2 / Winter/Spring 2011
cost, time, side-effects, con-
venience effect and quality of Table 1
life. Standardization of Uveitis Nomenclature (SUN) grading
2. What are the consequences as- system for AC cell and flare severity.2 The presence or
sociated with noncompliance absence of a hypopyon should be noted separately in
to the treatment plan? addition to the AC cellular activity grade.
3. What pertinent information
should be used to educate the Grade AC Cells (1 mm x 1 mm beam) AC Flare
patient about the condition? 0 None None
4. Discuss ways to respond to the 0.5+ 1-5 cells -
anxiety of the patient towards
future recurrence and progno- 1+ 6-15 cells Faint
sis with respect to the patient 2+ 16-25 cells Moderate (clear iris & lens)
and the patient’s family mem-
bers. 3+ 26-50 cells Marked (hazy iris & lens)
4+ >50 cells Intense (fibrin or plasmoid
Educator’s Guide aqueous)
The educator’s guide includes the nec-
essary information to discuss the case.
of the population.4 HLA-B27, a Class obvious. Ocular signs include anterior
Literature review I major histocompatibility complex chamber cells that slowly drift in the
The breakdown of blood-aqueous bar- (MHC), is a strong risk factor and as- aqueous humor. These anterior chamber
rier in the iris and ciliary body leads to sociated with up to half of all cases of cells should be differentiated regionally
clinical signs and symptoms of acute AAU.5 HLA-B27-positive AAU tends from cells in the vitreous, which would
anterior uveitis. It is the most common to be more severe in presentation and indicate an intermediate or posterior
form of intraocular inflammation seen earlier in onset than HLA-B27-negative uveitis. The clinician may often use
by eye care professionals.1 The leak- uveitis, affecting primarily younger pa- high magnification with a relatively
age of vascular contents into the ante- tients between 20 and 40 years of age.3 bright illumination upon biomicros-
rior chamber can be seen as “cells” and In addition, males are affected 2.5 times copy to visualize cells. The appearance
“flare” via slit lamp biomicroscopy. A more frequently than females in HLA- of cells in the AC is similar to seeing a
grading system was established by the B27-positive uveitis. The prevalence of few to numerous dust particles floating
Standardization of Uveitis Nomencla- the HLA-B27 gene varies among popu- and moving in empty space. Similarly,
ture (SUN) for clinical use (Table 1).2 lations, as high as 8% in Caucasians, bright illumination and magnification
Cells are predominantly white blood and as low as 0.5% in Japan.1,3 is often necessary to visualize flare,
cells (leukocytes) released in response A number of systemic inflammatory with conical beam illumination reveal-
to inflammation. Flare is comprised of diseases, such as ankylosing spondylitis ing a Tyndall effect (light scattering)
serum proteins: pro-inflammatory cy- (AS), Reiter’s syndrome and psoriatic from the suspended protein particles.
tokines and chemokines that selectively arthritis, have been known for decades Severe flare and inflammatory media-
recruit inflammatory white blood cells. to associate with HLA-B27 and AAU. tors released into the anterior chamber
Furthermore, flare can coalesce to form Particularly, 90% of patients with AS can rarely lead to a viscous ‘plasmoid’
fibrin, while white blood cells can pre- possess the HLA-B27 antigen.2, 6 aqueous and hypopyon. The corneal
cipitate in the corneal endothelium in endothelium may show adherent cells
certain forms of uveitis to form keratic Clinical features (both white blood cells and, less often,
precipitates (KPs). Therefore, the di- Acute anterior uveitis typically presents iris melanocytes) that predispose the in-
agnosis of AAU is relatively simple for with the patient experiencing hallmark ferior aspect of the cornea (Arlt’s trian-
clinicians because of multiple present- symptoms of recent onset eye pain (of- gle). Although the eye can appear white
ing signs and symptoms. However, the ten dull, aching pain) and photophobia. with uveitis, circumlimbal injection is
etiology is often much more difficult to Secondary symptoms include blurred a notable sign and, less often, a more
elucidate. vision, a watery/tearing eye, redness generalized conjunctival inflammation.
The annual incidence of uveitis has been and headache. One or both eyes may Posterior synechiae (iris adhesions, usu-
estimated to be about 35 per 100,000 be affected. Visual acuities may or may ally at the pupillary ruff, to the anterior
in the general population with a preva- not be reduced depending on severity lens capsule) are not uncommon with
lence of 0.5%.1 Of the uveitides catego- of the uveitis. Pupillary testing may anterior uveitis; one study found pos-
rized by anatomical location (anterior, show a sluggish pupillary constriction terior synechiae in half of 119 patients
intermediate, posterior, panuveitis) an- response to light, usually due to iris in- with acute anterior uveitis, regardless if
terior uveitis accounts for most of the flammation and/or iris synechial adhe- it was HLA-B27 positive or negative.7
cases seen clinically.3 The lifetime inci- sions. A direct and consensual eye pain A corectopia (irregularly shaped pupil)
dence of AAU may be as high as 0.2 % to light is highly specific to anterior can result from posterior synechiae, as
uveitis, even when other signs are not as well as later adhesion of pigment to the
Optometric Education 96 Volume 36, Number 2 / Winter/Spring 2011
anterior lens capsule in a circular pat-
tern corresponding to pupillary ruff Table 2
pigment (Vossius ring). A fibrin mem- Differential diagnoses for anterior segment
brane on the anterior lens capsule can inflammation
often remain from longstanding syn-
echiae. Extensive posterior synechiae AAU (iritis, iridocyclitis) Keratitis (infective, traumatic/toxic, contact lens
acute red eye)
can lead to circumferential adhesion to
the anterior lens capsule, leading to pu- Episcleritis/Scleritis
Lens-related (phacolysis/phacoanaphylaxis)
pillary block, a bowing forward of the
iris (iris bombé) from posterior aque- Acute angle closure glaucoma
Posterior segment disease (tumor, panuveitis)
ous entrapment, and highly-elevated
intraocular pressure (IOP). Peripheral Endophthalmitis (post operation, endogenous)
anterior synechiae (PAS), whereby the
peripheral iris tissue near the ciliary
body adheres to the anterior chamber
angle structures, is less common. Best the uvea. Photophobia, eye pain photokeratitis) from arc-weld flash-
observed via gonioscopy, these adhe- and reduced vision are usually very es or high altitude reflection sun/
sions can block the trabecular mesh- severe, with poorer prognosis for snow exposure, chemical insult, or
work, impeding aqueous outflow and long-term vision. from immune conditions (i.e., Thy-
potentially elevating the IOP. • Endophthalmitis, a true eye emer- geson’s superficial punctuate kerati-
gency involving inflammation of tis). Infective keratitis may be bac-
Differential diagnoses terial, viral, fungal, acanthamoebic,
the vitreous and aqueous humor,
The common differential diagnoses for may present with symptoms of or chlamydial/parasitic. Light sen-
AAU are summarized in Table 2, and blurred vision, eye pain and red- sitivity, redness, pain, and reduced
some of the more serious conditions are ness and light sensitivity, simi- vision with any of these forms of
discussed. lar to AAU. However, history is keratitis can mimic AAU. It is also
• Intermediate/posterior/panuveitis an important differential, as en- possible that an anterior uveitic
are conditions whereby uveal in- dophthalmitis can be a rare endog- response is seen accompanying an
flammation has progressed beyond enous (causative source is within infective keratitis, so treatment of
the iris tissue. The sign of cells and/ eye) complication from ocular both conditions may be warranted.
or inflammatory exudates in the infection after surgical procedures Treatment of the non-infective ker-
vitreous is a key finding with these such as cataract extraction and vit- atitis may be similar to treatment
uveitides, and vitreal haze is often reoretinal surgeries.9,10 Exogenous of AAU (i.e., topical steroid and
present. Because constant fluid ex- (source is from outside the eye) en- cycloplegic agents). With infective
change in the vitreous does not oc- dophthalmitis may result from in- keratitis, however, care must be tak-
cur as it does in the aqueous, the fection spread from another source en to determine the specific caus-
cells and inflammatory byproducts (i.e., endocarditis). Endophthalmi- ative organism, as topical steroids
persist and move with gravity to tis may also occur from penetrating have the potential reduce wound
settle in the inferior retina (called eye injury or ocular surgery and, in healing and the body’s immune re-
‘snowbanking’) along the pars pla- very rare instances, be due to un- sponse to fight the infection. This is
na. This condition of intermediate known causes or present as a sterile especially true of herpetic epithelial
uveitis is called pars planitis, and is inflammation from retained lens keratitis, where topical steroid use
more common in younger individ- material after an operation or from may worsen the condition. Patients
uals, with a mean age of 30.7 years toxic agents.11 Usually along with with herpetic keratitis (particularly
(± 15.1 years). Over two-thirds of similar symptoms, a layer of white herpes zoster infection) may pres-
intermediate uveitis cases are idio- blood cells may be seen settled in ent with acute pain, redness and
pathic, with sarcoidosis, multiple the inferior anterior chamber (hy- light sensitivity, and the clinician
sclerosis (MS) and Lyme disease popyon). Immediate referral for must look closely for signs of den-
being the relatively less common a vitreal tap and culturing/sensi- dritic lesions, pustules and rashes
causes.8 Posterior uveitis may pres- tivities is indicated for endophthal- that may identify herpetic infec-
ent with macular edema, chorioret- mitis, with subsequent pars plana tion. Fluorescein sodium and rose
inal inflammation, retinal vasculi- vitrectomy and fortified topical, Bengal stain assessment are critical
tis and optic disc edema. Vitreal intravitreal and systemic antibiotic to ruling-out herpetic lesions on
haze may also accompany posterior treatment.12,13 the cornea. Fluorescein staining
uveitis. While photophobia may be may also reveal epithelial defects,
• Keratitis can present with similar infiltrates and ulcers due to other
reduced in posterior uveitis (due to symptoms to AAU, and the causes
less inflammation of the irides), vi- organisms. The presence of mu-
of keratitis may be non-infective or copurulent discharge is a diagnostic
sual blur is usually more severe and infective in etiology. Non-infective
prognosis of visual recovery poorer. sign of bacterial or chlamydial in-
keratitis may be due to external fection. While untreated bacterial
Panuveitis involves all regions of sources such as ultraviolet light (i.e.,
Optometric Education 97 Volume 36, Number 2 / Winter/Spring 2011
and chlamydial corneal infections
usually worsen over several hours to Table 3
a few days, fungal and certain acan- Cycloplegic agents, their concentrations, maximal effect
thamoebic infections may progress and duration of action in healthy eyes
more slowly, with progression over
a week or more after initial inocu- Cycloplegic Agent Maximal Effect (min) Duration of Action
lation not uncommon. History of Tropicamide 0.5, 1% 20-30 3 hours
soft contact lens wear, old makeup Cyclopentolate 1, 2% 20-45 1 day
use, water-based activities (i.e.,
Homatropine 2, 5% 20-90 2-3 days
swimming, hot tub) and vegeta-
Scopolamine 0.25% 4-7 days
tive injury are important in deter- 20-45
mining the diagnosis. Treatment of Atropine 0.5, 1, 2% 30-40 1-2 week(s)
infective keratitis is dependent on
the causative organism, and typi-
cally involves topical antibiotics Figure 3
(bacterial), oral antibiotics (chla- The cellular inflammatory pathway (enzymes labeled
mydial), topical and oral antivirals in bold), with points of inhibition by corticosteroids and
(herpetic), antimycotics (fungal) or
antiamoebics (acanthamoeba). NSAIDs (nonsteroidal anti-inflammatory drugs) shown
(adapted from Samiy N et al., 1996)14
• Patients with acute angle closure can
present similar symptoms to AAU,
including pain, blurred vision, ha-
los vision, frontal headache, nausea
and vomiting. Circumlimbal flush
and corneal edema is often seen.
Intraocular pressure (IOP) spike
is an important sign to differenti-
ate acute angle closure from AAU;
however, the patient may have an
IOP spike secondary to iris bombé
caused by AAU. The main approach
to management of acute angle clo-
sure is to reduce the IOP as quickly
as possible with topical, and often stabilizing the blood-aqueous bar- (alpha receptor) agonist used for
oral, glaucoma medications. rier by decreasing the iris surface assisting with the dilation of the
area (preventing further cellular and pupil. It is used in-office with a cy-
Treatment options for acute anterior cloplegic agent for breaking recal-
exudative leakage). The main cy-
uveitis citrant posterior synechiae. Usually
cloplegic agents (listed from short-
Management of AAU is focused on 1) est maximal effect time/duration to only one or two drops are instilled
reducing the inflammation and any as- longest) are listed in Table 3. The in the affected eye to facilitate di-
sociated pain, redness, photophobia most popular agents used in AAU lation. The drug also assists in fa-
and visual blur; and 2) determining the treatment are homatropine 5% cilitating view of the vitreous and
etiology. The first step is achieved by (trade name: Isopto-Homatropine retina, to determine if there is any
several treatments: 5%; typical dosage igt q12hr) and posterior segment inflammation.
• Sun protection scopolamine 0.25% (trade name: • Corticosteroids
Isopto-Hyoscine; typical dosage igt
The patient with AAU has usu- q6hr). Atropine (trade name: Isop- Corticosteroids are critical in the
ally determined that avoidance of to-Atropine 1%; typical dosage igt treatment of uveitides, including
bright light is to their immediate q12hr) is used in more severe cases. AAU. They reduce pain (includ-
benefit. Encouragement of sun- Even though a cycloplegic’s dura- ing photophobia), inflammation
glasses, a brimmed hat, staying in- tion of action is relatively long in (of most ocular tissues) and redness
doors more frequently and lowered healthy eyes, the duration of action (of conjunctiva, episclera, limbus).
lighting levels are good behavioral may be much shorter in uveitis due Corticosteroids block the enzyme
modifications during the acute to the presence of increased esteras- phospholipase A2 (which converts
symptomatic stage. es in the AC of a uveitic eye; hence cell membrane phospholipids into
• Cycloplegics more frequent dosing is needed. inflammatory mediators such as leu-
kotrienes and prostaglandins). This
Cycloplegic agents are important • Mydriatics inflammatory pathway is seen in Fig-
for relaxing the iris (for comfort), Phenylephrine 2.5% or 10% (trade ure 3.14 Topical ophthalmic steroid
breaking posterior synechiae, and name: AK-Dilate) is an adrenergic drops can be divided into 3 main cat-
Optometric Education 98 Volume 36, Number 2 / Winter/Spring 2011
egories, based on clinical potency: tion with one or more antibiotics) • Osteoporosis
Minimally effective: are also available for evening use. • Growth suppression
Risks of topical corticosteroids in- • Reduced immunity (infec-
• dexamethasone sodium tions)
phosphate 0.05% oint- clude posterior subcapsular cataract
(PSC) formation and elevated IOP. • Hypothalamus-Pituitary-Ad-
ment renal (H-P-A) axis suppression
• loteprednol 0.2% (trade Usually these risks are minimal due
to the short-term use of steroids • Menstruation problems
name: Alrex)
in AAU treatment. Prednisolone Because of these risks, the use of
Moderately effective: acetate has a higher propensity to oral steroids should be weighed
• prednisolone phosphate elevate IOP. Studies have shown with the potential side-effects.
0.125%, 0.5%, 1% solu- lotoprednol 0.5% (Lotemax) to be • NSAIDs
tions comparable to prednisolone acetate
• fluorometholone 0.1% 1% in effectively reducing ante- Both oral and topical ophthalmic
(trade name: FML Mild), rior uveitis, yet not elevating IOP non-steroidal anti-inflammatory
0.25% (trade name: FML as much as prednisolone acetate.18 drugs (NSAIDs) have limited ef-
Forte) Other risks of topical steroid use fectiveness in treating active AAU,
• rimexolone 1% ( trade include reduced host immunity, as their mechanism of action in-
name: Vexol) stromal melt, scleral thinning and hibits the enzyme cyclo-oxygenase
herpetic epithelial infection spread. (which produces prostaglandins)
Maximally effective: but not the enzyme phospholipase
In certain recalcitrant uveitis cases, A2 (which produces leukotrienes,
• loteprednol 0.5% (trade
or when the patient is unable to responsible for attracting white
name: Lotemax; combined
properly instill eyedrops or oint- blood cells into the anterior cham-
with tobramycin in Zylet)
ment, injectable steroids may be ber via chemotaxis). However, one
• dexamethasone 0.1%
indicated. These include regional study showed a 66.8% reduction
(combined with tobramy-
subconjunctival or sub-Tenons in- in recurrences of HLA-B27-asso-
cin in TobraDex)
jections of triamcinolone or dex- ciated uveitis over a 3-year period
• 1% prednisolone acetate
amethasone, as well as intravitreal with chronic oral NSAID use.20
(trade name: Pred Forte)
injections of each drug (Triesence;
• difluprednate 0.05% • Immunomodulators
Alcon Laboratories) or implants
emulsion (trade name:
(Ozurdex; Allergan Inc.), respec- In cases of non-infectious AAU
Durezol)
tively. Fluocinolone acetate intra- that is recalcitrant or non-respon-
All topical ophthalmic steroid eye vitreal implant (Retisert; Bausch + sive to steroid treatment, immuno-
drops (except for the solution pred- Lomb) is also an option in recurrent modulation may be necessary. The
nisolone phosphate and emulsion uveitides unresponsive to other ste- effectiveness of these medications
diflurprednate) are formulated as roid treatments. Unfortunately, the with uveitis has been demonstrated
suspensions. As such, the patient risk of elevated IOP and cataract in several cases.21,22 These consist of
must shake the bottle vigorously with these routes of administration immunosuppressants and biolog-
before instilling the drop onto the is much higher.21 ics. The three main immunosup-
eye, to provide a homogenous sus- pressant drug categories are:
• Oral steroids such as prednisone
pension of medication. The most
(Orasone, Deltasone, Meticorten, • Antimetabolites (methotrex-
popular steroid prescribed for AAU
Sterapred, other trade names) and ate, mycophenolate, azathio-
is Pred Forte (prednisolone 1%; igt
methylprednisone (Medrol, other prine)
q2hr); its generic version has been
trade names) are indicated when • T-cell suppressors, aka calcineu-
found to be less homogenous in
an AAU is severe or when posterior rin inhibitors (cyclosporine,
formulation, with more shakes re-
ocular involvement is seen. Typi- voclosporin, tacrolimus)
quired for the drug to go into sus-
cal adult dosage is 1mg/kg body • Cytotoxic agents, aka alkylat-
pension.15, 16 A more recent steroid
weight, with taper upon improve- ing agents (cyclophosphamide,
on the market, difluprednate (Du-
ment and dependent on duration chlorambucil)
rezol) was shown to be as effective
of treatment (longer tapers with
as Pred Forte, yet with only half the Biologics, a relatively newer class
longer treatments). Along with
dosage of Pred Forte.17 All steroids of drugs, are comprised of recom-
increased IOP and posterior sub-
used over the course of a week or binant cytokines and monoclonal
capsular cataract risk, several other
more are usually tapered gradually antibodies directed against selected
potential side-effects include, but
upon improvement of signs and cell-surface markers.23 The main
are not limited to:
symptoms, and then discontinued. biologics are:
If symptoms recur, the steroid’s • Hypertension
• Tumor necrosis factor-alpha
original dosage (or more frequent • Hyperglycemia
inhibitors (infliximab, adali-
dosage) is re-initiated. Several ste- • Psychosis
mumab)
roid ointments (most in combina- • Edema (Cushing’s Syndrome)
• Anti-lymphocyte drugs (ritux-
Optometric Education 99 Volume 36, Number 2 / Winter/Spring 2011
imab, alemtuzumab)
• Interleukin-2 receptor blocker Table 4
(daclizumab) Common causes of acute and chronic anterior uveitis
• Recombinant interferon-alpha (adapted from McCannel et al., 1996)4
Both immunosuppressants and biolog-
Acute Anterior Uveitis Chronic Anterior Uveitis
ics often take several weeks to achieve
efficacy. HLA-B27 positive (uveitis only) Juvenile idiopathic arthritis (JIA)
Ankylosing spondylitis Fuch’s heterochromic iridocyclitis
• Surgery Reactive arthritis (Reiter’s) Idiopathic
Psoriatic arthropathy Sarcoidosis
Surgical treatment for AAU is rare HLA-B27 negative (idiopathic) Syphilis
and only indicated in severe cases Sarcoidosis Lupus
Behcet’s disease Herpes (zoster/simplex)
where secondary complications Posner-Schlossmann Syndrome
arise. Permanent structural changes Crystalline lens-associated
from uveitis that may require sur- Syphilis
Lupus
gical management include cataract Trauma
formation, secondary glaucoma
due to pupillary block or angle clo-
sure, and retinal detachment. Sur- Table 5
gical indications include restoring Review of systems via history with uveitis-associated
visual clarity, diagnostic biopsy, or diseases (adapted from Cheng et al., 2005 and
removing media opacities to moni-
Gutteridge et al., 2007)3,27
tor the posterior segment. Surgi-
cal procedures include, but are System Diseases
not limited to: extracapsular pha- Dermatological Psoriasis, syphilis, sarcoidosis, lupus, herpes simplex/zoster,
coemulsification/cataract extrac- Behcet’s disease
tion, iridotomy/iridectomy, filter- Gastrointestinal Inflammatory bowel disease
ing surgeries, vitrectomy and other Genito-urinary Reiter’s syndrome, Behcet’s disease, syphillis
corneal and retinal procedures. Respiratory Sarcoidosis, tuberculosis
Rheumatological Spondyloarthropathies (eg., alkylosing spondylitis)
Discussion
Uveitis is an inflammatory disease of
the eye, potentially responsible for up Table 6
to 20% of all blindness.24 The Intern- Systemic diseases with uveitis association and
tational Uveitis Study Group (IUSG)
and Standardization of Uveitis nomen- corresponding lab tests (adapted from Cheng et al., 2005)3
clature (SUN) Working Group have Diseases Clinical Features Laboratory tests
adopted a classification of uveitis ac- HLA-B27 positive Uveitis only HLA-B27
cording to anatomical location: ante-
Ankylosing spondylitis Lower back pain, worse in a.m. HLA-B27, ESR, spinal X-ray
rior (anterior chamber), intermediate
(ciliary body, vireous), and posterior Reiter’s syndrome Triad: arthritis, urethritis and HLA-B27, ESR, ANA
conjunctivitis
(retina, choroid), with panuveitis in- Arthritis, psoriasis joint pain, skin inflammation HLA-B27, joint X-rays
volving all locations.25,26 Acute anterior
Inflammatory bowel disease Bloody diarrhea & abdominal cramp HLA-B27, endoscopy
uveitis (AAU) is an ocular presenta-
tion that has many potential etiologies. Behcet’s disease Aphthous mouth/genital ulcers HLA-B5
Identification of the key clinical find- Multiple sclerosis Optic neuritis, CNS plaques Cranial MRI, HLA-DR2
ings of AAU – cells and flare – along Sarcoidosis African ethnicity, shortness of breath, ACE, lysozyme, chest X-ray,
skin nodules gallium scan, biopsy
with the accompanying symptoms of
pain and photophobia - has been docu-
mented in the literature for over half
a century.27 While the most common spondylitis and other connective tissue tion. Less common potential infective
etiology of anterior uveitis is idiopathic disorders, questions regarding joint and etiologies include syphilis, tuberculosis,
(38-70%), the next most-common eti- back problems, pain on urination or toxoplasmosis and Lyme disease.4 Table
ology is HLA-B27-positive, particu- stomach irritation, arthritis, or other 4 summarizes the common causes of
larly with acute-onset forms.4 HLA- autoimmune diseases (i.e., Reiter’s syn- acute and chronic anterior uveitis.
B27 is present in 1.4-8% of the general drome, inflammatory bowel disease,
psoriatic arthritis, and post-infectious The management of uveitis is strongly
population; however, it can be present achieved through an evidence-based
in between 50-60% of patients with arthritis) should be asked in the his-
tory, along with the patient’s current approach. No standard laboratory
AAU.3 Since HLA-B27-positive re- evaluation for uveitis exists, except for
sults are strongly related to ankylosing medication list. Other causes of AAU
may include trauma and herpetic infec- determining syphilis and possibly sar-
Optometric Education 100 Volume 36, Number 2 / Winter/Spring 2011
coidosis-based etiologies. In addition, B-27 2. Bloch-Michel E, Nussenblatt RB.
many laboratory tests have false-neg- Some lab tests, such as complete blood International Uveitis Study Group
ative or false-positive results that may count (CBC), erythrocyte sedimenta- recommendations for the evalu-
potentially confuse the clinical picture tion rate (ESR), and rheumatoid fac- ation of intraocular inflamma-
and/or contribute to erroneous diag- tor (Rf ), have been regarded as too tory disease. Am J Ophthalmol.
noses, along with an additional cost non-specific for diagnostic purposes in 1987;103:234-235.
burden.28 Careful history and physical anterior uveitis, and only play only an 3. Chang JH, McCluskey PJ, Wake-
examination related to the review of adjunct role in certain cases.32 The clini- field D. Acute anterior uveitis
systems (i.e., dermatologic, hemato- cian must balance the diagnostic value and HLA-B27. Surv Ophthalmol.
logic, respiratory, circulatory, neuro- with cost-effectiveness when ordering 2005;50:364–388.
logical, ear/nose/throat, constitutional, laboratory tests (Table 6).
etc.) often is more valuable to deter- 4. McCannel CA, Holland GN, Helm
mining the cause of the uveitis (Table CJ, Cornell PJ, Winston JV, Rim-
Conclusion mer TG. Causes of uveitis in the
5).29 Physical signs such as the presence
or absence of granulomatous nodules This article highlights two cases of acute general practice of ophthalmology.
or keratic precipitates (KPs) also assist anterior uveitis (AAU), their clinical UCLA Community-Based Uveitis
in discriminating autoimmune (i.e., management and course. While the Study Group. Am J Ophthalmol.
sarcoid, systemic lupus erythematosis) hallmark signs and symptoms of AAU 1996;121:35–46.
from non-autoimmune-based uveitis.30 are highly diagnostic, the pathogenesis 5. Chang JH, McCluskey P, Wakefield
and etiology may be elusive. A careful D. Expression of toll-like receptor
When AAU is severe, unresponsive to evidence-based methodology, including
treatment, persists or recurs, labora- 4 and its associated lipopolysaccha-
detailed case history and review of sys- ride receptor complex by resident
tory testing may be necessary (Table 6). tems, physical examination and poten-
Minimum lab tests (with key identifi- antigen-presenting cells in the hu-
tial laboratory testing, is necessary for man uvea. Invest Ophthalmol Vis
able disease examples in brackets) may effective diagnosis and management.
include: HLA-B27 (ankylosing spon- Sci. 2004;45:1871–1878.
Treatment is initially focused on reduc-
dylitis), urinalysis (psoriatic arthritis), ing the inflammatory findings, with the 6. Brewerton DA, Hart FD, Nicholls A,
angiotensin converting enzyme (ACE) goals of improving patient comfort and Caffrey M, James DC, Sturrock RD.
(sarcoidosis), venereal disease research visual function. Once a more detailed Ankylosing spondylitis and HLA-
laboratory aka VDRL and fluorescent etiology of the AAU is determined, B27. Lancet. 1973;1:904–907.
treponemal antibody aka FTA-ABS treatment is then also geared towards 7. Linssen A, Meenken C Outcomes of
(syphilis) and chest X-ray (tuberculosis, the cause. HLA-B27-positive and HLA-B27-
sarcoidosis). In certain cases, anterior
Throughout the care of the patient negative acute anterior uveitis. Am
chamber or vitreal taps, culture swabs
with AAU, it is important to educate J Ophthalmol. 1995;120(3):351-
or tissue biopsies may be indicated. One
the patient thoroughly regarding his/ 61.
clinical study made evidence-based rec-
ommendations for appropriate tests in her condition, the possible causes and 8. Rodriguez A et al. Referral pat-
four anterior uveitis situations:31 prognosis. Following this, discussion of terns of uveitis in a tertiary eye
the various treatment options and ini- care center. Arch Ophthalmol.
• Non-granulomatous anterior tiation of treatment should begin im- 1996;114(5):593-9.
uveitis in an adult: HLA-B27 mediately, with close monitoring (i.e.,
daily or every few days, depending on 9. Taban M, Behrens A, Newcomb
o If recurrent or chronic: chest
the severity of the presentation). Judi- RL. Acute endophthalmitis follow-
X-ray, VDRL and FTA-ABS
cious yet effective dosage of topical cor- ing cataract surgery: a systematic
• Granulomatous anterior uveitis in review of the literature. Arch Oph-
an adult: chest X-ray, purified pro- ticosteroid and cycloplegic agents are
the mainstay of AAU treatment. De- thalmol. 2005;123(5):613-20.
tein derivative (PPD) tuberculin
pending on the presentation and cause, 10. Lundstrom M, Wejde G, Stenevi
testing, serum ACE levels, VDRL
other medications, lab tests and tertiary U, Thorburn W, Montan P. En-
and FTA-ABS
procedures may be necessary. Finally, dophthalmitis after cataract sur-
• Granulomatous anterior uveitis, coordination with other specialists (i.e., gery: a nationwide prospective
suspected sarcoidosis, in an adult ophthalmologists, rheumatologists) study evaluating incidence in rela-
or child: chest X-ray, ACE may be critical in diagnosis and treat- tion to incision type and location.
o If suspicion is high despite ment. Eye care providers play a key role Ophthalmology. 2007;114(5):866-
these tests normal: High-reso- in the interdisciplinary management of 70.
lution computerized tomogra- the patient with AAU. 11. Zhang Y, Zhang MN, Jiang CH,
phy (HRCT) scan of the chest Yao Y, Zhang K. Endophthalmitis
or whole body gallium scan References following open globe injury. Br J
with or without biopsy 1. Chang JH, Wakefield D. Uveitis: a Ophthalmol. 2010;94:111-114.
• Anterior uveitis in a child: Anti- global perspective. Ocular Immu- 12. Ng JQ, Morlet N, Pearman JW,
nuclear antibody (ANA), HLA nol Inflamm. 2002;10:263–279. Constable IJ, McAllister IL, Kenne-
Optometric Education 101 Volume 36, Number 2 / Winter/Spring 2011
dy CJ. Management and outcomes 21. Walton RC, Nussenblatt RB, Whit- uveitis investigation by Canadian
of postoperative endophthalmitis cup SM. Cyclosporine therapy for ophthalmologists. Can J Ophthal.
since the endophthalmitis vitrec- severe sight-threatening uveitis in 2008;43(6):652-657.
tomy study: the Endophthalmitis children and adolescents. Ophthal-
Population Study of Western Aus- mology. 1998;105(11):2028-34.
tralia (EPSWA)’s fifth report. Oph- 22. Huang JJ. Alternatives for long-
thalmology. 2005; 112(7):1199- term immunomodulation. Glau-
206. coma Today. 2010;8(12):46-48.
13. Endophthalmitis Vitrectomy Study 23. Imrie FR, Dick AD. Biologics in
Group. Results of the Endophthal- the treatment of uveitis. Curr Opin
mitis Vitrectomy Study. A random- Ophthalmol. 2007;18(6):481-6.
ized trial of immediate vitrectomy
and of intravenous antibiotics for 24. Suttorp-Schulten MS, Rothova A.
the treatment of postoperative bac- The possible impact of uveitis in
terial endophthalmitis. Arch Oph- blindness: a literature survey. Br
thalmol. 1995;113(12):1479-96. J Ophthalmol. 1996;80(9):844-
848.
14. Samiy N, Foster CS. The role of
non-steroidal anti-inflammatory 25. Jabs DA, Nussenblatt RB, Rosen-
drugs in ocular inflammation. Int baum JT. Standardization of Uveitis
Ophthalmol Clin. 1996;36:195- Nomenclature (SUN) Working
206. Group. Standardization of uveitis
nomenclature for reporting clinical
15. Fiscella, R.G., Jensen, M. & Van data. Results of the First Interna-
Dyck, G. Generic prednisolone tional Workshop. Am J Ophthal-
suspension substitution. Arch mol. 2005;140:509-516.
Ophthal. 1998;116:703.
26. Robert H Janigian Jr, MD Uveitis,
16. Calvin W. Roberts, Peter L. Nelson. Evaluation and Treatment. Web ar-
Comparative analysis of predniso- ticle. www.emedicine.
lone acetate suspensions. J Ocular com. Accessed on Feb 10, 2010.
Pharm Ther. 2007;23(2):182-187.
27. Hogan MR, Kimura SJ, Thygeson
17. DaVanzo RJ. Durezol™ compared P. Signs and symptoms of uveitis:
to Pred Forte® in the treatment of I. Anterior uveitis. Am J Ophthal-
endogenous anterior uveitis. Poster mol. 1959;47:162-3.
D1106, program 2697. ARVO
Annual Meeting; May 4, 2009; 28. Sandler G. The importance of the
Ft.Lauderdale,FL. history in the medical clinic and
the cost of unnecessary tests. Am
18. Controlled evaluation of lotepred- Heart J. 1980;100(6 Pt 1):928-31.
nol etabonate and prednisolone ac-
etate in the treatment of acute ante- 29. Gutteridge IF and Hall AJ. Acute
rior uveitis. Loteprednol Etabonate anterior uveitis in primary care.
US Uveitis Study Group. Am J Clin Exp Optom. 2007; 90(2):70-
Ophthalmol. 1999;127(5):597-9. 82.
19. Goldstein DA, Godfrey DG, Hall 30. Sinha R, Naithani P, Satpal G.
A, Callanan DG, Jaffe GJ, Pearson Newer investigations and manage-
PA, Usner DW, Comstock TL. In- ment guidelines in uveitis. Indian J
traocular pressure in patients with Ophthalmol. 2010; 58(1):88–91.
uveitis treated with fluocinolone 31. Forooghian F, Gupta R, Wong DT;
acetonide implants. Arch Ophthal- Derzko-Dzulynsky L. Anterior
mol. 2009;127(1):115-6. uveitis investigation by Canadian
20. Teasley LA, Ahmed M, Androudi ophthalmologists: insights from the
S, et al. Oral non-steroidal anti-in- Canadian National Uveitis Survey.
flammatory drug therapy for HLA- Can J Ophthal. 2006;41(5):576-
B27 positive patients with chronic 83.
non-infectious uveitis. ARVO; 32. Noble J, Hollands H, Forooghian
May 1-5, 2005; Fort Lauderdale, F, Yazdani A, Sharma S, Wong DT,
Florida. Abstract 2831. Derzko-Dzulynsky L. Evaluating
the cost-effectiveness of anterior
Optometric Education 102 Volume 36, Number 2 / Winter/Spring 2011
Vous aimerez peut-être aussi
- Textbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyD'EverandTextbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyPas encore d'évaluation
- Volume 35 Number 3 Article3Document8 pagesVolume 35 Number 3 Article3Rita HastaPas encore d'évaluation
- Management of Prosthetic Valve Endocarditis: A Clinical ChallengeDocument2 pagesManagement of Prosthetic Valve Endocarditis: A Clinical Challengedr yasminPas encore d'évaluation
- HenderlyDocument6 pagesHenderlymeenali karnPas encore d'évaluation
- Gastric PerforationDocument5 pagesGastric PerforationReyhan AristoPas encore d'évaluation
- Gastric Perforation by A Ventriculoperitoneal Shunt in An AdultDocument5 pagesGastric Perforation by A Ventriculoperitoneal Shunt in An AdultStereo PodPas encore d'évaluation
- Gastric Perforation by A Ventriculoperitoneal Shunt in An AdultDocument5 pagesGastric Perforation by A Ventriculoperitoneal Shunt in An AdultStereo PodPas encore d'évaluation
- 01 Cir 15 6 814Document13 pages01 Cir 15 6 814Niarti Ulan SariPas encore d'évaluation
- January 2018 Ophthalmic PearlsDocument3 pagesJanuary 2018 Ophthalmic Pearlsaswad 0008Pas encore d'évaluation
- Wong 2020Document5 pagesWong 2020samPas encore d'évaluation
- IMP Shock Etiol 5y Outcome VA-ECMO Edit 2023Document3 pagesIMP Shock Etiol 5y Outcome VA-ECMO Edit 2023vladbvs16Pas encore d'évaluation
- Rotator Cuff Tendinopathy:subacromial Impingement Syndrome - Is It Time For A New Method of Assessment?Document6 pagesRotator Cuff Tendinopathy:subacromial Impingement Syndrome - Is It Time For A New Method of Assessment?杨钦杰Pas encore d'évaluation
- Rotator Cuff Tendinopathy/subacromial Impingement Syndrome: Is It Time For A New Method of Assessment?Document6 pagesRotator Cuff Tendinopathy/subacromial Impingement Syndrome: Is It Time For A New Method of Assessment?Rilind ShalaPas encore d'évaluation
- Point of Care Ultrasound: The Critical Imaging Tool For The Critically UnwellDocument10 pagesPoint of Care Ultrasound: The Critical Imaging Tool For The Critically UnwellOswaldo OrtizPas encore d'évaluation
- Retinal ManifestationsDocument3 pagesRetinal ManifestationsFerdyPas encore d'évaluation
- Diagnostic Evaluation of Stroke Etiology: Review ArticleDocument13 pagesDiagnostic Evaluation of Stroke Etiology: Review Articleveerraju tvPas encore d'évaluation
- 01 Cir 98 25 2936Document13 pages01 Cir 98 25 2936Ikhsan Amadea9969Pas encore d'évaluation
- Antireflux Surgery Lich-GregoirDocument16 pagesAntireflux Surgery Lich-GregoircristiangelsPas encore d'évaluation
- Juvenile Cataract in Association With Tuberous Sclerosis ComplexDocument6 pagesJuvenile Cataract in Association With Tuberous Sclerosis ComplexAnonymous argZ1ZPas encore d'évaluation
- Latest Development in PCVDocument9 pagesLatest Development in PCVAndityo SidohutomoPas encore d'évaluation
- Corneal Collagen Cross-Linking in The Stabilization of KeratoconusDocument9 pagesCorneal Collagen Cross-Linking in The Stabilization of KeratoconusPunam RazputriPas encore d'évaluation
- 100152-Article Text-841-1-10-20210226Document5 pages100152-Article Text-841-1-10-20210226Rachel DenonaPas encore d'évaluation
- Dekker 2008Document6 pagesDekker 2008Charles CardosoPas encore d'évaluation
- My Approach To Interstitial Lung Disease Usingclinical, Radiological and Histopathological PatternsDocument15 pagesMy Approach To Interstitial Lung Disease Usingclinical, Radiological and Histopathological PatternsMarcelle FreirePas encore d'évaluation
- Prevalence of Blindness in Patients With Uveitis: Original ResearchDocument4 pagesPrevalence of Blindness in Patients With Uveitis: Original ResearchMuhammad RaflirPas encore d'évaluation
- Vogt-Koyanagi-Harada Disease: Francisco Max Damico, Szil Ard Kiss, and Lucy H. YoungDocument8 pagesVogt-Koyanagi-Harada Disease: Francisco Max Damico, Szil Ard Kiss, and Lucy H. YoungLalu Reza AldiraPas encore d'évaluation
- Paediatric Vesicoureteric Reflux Imaging, Where Are We Novel UltrasoundDocument7 pagesPaediatric Vesicoureteric Reflux Imaging, Where Are We Novel UltrasoundRiza Muhammad NuurPas encore d'évaluation
- Advances in Cardiovascular ImagingDocument9 pagesAdvances in Cardiovascular ImagingAlina SarbuPas encore d'évaluation
- 2 Wilkes1989Document9 pages2 Wilkes1989LAURA MARCELA BARRENECHE CALLEPas encore d'évaluation
- Uveitis and Systemic DiseaseDocument5 pagesUveitis and Systemic DiseaseAnonymous syRbQm6Pas encore d'évaluation
- Management of Premature Ventricular Complexes in TDocument12 pagesManagement of Premature Ventricular Complexes in TAmmon10famPas encore d'évaluation
- Clinical Presentation of Acute Appendicitis: Clinical Signs-Laboratory Findings-Clinical Scores, Alvarado Score and Derivate ScoresDocument10 pagesClinical Presentation of Acute Appendicitis: Clinical Signs-Laboratory Findings-Clinical Scores, Alvarado Score and Derivate ScoresRanjoo PriyaPas encore d'évaluation
- Clinical Characteristics and Surgical Safety in Congenital Cataract Eyes With Three Pathological Types of Posterior Capsule AbnormalitiesDocument9 pagesClinical Characteristics and Surgical Safety in Congenital Cataract Eyes With Three Pathological Types of Posterior Capsule Abnormalitiesaristo callenPas encore d'évaluation
- July 2016 Ophthalmic PearlsDocument4 pagesJuly 2016 Ophthalmic PearlsRaissaPas encore d'évaluation
- Spence 2009Document18 pagesSpence 2009Amma CrellinPas encore d'évaluation
- Clinical Review - FullDocument6 pagesClinical Review - FullfPas encore d'évaluation
- Inferior Vena Cava Ultrasonography For Volume Status EvaluationDocument13 pagesInferior Vena Cava Ultrasonography For Volume Status Evaluationtavo570Pas encore d'évaluation
- Amnion Rupture SequenceDocument4 pagesAmnion Rupture SequenceashrafmogyPas encore d'évaluation
- Preop Assesment Cardiac SurgeryDocument6 pagesPreop Assesment Cardiac Surgerybhimo priambodoPas encore d'évaluation
- Uveitis and Systemic DiseasesDocument50 pagesUveitis and Systemic DiseasesAnumeha JindalPas encore d'évaluation
- Ma 2021 Uveitis 101Document5 pagesMa 2021 Uveitis 101Jenny MaPas encore d'évaluation
- Median Arcuate Ligament Syndrome: A Clinical Dilemma: EditorialDocument2 pagesMedian Arcuate Ligament Syndrome: A Clinical Dilemma: EditorialAna Karen RPas encore d'évaluation
- Iewpoin: Onvergence Nsufficiency IagnosesDocument3 pagesIewpoin: Onvergence Nsufficiency IagnosesPierre A. RodulfoPas encore d'évaluation
- Valvas Uretrales PosterioresDocument8 pagesValvas Uretrales PosterioresJULIO EDUARDO CENTURION MAGNANPas encore d'évaluation
- Premature Ventricular Complexes in Apparently Normal Hearts 2016Document12 pagesPremature Ventricular Complexes in Apparently Normal Hearts 2016rentedmule00Pas encore d'évaluation
- 779 FullDocument6 pages779 FullAlexander G. Álvarez RojasPas encore d'évaluation
- Articulo Uveitis Anterior ViralDocument10 pagesArticulo Uveitis Anterior ViralJohana DíazPas encore d'évaluation
- Van Nieuwenhove Et Al 2021 Imaging of Traumatic and Atraumatic Penile LumpsDocument2 pagesVan Nieuwenhove Et Al 2021 Imaging of Traumatic and Atraumatic Penile LumpsThesisaurus IDPas encore d'évaluation
- Articulo 2Document6 pagesArticulo 2Sonia GarcíaPas encore d'évaluation
- Abdominal Trauma Presentation NotesDocument14 pagesAbdominal Trauma Presentation NoteszaminazzPas encore d'évaluation
- 135 139 PDFDocument5 pages135 139 PDFBramantya WuPas encore d'évaluation
- Current Approach in The Diagnosis and Management oDocument10 pagesCurrent Approach in The Diagnosis and Management oFabiant AsyifaPas encore d'évaluation
- International Consensus Statement On Nomenclature and Classification of The Congenital BAV and Its Aortopathy - 2021Document17 pagesInternational Consensus Statement On Nomenclature and Classification of The Congenital BAV and Its Aortopathy - 2021reymistery10Pas encore d'évaluation
- Feline Acute Kidney Injury. 2. Approach To Diagnosis, Treatment and PrognosisDocument9 pagesFeline Acute Kidney Injury. 2. Approach To Diagnosis, Treatment and PrognosisMartín QuirogaPas encore d'évaluation
- Approach To A Newborn With Suspected CHD: February 2012Document10 pagesApproach To A Newborn With Suspected CHD: February 2012akshayajainaPas encore d'évaluation
- RetinitisDocument11 pagesRetinitisJorge Troya CárdenasPas encore d'évaluation
- American Journal of Ophthalmology Case ReportsDocument3 pagesAmerican Journal of Ophthalmology Case ReportsElison Jaya PanggaloPas encore d'évaluation
- Ocular Manifestations of Leprosy - A Clinical Study: Original ArticleDocument4 pagesOcular Manifestations of Leprosy - A Clinical Study: Original ArticleAzizah TjakradidjajaPas encore d'évaluation
- Care of The Patient With Anterior Uveitis: Quick Reference GuideDocument4 pagesCare of The Patient With Anterior Uveitis: Quick Reference GuideAkicaPas encore d'évaluation
- Intussusception in Children - A Clinical ReviewDocument8 pagesIntussusception in Children - A Clinical Reviewjohanrubiano6Pas encore d'évaluation
- Chronic Obstructive Pulmonary DiseaseDocument293 pagesChronic Obstructive Pulmonary DiseaseWirjapratama PutraPas encore d'évaluation
- Eradication of Multi-Drug Resistant Ac... (Surg Infect (Larchmt)Document2 pagesEradication of Multi-Drug Resistant Ac... (Surg Infect (Larchmt)Wirjapratama PutraPas encore d'évaluation
- GRAFIKDocument1 pageGRAFIKWirjapratama PutraPas encore d'évaluation
- HackingDocument1 pageHackingWirjapratama PutraPas encore d'évaluation
- ACA 122-My Academic Plan (MAP) Assignment: InstructionsDocument5 pagesACA 122-My Academic Plan (MAP) Assignment: Instructionsapi-557842510Pas encore d'évaluation
- The Passive: Solutions Third Edition Upper-IntermediateDocument2 pagesThe Passive: Solutions Third Edition Upper-Intermediatelees10088Pas encore d'évaluation
- Patient's ProfileDocument1 pagePatient's ProfilehsiriaPas encore d'évaluation
- Neuro EEG BrochureDocument2 pagesNeuro EEG BrochureAhmad HamdounPas encore d'évaluation
- Glenmark Unveils Its Strategic Blueprint For Transition Into An Innovation ) Led Global Pharmaceutical Organization in The Next Decade (Company Update)Document31 pagesGlenmark Unveils Its Strategic Blueprint For Transition Into An Innovation ) Led Global Pharmaceutical Organization in The Next Decade (Company Update)Shyam SunderPas encore d'évaluation
- IMS US Diabetes MarketDocument6 pagesIMS US Diabetes MarketsyedPas encore d'évaluation
- CV RUGS Format TZMTJ 18022014Document6 pagesCV RUGS Format TZMTJ 18022014Nor LiyanaPas encore d'évaluation
- Referral Process Flow Chart: Updated 12/18/18 2017 SMDocument1 pageReferral Process Flow Chart: Updated 12/18/18 2017 SMnndjskPas encore d'évaluation
- Tujuan Pembelajaran: Asking - Filling in Medical ReportDocument8 pagesTujuan Pembelajaran: Asking - Filling in Medical ReportNesi AgustiaPas encore d'évaluation
- PratikPatel - Duodenal AtresiaDocument1 pagePratikPatel - Duodenal AtresiaIkhlasia Amali MahzumPas encore d'évaluation
- Project ProposalDocument5 pagesProject ProposalJessica GlitterPas encore d'évaluation
- St. Louis City Youth Sports GuidelinesDocument8 pagesSt. Louis City Youth Sports GuidelinesKevinSeanHeldPas encore d'évaluation
- Nursing Path o CardsDocument194 pagesNursing Path o CardsDanielle Shull100% (1)
- Herbal Its Project Biology.....Document52 pagesHerbal Its Project Biology.....MISHAPas encore d'évaluation
- Vacant Seats For Transfer - Admissions 2022Document4 pagesVacant Seats For Transfer - Admissions 2022Shahroz RindPas encore d'évaluation
- DRTP Announcement 2012-EnglishDocument2 pagesDRTP Announcement 2012-EnglishHengameh JavaheryPas encore d'évaluation
- Tubercular Meningitis in Children: Grisda Ledivia Lay, S.Ked 1508010038 Pembimbing: DR - Donny Argie, SP - BSDocument12 pagesTubercular Meningitis in Children: Grisda Ledivia Lay, S.Ked 1508010038 Pembimbing: DR - Donny Argie, SP - BSAulia PuspitaPas encore d'évaluation
- Covid BingDocument4 pagesCovid Bingaustinederick606Pas encore d'évaluation
- Wabah TBC Di VietnamDocument8 pagesWabah TBC Di VietnamSatya WangsaPas encore d'évaluation
- Executive Order 202-202.37 (June 05)Document87 pagesExecutive Order 202-202.37 (June 05)OAPas encore d'évaluation
- List of Providers - 10032023Document24 pagesList of Providers - 10032023Rodalyn PaddayumanPas encore d'évaluation
- APPS 2013 Japan WorkshopDocument19 pagesAPPS 2013 Japan WorkshopExaudi EbennezerPas encore d'évaluation
- Secondary Health 7 Q4 Module4Document9 pagesSecondary Health 7 Q4 Module4Rona RuizPas encore d'évaluation
- 2015 UEMX 3613 Topic4-Risk AssessmentDocument38 pages2015 UEMX 3613 Topic4-Risk AssessmentigantiPas encore d'évaluation
- Hospital List in SADocument26 pagesHospital List in SASudhakar KuppireddyPas encore d'évaluation
- Report AyendeDocument13 pagesReport AyendeAbubakar RabiuPas encore d'évaluation
- Pregestational ConditionsDocument66 pagesPregestational ConditionsEsvinch EsvinchPas encore d'évaluation
- The Secret To Great Health Escaping The Healthcare Matrix FinalDocument22 pagesThe Secret To Great Health Escaping The Healthcare Matrix FinalpenstyloPas encore d'évaluation
- HBSAG (Hepatitis B Antigen) TEST: PositiveDocument2 pagesHBSAG (Hepatitis B Antigen) TEST: PositiveJoycePas encore d'évaluation
- QR Management of Breast Cancer (3rd Ed)Document8 pagesQR Management of Breast Cancer (3rd Ed)Jye yiPas encore d'évaluation