Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- 2020 15 TheaII - SvitzerJosephineDocument44 pages2020 15 TheaII - SvitzerJosephinesoongbinPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Safety Flyer To The Fishing IndustryDocument2 pagesSafety Flyer To The Fishing IndustrysoongbinPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
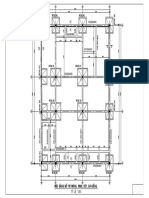
- KC - 02-12 (Mat Bang Bo Tri Mong)Document1 pageKC - 02-12 (Mat Bang Bo Tri Mong)soongbinPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- MIT6 0002F16 Lec3 Graph Theoretic ModelDocument38 pagesMIT6 0002F16 Lec3 Graph Theoretic ModelsoongbinPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Tor and The Dark Net - Volume 1 (2016) PDFDocument40 pagesTor and The Dark Net - Volume 1 (2016) PDFvectorone100% (1)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- DM StatDocument7 pagesDM StatlxangelusxlPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- KC 06-12 PDFDocument1 pageKC 06-12 PDFsoongbinPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- IMCA Safety Flash 17-18Document5 pagesIMCA Safety Flash 17-18soongbinPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Bollard Pull AESDocument7 pagesBollard Pull AESsoongbinPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- Twin Cranes Lift Arrangement by Orca PDFDocument6 pagesTwin Cranes Lift Arrangement by Orca PDFsoongbinPas encore d'évaluation
- GL Iv-6-4 eDocument214 pagesGL Iv-6-4 ejobinhoeljovenPas encore d'évaluation
- Linear Regression with One Variable ExplainedDocument49 pagesLinear Regression with One Variable ExplainedRamon LinsPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Inclining Test Unified Procedure No.31Document5 pagesInclining Test Unified Procedure No.31Emrah YesiltasPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Hydrodynamic ToolsDocument10 pagesHydrodynamic ToolssoongbinPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Lecture8 PDFDocument42 pagesLecture8 PDFsoongbinPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Linear Regression with One Variable ExplainedDocument49 pagesLinear Regression with One Variable ExplainedRamon LinsPas encore d'évaluation
- Tumors of The Central Nervous System - VOL 12Document412 pagesTumors of The Central Nervous System - VOL 12vitoPas encore d'évaluation
- Iso 28000Document11 pagesIso 28000Aida FatmawatiPas encore d'évaluation
- Allium CepaDocument90 pagesAllium CepaYosr Ahmed100% (3)
- Module A Specimen Questions January2020 PDFDocument5 pagesModule A Specimen Questions January2020 PDFShashi Bhusan SinghPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Directory of Frequently Called Numbers: Maj. Sheikh RahmanDocument1 pageDirectory of Frequently Called Numbers: Maj. Sheikh RahmanEdward Ebb BonnoPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- CERADocument10 pagesCERAKeren Margarette AlcantaraPas encore d'évaluation
- Rudraksha - Scientific FactsDocument20 pagesRudraksha - Scientific FactsAkash Agarwal100% (3)
- 1 Colmac DX Ammonia Piping Handbook 4th EdDocument64 pages1 Colmac DX Ammonia Piping Handbook 4th EdAlbertoPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Characteristics of Uveitis Presenting For The First Time in The Elderly Analysis of 91 Patients in A Tertiary CenterDocument9 pagesCharacteristics of Uveitis Presenting For The First Time in The Elderly Analysis of 91 Patients in A Tertiary CenterFrancescFranquesaPas encore d'évaluation
- Base para Detectores de Humo y Temperatura KIDDE KI-SBDocument2 pagesBase para Detectores de Humo y Temperatura KIDDE KI-SBAnderson CastañedaPas encore d'évaluation
- Parasitology Lecture Hosts, Symbiosis & TransmissionDocument10 pagesParasitology Lecture Hosts, Symbiosis & TransmissionPatricia Ann JosePas encore d'évaluation
- Urban Drainage Modelling Guide IUD - 1Document196 pagesUrban Drainage Modelling Guide IUD - 1Helmer Edgardo Monroy GonzálezPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Genetically Engineered MicroorganismsDocument6 pagesGenetically Engineered Microorganismsaishwarya joshiPas encore d'évaluation
- Workplace Hazard Analysis ProcedureDocument12 pagesWorkplace Hazard Analysis ProcedureKent Nabz60% (5)
- English III Module 2 Simple Present Job and Job VerbsDocument4 pagesEnglish III Module 2 Simple Present Job and Job VerbsAdrian CortesPas encore d'évaluation
- Cipac MT 185Document2 pagesCipac MT 185Chemist İnançPas encore d'évaluation
- Haematology Notes - 3rd EdDocument100 pagesHaematology Notes - 3rd EdSally Brit100% (1)
- Tugas B InggrisDocument9 pagesTugas B InggrisDellyna AlmaPas encore d'évaluation
- Abortion and UtilitarianismDocument4 pagesAbortion and UtilitarianismBrent Harvey Soriano JimenezPas encore d'évaluation
- Human Capital FormationDocument9 pagesHuman Capital Formationtannu singh67% (6)
- Mod 6 Soft Tissue InjuriesDocument5 pagesMod 6 Soft Tissue Injuriesrez1987100% (1)
- Quality Control Plan Static EquipmentDocument1 pageQuality Control Plan Static EquipmentdhasdjPas encore d'évaluation
- Switzerland: Food and CultureDocument18 pagesSwitzerland: Food and CultureAaron CoutinhoPas encore d'évaluation
- Pictorial History of AOTADocument5 pagesPictorial History of AOTAThe American Occupational Therapy Association0% (4)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Social Studies SbaDocument12 pagesSocial Studies SbaSupreme KingPas encore d'évaluation
- Notice: Use of Segways® and Similar Devices by Individuals With A Mobility Impairment in GSA-Controlled Federal FacilitiesDocument2 pagesNotice: Use of Segways® and Similar Devices by Individuals With A Mobility Impairment in GSA-Controlled Federal FacilitiesJustia.comPas encore d'évaluation
- Operating Instructions: Katflow 100Document52 pagesOperating Instructions: Katflow 100Nithin KannanPas encore d'évaluation
- 2 English Course BDocument8 pages2 English Course BAnjana27Pas encore d'évaluation
- 2.1. Pharmacological Therapeutics. 2.2. Basic Cardiac Life Support (BCLS) and Advanced Cardiac Life Support (ACLS) in Neonates and ChildDocument3 pages2.1. Pharmacological Therapeutics. 2.2. Basic Cardiac Life Support (BCLS) and Advanced Cardiac Life Support (ACLS) in Neonates and Childclint xavier odangoPas encore d'évaluation
- EcR - 1 Leading and Lagging IndicatorsDocument10 pagesEcR - 1 Leading and Lagging IndicatorsMiloš ĐukićPas encore d'évaluation
- Endure: How to Work Hard, Outlast, and Keep HammeringD'EverandEndure: How to Work Hard, Outlast, and Keep HammeringÉvaluation : 4.5 sur 5 étoiles4.5/5 (283)
- Transformed: Moving to the Product Operating ModelD'EverandTransformed: Moving to the Product Operating ModelÉvaluation : 4 sur 5 étoiles4/5 (1)