Vous aimerez peut-être aussi
- Equity in Healthcare: Journal of the Student National Medical Association (JSNMA), #22.1D'EverandEquity in Healthcare: Journal of the Student National Medical Association (JSNMA), #22.1Pas encore d'évaluation
- Running Head: Lehighton Epidemiology Study 1Document11 pagesRunning Head: Lehighton Epidemiology Study 1shawnee11Pas encore d'évaluation
- Community Health Project Assignment 01068804Document14 pagesCommunity Health Project Assignment 01068804John HortonPas encore d'évaluation
- Research Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionD'EverandResearch Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionPas encore d'évaluation
- Screening Cleveland Public School Children for Hypertension and ObesityDocument4 pagesScreening Cleveland Public School Children for Hypertension and ObesitybbmantapPas encore d'évaluation
- Literature Review Childhood ObesityDocument4 pagesLiterature Review Childhood Obesityc5j07dce100% (1)
- Family Functioning StyleDocument6 pagesFamily Functioning Styletito_pintooPas encore d'évaluation
- Community Health Paper IIDocument19 pagesCommunity Health Paper IIapi-444056287Pas encore d'évaluation
- Preventing Obesity and Promoting Cardiometabolic Health: The Promise and Potential of Policies and The Affordable Care ActDocument5 pagesPreventing Obesity and Promoting Cardiometabolic Health: The Promise and Potential of Policies and The Affordable Care ActKristine Anne SorianoPas encore d'évaluation
- Capstone Literature ReviewDocument7 pagesCapstone Literature Reviewapi-548734139Pas encore d'évaluation
- Obesity Literature Review PDFDocument6 pagesObesity Literature Review PDFfat1kifywel3100% (1)
- The Social Determinants of Health: EditorialDocument6 pagesThe Social Determinants of Health: EditorialJoshPas encore d'évaluation
- Literature Review Obesity ChildhoodDocument8 pagesLiterature Review Obesity Childhoodafdttjujo100% (1)
- Teresa-Isiaho-Community AssessmentDocument10 pagesTeresa-Isiaho-Community Assessmentapi-337126539Pas encore d'évaluation
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsD'EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsPas encore d'évaluation
- Eating DisorderDocument6 pagesEating Disorderapi-609033638Pas encore d'évaluation
- Healthy Eating For Healthy CommunitiesDocument9 pagesHealthy Eating For Healthy CommunitiesMailey GanPas encore d'évaluation
- Reducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes: The Evidence from Population-Based InterventionsD'EverandReducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes: The Evidence from Population-Based InterventionsArden HandlerPas encore d'évaluation
- Nutritional Status of School Age Children in Private Elementary Schools: Basis For A Proposed Meal Management PlanDocument5 pagesNutritional Status of School Age Children in Private Elementary Schools: Basis For A Proposed Meal Management PlanIjaems JournalPas encore d'évaluation
- EnglishDocument9 pagesEnglishapi-245723352Pas encore d'évaluation
- Patients' Knowledge of Diabetes Complications and S Elf-Management Practices in GhanaDocument18 pagesPatients' Knowledge of Diabetes Complications and S Elf-Management Practices in GhanaNurul pattyPas encore d'évaluation
- Childhood Obesity Literature ReviewDocument7 pagesChildhood Obesity Literature Reviewc5eyjfnt100% (1)
- Healing Across Cultures: Pathways to Indigenius Health EquityD'EverandHealing Across Cultures: Pathways to Indigenius Health EquityPas encore d'évaluation
- The New Public Health: An Introduction for the 21st CenturyD'EverandThe New Public Health: An Introduction for the 21st CenturyPas encore d'évaluation
- Youngl Community Health Project Part 1 1Document7 pagesYoungl Community Health Project Part 1 1api-467110214Pas encore d'évaluation
- Does Education Modify The Effect of Ethnicity in The Expression of Ideal Cardiovascular Health? The Baptist Health South Florida Employee StudyDocument8 pagesDoes Education Modify The Effect of Ethnicity in The Expression of Ideal Cardiovascular Health? The Baptist Health South Florida Employee Studysankalp dasPas encore d'évaluation
- Childhood Obesityfinal 2Document12 pagesChildhood Obesityfinal 2api-260974225Pas encore d'évaluation
- Group Scholarly Paper-NewaygoDocument10 pagesGroup Scholarly Paper-Newaygoapi-283424486Pas encore d'évaluation
- What Is Public HealthDocument13 pagesWhat Is Public HealthHpg HsuPas encore d'évaluation
- Literature Review ObesityDocument4 pagesLiterature Review Obesityfvehwd96100% (1)
- Effective Care for High-Need Patients: Opportunities for Improving Outcomes, Value, and HealthD'EverandEffective Care for High-Need Patients: Opportunities for Improving Outcomes, Value, and HealthPas encore d'évaluation
- Timera Donald Fixed Document - Research ProposalDocument29 pagesTimera Donald Fixed Document - Research Proposalapi-533813582Pas encore d'évaluation
- Artikel Pubmed 3Document6 pagesArtikel Pubmed 3Sofa AmaliaPas encore d'évaluation
- Linking Neighborhood Factors to Food Insecurity in SeniorsDocument12 pagesLinking Neighborhood Factors to Food Insecurity in SeniorsNovita DewiPas encore d'évaluation
- Building Future Health and Well-Being of Thriving Toddlers and Young Children: 95th Nestlé Nutrition Institute Workshop, September 2020D'EverandBuilding Future Health and Well-Being of Thriving Toddlers and Young Children: 95th Nestlé Nutrition Institute Workshop, September 2020Pas encore d'évaluation
- Diseases of Poverty: Epidemiology, Infectious Diseases, and Modern PlaguesD'EverandDiseases of Poverty: Epidemiology, Infectious Diseases, and Modern PlaguesPas encore d'évaluation
- HS390 Group6 ResearchDocument6 pagesHS390 Group6 Researchjoseyalm2323Pas encore d'évaluation
- KaltsassjpintroDocument2 pagesKaltsassjpintroapi-384506632Pas encore d'évaluation
- Nutritional Status of Low-Income Families: Trend AnalysisDocument2 pagesNutritional Status of Low-Income Families: Trend AnalysisFrianne LuxPas encore d'évaluation
- PCD 12 E42Document11 pagesPCD 12 E42api-326476970Pas encore d'évaluation
- Community Health Paper Part IIDocument31 pagesCommunity Health Paper Part IIapi-260168909Pas encore d'évaluation
- SPH 492 Recommendations Michelle ChanDocument12 pagesSPH 492 Recommendations Michelle Chanapi-359725477Pas encore d'évaluation
- Research Statement Chizoba AnyimukwuDocument2 pagesResearch Statement Chizoba Anyimukwuapi-438638070Pas encore d'évaluation
- Emerging Issues in Geriatric Care: Aging and Public Health PerspectivesDocument6 pagesEmerging Issues in Geriatric Care: Aging and Public Health PerspectiveslynhareePas encore d'évaluation
- Diabetes-Related Knowledge Among Middle-Aged African American Women in North TexasD'EverandDiabetes-Related Knowledge Among Middle-Aged African American Women in North TexasPas encore d'évaluation
- Maternal and Child Undernutrition 2: SeriesDocument18 pagesMaternal and Child Undernutrition 2: SeriesBudirmanPas encore d'évaluation
- Transcultural Diabetes CareDocument37 pagesTranscultural Diabetes CareTengku EltrikanawatiPas encore d'évaluation
- 9 FullDocument7 pages9 FullSaudah Sii SipitPas encore d'évaluation
- ESSINGTON. Legislating Weight Loss. Are Antiobesity Public Health Policies Making An ImpactDocument9 pagesESSINGTON. Legislating Weight Loss. Are Antiobesity Public Health Policies Making An ImpactNina NavajasPas encore d'évaluation
- Preventing Childhood Overweight and Obesity: Parents Can Make A DifferenceDocument20 pagesPreventing Childhood Overweight and Obesity: Parents Can Make A DifferenceProject PAPas encore d'évaluation
- Nutritional Status of Pre-School Children From Low Income FamiliesDocument11 pagesNutritional Status of Pre-School Children From Low Income FamiliesFiraz R AkbarPas encore d'évaluation
- Socioeconomic Status and Obesity A Review of The Literature PDFDocument6 pagesSocioeconomic Status and Obesity A Review of The Literature PDFafmabreouxqmrcPas encore d'évaluation
- Adverse Childhood Experiences: Retrospective Study To Determine Their Impact On Adult Health Behaviours and Health Outcomes in A UK PopulationDocument11 pagesAdverse Childhood Experiences: Retrospective Study To Determine Their Impact On Adult Health Behaviours and Health Outcomes in A UK PopulationBadger6Pas encore d'évaluation
- H SC 400 Journal CritiqueDocument6 pagesH SC 400 Journal Critiqueapi-735565786Pas encore d'évaluation
- Fast FoodDocument8 pagesFast Foodkangna_sharma20Pas encore d'évaluation
- Jurnal Nomor 19Document10 pagesJurnal Nomor 19Agusniko SinagaPas encore d'évaluation
- Jeanine MDocument2 pagesJeanine Mapi-417952873Pas encore d'évaluation
- ExemplarDocument4 pagesExemplarapi-417952873Pas encore d'évaluation
- Pediatric Use of Insulin Pump Therapy and Its Impact On Glycemic Control CorrectedDocument17 pagesPediatric Use of Insulin Pump Therapy and Its Impact On Glycemic Control Correctedapi-417952873Pas encore d'évaluation
- Running Head: DISCHARGE PLAN 1Document11 pagesRunning Head: DISCHARGE PLAN 1api-417952873Pas encore d'évaluation
- ExemplarDocument4 pagesExemplarapi-417952873Pas encore d'évaluation
- Diaz Poster Presentation 1Document1 pageDiaz Poster Presentation 1api-417952873Pas encore d'évaluation
- Return of Bowel Sounds Indicating An End ofDocument12 pagesReturn of Bowel Sounds Indicating An End ofapi-417952873Pas encore d'évaluation
- Nur 342 Goals Objectives WorksheetDocument2 pagesNur 342 Goals Objectives Worksheetapi-417952873100% (3)
- The Benefits of Uninterrupted Skin To Skin Contact JMDDocument10 pagesThe Benefits of Uninterrupted Skin To Skin Contact JMDapi-417952873Pas encore d'évaluation
- Concept Map 321Document13 pagesConcept Map 321api-417952873Pas encore d'évaluation
- JMD PPH Critical Thinking Map-1Document1 pageJMD PPH Critical Thinking Map-1api-417952873Pas encore d'évaluation
- FinalconceptmapjmdDocument8 pagesFinalconceptmapjmdapi-417952873Pas encore d'évaluation
- Concept Map Final JMDDocument14 pagesConcept Map Final JMDapi-417952873Pas encore d'évaluation
- Acute Care Map Diaz 1Document16 pagesAcute Care Map Diaz 1api-417952873Pas encore d'évaluation
- Infections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaDocument68 pagesInfections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaMonique BorresPas encore d'évaluation
- Epidemiology - ReportDocument9 pagesEpidemiology - ReportIsabel HernandezPas encore d'évaluation
- Gastrointestinal DiseaseDocument20 pagesGastrointestinal DiseasenarenmaniamPas encore d'évaluation
- ABCs of Neuroimaging - Ali YIKILMAZDocument45 pagesABCs of Neuroimaging - Ali YIKILMAZRanintha SurbaktiPas encore d'évaluation
- Cardiovascular Disorder Case Study - EditedDocument4 pagesCardiovascular Disorder Case Study - EditedTimohPas encore d'évaluation
- Pathophysiology: Tonsillitis Is Inflammation of The Tonsils, Two OvalDocument13 pagesPathophysiology: Tonsillitis Is Inflammation of The Tonsils, Two Ovalyangi doka100% (1)
- Hepatitis B Serological Markers and Plasma DNA ConDocument9 pagesHepatitis B Serological Markers and Plasma DNA ConSerendipity21Pas encore d'évaluation
- Myasthenia Gravis PTDocument4 pagesMyasthenia Gravis PTKarunya VkPas encore d'évaluation
- Diabetic Treatment Adherence at LASUTHDocument63 pagesDiabetic Treatment Adherence at LASUTHijojo elizabethPas encore d'évaluation
- Communicable Diseases GR.8 HealthDocument40 pagesCommunicable Diseases GR.8 HealthAiza May RosasPas encore d'évaluation
- 10 Healty Gateways Info For Ships To Prepare For COVID-19 PDFDocument16 pages10 Healty Gateways Info For Ships To Prepare For COVID-19 PDFDennis VolodchenkoPas encore d'évaluation
- Computer-Based English Proficiency Test AdvisoryDocument7 pagesComputer-Based English Proficiency Test AdvisoryJoyce CarilloPas encore d'évaluation
- The Lasting Impact of Covid-19 2Document4 pagesThe Lasting Impact of Covid-19 2api-650392913Pas encore d'évaluation
- COPD vs. Asthma Symptoms: 6 Differences and 6 SimilaritiesDocument3 pagesCOPD vs. Asthma Symptoms: 6 Differences and 6 Similaritiessd saklinePas encore d'évaluation
- CA 15.3 breast cancer antigen testDocument4 pagesCA 15.3 breast cancer antigen testडा. सत्यदेव त्यागी आर्यPas encore d'évaluation
- Updated COVID-19 Quarantine InformationDocument1 pageUpdated COVID-19 Quarantine Informationkitty smithPas encore d'évaluation
- Skin Pathology: DR Shehu Abdullahi 19/01/2023Document23 pagesSkin Pathology: DR Shehu Abdullahi 19/01/2023Mohammed HussainPas encore d'évaluation
- Sample: Extract 1: Questions 31-36Document5 pagesSample: Extract 1: Questions 31-36Jorge VegaPas encore d'évaluation
- Assessment Checklist Measles Rubella VaccineDocument1 pageAssessment Checklist Measles Rubella VaccineDatu Hoffer RhuPas encore d'évaluation
- Initial Patient Assessment in OpdDocument4 pagesInitial Patient Assessment in OpdLokender Goyal100% (1)
- Biostatistic and Epidemiology Lecture NoteDocument66 pagesBiostatistic and Epidemiology Lecture Notefff100% (3)
- Sas 40Document2 pagesSas 40Sistine Rose LabajoPas encore d'évaluation
- COVID Origin and Global SpreadDocument12 pagesCOVID Origin and Global SpreadChaitanya BhardwajPas encore d'évaluation
- Learning About Noncommunicable DiseasesDocument2 pagesLearning About Noncommunicable DiseasesRafaella Feroza CastroPas encore d'évaluation
- Department of Molecular Virology: COVID-19 (Corona) VirusDocument1 pageDepartment of Molecular Virology: COVID-19 (Corona) VirusMuhammad AreebPas encore d'évaluation
- WIL - English Does Work 7 Cronica WRITINGDocument2 pagesWIL - English Does Work 7 Cronica WRITINGwilbert edill rodriguez martinez50% (2)
- Mayo Clinic BPPVDocument4 pagesMayo Clinic BPPVCS NarayananPas encore d'évaluation
- Pediatric SmleDocument59 pagesPediatric SmleMoayad Zeyad M100% (1)
- Rheum at OlogyDocument42 pagesRheum at Ologymy Lord JesusPas encore d'évaluation
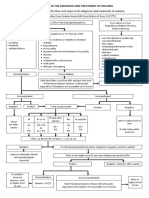
- Algorithm in The Diagnosis and Treatment of MalariaDocument1 pageAlgorithm in The Diagnosis and Treatment of MalariaPearl Monette Cedeño AngPas encore d'évaluation