Vous aimerez peut-être aussi
- MBE-Con Law OutlineDocument31 pagesMBE-Con Law OutlineStacy Oliveira100% (3)
- Our Campus, Our SafetyDocument44 pagesOur Campus, Our SafetyToronto Star100% (2)
- Transgender ArticleDocument9 pagesTransgender ArticleKob PhetphachanhPas encore d'évaluation
- Gad SogieDocument104 pagesGad SogieRiejie Sta IsabelPas encore d'évaluation
- Gender-Nonconforming Lesbian, Gay, Bisexual, and Transgender Youth: School Victimization and Young Adult Psychosocial AdjustmentDocument10 pagesGender-Nonconforming Lesbian, Gay, Bisexual, and Transgender Youth: School Victimization and Young Adult Psychosocial AdjustmentGender SpectrumPas encore d'évaluation
- LGBT Thesis EnglishDocument15 pagesLGBT Thesis EnglishStalita NiColaou50% (6)
- Primary SocializationDocument16 pagesPrimary SocializationJoy CruzPas encore d'évaluation
- What Research Shows: NARTH's Response To The APA Claims On HomosexualityDocument4 pagesWhat Research Shows: NARTH's Response To The APA Claims On Homosexualitybmx0Pas encore d'évaluation
- Discussion On Gender and Sexuality in DSM 5 Justin BarronDocument28 pagesDiscussion On Gender and Sexuality in DSM 5 Justin BarronDedi Ariwibowo100% (1)
- Transgender Literature Review 1 Running Head: Transgender Research Literature ReviewDocument13 pagesTransgender Literature Review 1 Running Head: Transgender Research Literature ReviewPrincess Irish Daryll DiegoPas encore d'évaluation
- Mental Health in Lesbian, Gay, Bisexual, and Transgender (LGBT) YouthDocument25 pagesMental Health in Lesbian, Gay, Bisexual, and Transgender (LGBT) YouthKaren Angelie D. Bedaño100% (1)
- "Written Report: Gender Dysphoria": Polytechnic University of The PhilippinesDocument11 pages"Written Report: Gender Dysphoria": Polytechnic University of The PhilippinesAnnie JnePas encore d'évaluation
- Position PaperDocument8 pagesPosition PaperRufa Mae BarbaPas encore d'évaluation
- Gender and SexualityDocument58 pagesGender and SexualityNino ShorttePas encore d'évaluation
- Gender IdentityDocument7 pagesGender Identityshakti1432ssPas encore d'évaluation
- Gender DysphoriaDocument5 pagesGender DysphoriaRochelle Cuenca100% (1)
- The Importance of Comprehensive Sexual Education in School CurriculumsDocument9 pagesThe Importance of Comprehensive Sexual Education in School CurriculumsDavid GoosePas encore d'évaluation
- Report On Gender and Sexuality OutlineDocument8 pagesReport On Gender and Sexuality OutlineBear OstreaPas encore d'évaluation
- School-Related Violence and Bullying On The Basis of Sexual Orientation and Gender Identity or Expression (SOGIE)Document85 pagesSchool-Related Violence and Bullying On The Basis of Sexual Orientation and Gender Identity or Expression (SOGIE)Jae LeePas encore d'évaluation
- Beyond The Absent Breadwinner: Mapping The Paternal Masculinities of Dutch Highly Involved FathersDocument22 pagesBeyond The Absent Breadwinner: Mapping The Paternal Masculinities of Dutch Highly Involved FathersJustine Van de BeekPas encore d'évaluation
- From Gender Identity Disorder To Gender Identity CreativityDocument21 pagesFrom Gender Identity Disorder To Gender Identity CreativityGender SpectrumPas encore d'évaluation
- Sexual Orientation and Gender IdentityDocument3 pagesSexual Orientation and Gender IdentityAizel Elumbaring100% (2)
- Sex, Sexuality & Gender-NotesDocument6 pagesSex, Sexuality & Gender-NotesPinakiRanjanSarkarPas encore d'évaluation
- Hegemony of HeteronormativityDocument18 pagesHegemony of HeteronormativitySilvia Ozawa100% (1)
- Sex ReassignmentDocument28 pagesSex ReassignmentBarbara Evans Fleischauer100% (1)
- TransgenderDocument6 pagesTransgenderapi-390108584Pas encore d'évaluation
- Gender Dysphoria: Submitted By: Rhea Andrea F. Uy BS Psychology 3-1Document7 pagesGender Dysphoria: Submitted By: Rhea Andrea F. Uy BS Psychology 3-1Rhea Andrea Uy100% (1)
- LGBTQDocument21 pagesLGBTQValerie Miguel100% (1)
- Gender Spectrum - Understanding GenderDocument2 pagesGender Spectrum - Understanding GenderGender SpectrumPas encore d'évaluation
- Heterosexual Identity DevelopmentDocument36 pagesHeterosexual Identity DevelopmentDiego JoaquínPas encore d'évaluation
- Gender Based ViolenceDocument24 pagesGender Based ViolenceAnngelina Mandigma100% (1)
- Debate On HomosexualsDocument2 pagesDebate On HomosexualsLiQinghuaPas encore d'évaluation
- AbstractDocument6 pagesAbstractdeviPas encore d'évaluation
- A Research Study About Loneliness, Social Connectedness and Life Attitude of Working Persons With DisabilityDocument57 pagesA Research Study About Loneliness, Social Connectedness and Life Attitude of Working Persons With DisabilityArveeh AvilesPas encore d'évaluation
- Paul Cameron Gay Parents More Apt To MolestDocument11 pagesPaul Cameron Gay Parents More Apt To MolestIrritated Genie100% (1)
- Essay Gay MarriageDocument3 pagesEssay Gay MarriageJoanna KolczyńskaPas encore d'évaluation
- Transgender Persons Rights in The EU Member StatesDocument32 pagesTransgender Persons Rights in The EU Member StatesLukas BerredoPas encore d'évaluation
- Gender Identity Disorder in Children and AdolescentsDocument27 pagesGender Identity Disorder in Children and AdolescentsGender Spectrum100% (3)
- Chapter 1 3 FINALDocument31 pagesChapter 1 3 FINALDhimple HidalgocunananPas encore d'évaluation
- Gender Dysphoria PaperDocument4 pagesGender Dysphoria Paperapi-242440017Pas encore d'évaluation
- HomosexualityDocument22 pagesHomosexualityVincent Maslog Ang88% (8)
- LGBTDocument89 pagesLGBTFrancis CrizonPas encore d'évaluation
- Changing Sexual Orientation: A Consumers' Report Ariel Shidlo and Michael SchroederDocument11 pagesChanging Sexual Orientation: A Consumers' Report Ariel Shidlo and Michael Schroederbmx0Pas encore d'évaluation
- Social Dimension - Sex and Education (Chapter 8)Document10 pagesSocial Dimension - Sex and Education (Chapter 8)Francis A. DiazPas encore d'évaluation
- The Sexual SelfDocument29 pagesThe Sexual SelfYumi GushikenPas encore d'évaluation
- What Is Human Sexuality?Document30 pagesWhat Is Human Sexuality?Muhammad NurthariqPas encore d'évaluation
- Gender DysphoriaDocument33 pagesGender Dysphoriamuhammad sholihuddinPas encore d'évaluation
- Rape Culture EssayDocument9 pagesRape Culture Essayapi-314553279Pas encore d'évaluation
- 1 Sex, Gender, and Sexuality2Document16 pages1 Sex, Gender, and Sexuality2Anne WongPas encore d'évaluation
- Factors Affecting Societal Acceptance Among The Lgbtqia+ Community Members of Infotech Development Systems Colleges INC. ACADEMIC YEAR 2022-2023Document30 pagesFactors Affecting Societal Acceptance Among The Lgbtqia+ Community Members of Infotech Development Systems Colleges INC. ACADEMIC YEAR 2022-2023Mark Nhel Pardiñas BuelvaPas encore d'évaluation
- A Clockwork OrangeDocument2 pagesA Clockwork OrangeAnjo OlorPas encore d'évaluation
- Gender Identity and Sexual Orientation Development Among TeenagersDocument9 pagesGender Identity and Sexual Orientation Development Among TeenagersCarmella PlangPas encore d'évaluation
- LGBT Thesis ManuscriptDocument31 pagesLGBT Thesis ManuscriptJamille YapPas encore d'évaluation
- Care of The Child With The Desire To Change GenderDocument8 pagesCare of The Child With The Desire To Change GenderGender SpectrumPas encore d'évaluation
- 10 Page Essay WFCDocument12 pages10 Page Essay WFCapi-344557725Pas encore d'évaluation
- Sexuality in IslamDocument100 pagesSexuality in IslamRadulescu MarianPas encore d'évaluation
- Position Paper of LGBTDocument2 pagesPosition Paper of LGBTLov Aie ElyPas encore d'évaluation
- Running Head: LGBT 1Document8 pagesRunning Head: LGBT 1Nathaniel BernalPas encore d'évaluation
- LGBT RightsDocument17 pagesLGBT RightsFeleen Miñon100% (1)
- Gender Identity Presentation SlidesDocument21 pagesGender Identity Presentation Slidesapi-393037741100% (1)
- LGBT ThailandDocument49 pagesLGBT ThailandcanPas encore d'évaluation
- Equipment KeysDocument3 pagesEquipment KeysBreajAdarbePas encore d'évaluation
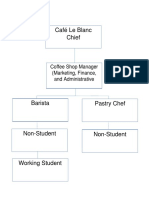
- Org ChartDocument1 pageOrg ChartBreajAdarbePas encore d'évaluation
- Prevention Cost Actual CostDocument2 pagesPrevention Cost Actual CostBreajAdarbePas encore d'évaluation
- Indian Foods by RegionDocument2 pagesIndian Foods by RegionBreajAdarbePas encore d'évaluation
- In Partial Fulfilment of The Requirements For The SubjectDocument4 pagesIn Partial Fulfilment of The Requirements For The SubjectBreajAdarbePas encore d'évaluation
- Yceum of The Philippines University Cavite Campus College of International Tourism and Hospitality ManagementDocument4 pagesYceum of The Philippines University Cavite Campus College of International Tourism and Hospitality ManagementBreajAdarbePas encore d'évaluation
- WesternDocument71 pagesWesternBreajAdarbePas encore d'évaluation
- Multiple Choice Questions and Answers On TransistorsDocument16 pagesMultiple Choice Questions and Answers On TransistorsBreajAdarbe50% (2)
- BSBDIV501 Assess - 2Document3 pagesBSBDIV501 Assess - 2Anjali ChoudharyPas encore d'évaluation
- Discrimination Against Women and The Girl ChildDocument151 pagesDiscrimination Against Women and The Girl Childdlaw8390% (10)
- 21ST Century Q2 M1 L3 Justine MimayDocument5 pages21ST Century Q2 M1 L3 Justine MimayMark Kenneth CastilloPas encore d'évaluation
- Age Discrimination 2Document2 pagesAge Discrimination 2Raphael Seke OkokoPas encore d'évaluation
- Humanrights Project FinalDocument27 pagesHumanrights Project FinalSakshiPas encore d'évaluation
- DiscriminationDocument2 pagesDiscriminationDarlene Jane MaynesPas encore d'évaluation
- Gender Inequality in The Hospitality Industry: Issues and Challenges. A Case Study of Selected Hotels in Ondo State in NigeriaDocument6 pagesGender Inequality in The Hospitality Industry: Issues and Challenges. A Case Study of Selected Hotels in Ondo State in NigeriaReymark Pe�aflorPas encore d'évaluation
- Notice: Investment Company Act of 1940: MFS Series Trust X Et Al.Document4 pagesNotice: Investment Company Act of 1940: MFS Series Trust X Et Al.Justia.comPas encore d'évaluation
- Valerie Underwood v. State of New York, Office of Court Administration, New York State Civil Service Commission, and James Ruffin, Defendants-Intervenors, 647 F.2d 162, 2d Cir. (1981)Document2 pagesValerie Underwood v. State of New York, Office of Court Administration, New York State Civil Service Commission, and James Ruffin, Defendants-Intervenors, 647 F.2d 162, 2d Cir. (1981)Scribd Government DocsPas encore d'évaluation
- Albanian HomophobiaDocument4 pagesAlbanian HomophobiaSasa MilosevicPas encore d'évaluation
- The Universal Declaration On Bioethics and Human RightsDocument14 pagesThe Universal Declaration On Bioethics and Human RightsMohamed SaberPas encore d'évaluation
- Discrimination at WorkDocument19 pagesDiscrimination at WorkruchikabantaPas encore d'évaluation
- Discrimination in Health CareDocument5 pagesDiscrimination in Health CareKimberly Poong100% (10)
- PDF (SG) - EAP11 - 12 - UNIT 1 - LESSON 1 - Structure of Academic TextsDocument23 pagesPDF (SG) - EAP11 - 12 - UNIT 1 - LESSON 1 - Structure of Academic TextsAshliegh Luna NorbePas encore d'évaluation
- Intercultural Communication A Critical Introductio... - (Chapter 9 Intercultural Communication and Exclusion)Document16 pagesIntercultural Communication A Critical Introductio... - (Chapter 9 Intercultural Communication and Exclusion)LUIS ALBERTO TORRES VASQUEZPas encore d'évaluation
- Jus Cogens ReduxDocument6 pagesJus Cogens ReduxJessie ZhangPas encore d'évaluation
- Theo.2 Chapter 6Document13 pagesTheo.2 Chapter 6Baozi dumpsPas encore d'évaluation
- 2015-16 School District CalendarDocument24 pages2015-16 School District Calendarapi-278670576Pas encore d'évaluation
- MD2718699Document1 pageMD2718699Political AlertPas encore d'évaluation
- Apartheid in South AfricaDocument5 pagesApartheid in South AfricaBrandy SangurahPas encore d'évaluation
- Complaint and Adjustment Letter Example PDFDocument16 pagesComplaint and Adjustment Letter Example PDFEdmundo MunguambePas encore d'évaluation
- Affirmative Action Programs: - Utilization AnalysisDocument10 pagesAffirmative Action Programs: - Utilization AnalysissarlagroverPas encore d'évaluation
- Working With WordsDocument1 pageWorking With WordsnounaPas encore d'évaluation
- 10 - Defendants' Answer To Plaintiff's Complaint (11.04.22)Document50 pages10 - Defendants' Answer To Plaintiff's Complaint (11.04.22)WNDUPas encore d'évaluation
- EEODocument17 pagesEEOClive RhavenPas encore d'évaluation
- Win TR20 User Guide Ver 310 Mar 2015Document253 pagesWin TR20 User Guide Ver 310 Mar 2015Edi GunawanPas encore d'évaluation
- Medical Jurisprudence GuideDocument13 pagesMedical Jurisprudence GuideSev SevaarPas encore d'évaluation
- Case 1 WalmartDocument2 pagesCase 1 Walmartijustateanapple100% (2)