Académique Documents
Professionnel Documents
Culture Documents
Kellum 2018
Transféré par
hemer hadyn calderon alvitesCopyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Kellum 2018
Transféré par
hemer hadyn calderon alvitesDroits d'auteur :
Formats disponibles
REVIEWS
Paradigms of acute kidney injury
in the intensive care setting
John A. Kellum1 and John R. Prowle2,3
Abstract | Acute kidney injury (AKI) is a heterogeneous clinical syndrome that has multiple
aetiologies, variable pathogenesis and diverse outcomes. However, these heterogeneities are not
reflected in current approaches to the diagnosis and, to some degree, treatment of AKI. For
example, congestive heart failure and dehydration can produce identical changes in serum
creatinine level and urine output (parameters that are used to define AKI); however, they differ
vastly in their physiological contexts and demand completely opposite treatments. AKI is often
still considered to be a homogeneous clinical entity, which implies a uniform pathogenesis and a
well-defined prognosis. As a consequence, efforts to find effective AKI treatments have been
hampered by a lack of clear clinical classifications for various types of AKI. In addition,
subclassification of AKI into subclinical phenotypes — for example, on the basis of protein
biomarkers and other in vitro diagnostics that take into account disease aetiology and underlying
pathogenesis — might be necessary to develop therapeutic approaches that effectively target
the widely differing pathomechanisms of AKI. In this Review, we discuss the major subtypes of AKI
that are associated with sepsis, major surgery, renal hypoperfusion and nephrotoxin exposure —
situations that are typically seen in the intensive care setting. We consider differences and
similarities in their phenotype, pathogenesis and outcomes and how this information might be
used to guide treatment.
1
Center for Critical Care Acute kidney injury (AKI) — a loose collection of any degree of AKI have an increased risk of death that
Nephrology, Department syndromes characterized by a sudden decrease in esti is at least in part attributable to AKI itself, although the
of Critical Care Medicine, mated glomerular filtration rate (eGFR) — is estimated reasons for this association are not fully understood.
University of Pittsburgh
School of Medicine and
to affect 2–3 people per 1,000 individuals in the USA1. Translation of these clear epidemiological observa
University of Pittsburgh However, this approximation is likely to be an under tions to clinical practice has proved complex, however,
Medical Center, estimate owing to the silent nature of AKI: the incidence and current management remains based on minimizing
3347 Forbes Avenue, could be as high as 15 in 1,000 adults per year in the the risk of developing AKI and providing supportive
Suite 220, Pittsburgh,
UK2. Moreover, older individuals are disproportion care7. This division between the increased recognition
Pennsylvania 15213, USA.
2
Adult Critical Care Unit, ately affected by AKI: the rate of AKI in 2011 among of AKI and the lack of substantial developments in AKI
Department of Renal and US Medicare patients aged 66–69 years was 14.9 per therapy has led to criticism of current concepts and defi
Transplant Medicine, 1,000 individuals, increasing with age to 18.8 per 1,000 nitions as being inadequate to individualize therapy and
The Royal London Hospital, individuals aged 70–74, 26.4 per 1,000 individuals aged improve outcomes8 (BOX 1). In the same way that can
Whitechapel Road,
London E1 1BB, UK.
75–79, 35.9 per 1,000 individuals aged 80–84, and cer therapies were advanced initially by understanding
3
William Harvey Research 49.6 per 1,000 individuals aged ≥85 (REF. 3). The con malignancy in general, but subsequently revolutionized
Institute, Barts and the sequences of AKI are no less substantial in older indi by characterization of differences among molecular
London School of Medicine viduals. The relative risk of death attributable to AKI subtypes, a universal strategy is unlikely to be success
and Dentistry, Queen Mary
is similar across age groups, despite lower overall sur ful in the treatment of AKI given the widely differing
University of London,
Charterhouse Square, vival and lower odds of renal function recovery among underlying mechanisms; instead, targeted treatment will
London EC1M 6BQ, UK. older individuals4. probably be required to achieve consistent clinical bene
Correspondence to J.A.K. Evidence from the past few years also suggests that fits. The concept that AKI is a syndrome of rising serum
kellumja@upmc.edu even mild forms of AKI (for example, a 50% increase in creatinine levels and/or oliguria caused by multifactorial
doi:10.1038/nrneph.2017.184 serum creatinine) are associated with an increased risk systemic insults raises the question to what extent a com
Published online 22 Jan 2018 of hospital mortality 5,6. Therefore, patients who develop mon pathophysiological pathway exists following diverse
NATURE REVIEWS | NEPHROLOGY VOLUME 14 | APRIL 2018 | 217
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Key points Sepsis is characterized by systemic vasodilation,
profound alterations in the macrocirculation and
• Acute kidney injury (AKI) is not a single disease but a loose collection of syndromes microcirculation with heterogeneity of regional blood
characterized by an abrupt decrease in glomerular filtration rate flow distribution17 and substantial decreases in func
• Broad classifications of AKI — according to the dominant aetiology (such as sepsis or tional capillary density 18,19. In humans and large animal
nephrotoxicity) as opposed to pseudo-anatomical categories (for example, prerenal models, including sheep and pigs, cardiac output is usu
or intrarenal) — demonstrate more consistent relationships with pathophysiology and ally increased during the initial stage of sepsis. Studies
can improve therapeutic approaches
in large animal models have also demonstrated that the
• Broad aetiology-based classification may still be insufficient, as heterogeneity could renal circulation participates in the systemic vasodila
exist at the molecular level; however, whether this heterogeneity leads to differences
tation of sepsis, but despite an increase in renal blood
in response to therapy is not yet known
flow (RBF), oliguria occurs and AKI develops within
• Protein biomarkers and other in vitro diagnostics are likely to have a role in both
hours20,21. This dissociation between GFR and RBF can
characterizing clinical phenotypes of AKI and aiding the discovery of new
endophenotypes, with the ultimate goal of matching subsets of patients to effective
be explained by alterations in the balance of efferent and
therapeutic approaches afferent glomerular arteriolar tone and decreased renal
perfusion pressure22 (FIG. 1). For example, a reduction in
GFR can be induced by a combination of systemic hypo
injuries. Conversely, it is unclear to what extent differing tension and efferent arteriole vasodilation, which causes
aetiologies of AKI constitute distinct paradigms (that is, the intraglomerular filtration pressure to drop below the
distinctive phenotypes caused by differing pathophysio required threshold for effective ultrafiltration despite
logical mechanisms), which demand specific treatments normal glomerular perfusion. Such changes should be
and confer unique prognoses. In this Review, we discuss reversible following systemic haemodynamic normal
the differing causes and clinical contexts of AKI that ization such as that induced by vasopressor therapy
have been identified9, including a discussion of their (for example, noradrenaline). The reversibility of these
common and distinguishing features. We attempt to haemodynamic changes is evidenced by a comparison
identify paradigms that might inform our therapeutic of renal function, perfusion and histological changes
approach and draw parallels and contrasts between these in sheep experiencing septic shock23, which showed no
settings in terms of their epidemiology, pathophysiology change in RBF and renal oxygen consumption, with
and outcomes. Given the wide range of aetiologies that histological alterations limited to minor focal mesan
can cause AKI, we focus on AKI that typically occurs in gial expansion, suggesting that mechanisms other than
the intensive care setting. RBF and oxygenation contribute to the development of
AKI in sepsis. For scenarios in which RBF does decrease
Sepsis-associated AKI during sepsis, this change may be a consequence of AKI
Epidemiology. Sepsis is the leading condition associ rather than a cause. For example, a progressive increase
ated with AKI in the hospital and intensive care unit in renal vascular resistance occurred 18–22 hours after
(ICU)5,9–11. Similar to AKI, sepsis is a disease of elderly induction of sepsis in a porcine sepsis model, but only
individuals and is substantially associated with risk in animals with AKI. These haemodynamic changes
of death in the hospital12. Globally, sepsis is found in were preceded by substantial increases in plasma pro-
almost 50% of patients with severe AKI in the ICU9,13. inflammatory cytokines (such as IL‑6 and tumour
An analysis of US health-care databases including necrosis factor (TNF)) in the animals with AKI24, sug
nearly 200,000 individuals across seven states identi gesting that renal vasoconstriction occurs in response
Inflammatory mediators
fied AKI in 22% of patients with diagnostic codes for to inflammatory injury rather than being the initiating
A wide array of substances that severe sepsis, which was associated with 38.2% mortal event of renal injury.
mediate and modulate various ity 12. In Europe, a 51% rate of AKI has been reported in Similarly, in clinical sepsis, these early haemodynamic
aspects of inflammation. These patients with sepsis, with an associated ICU mortality of changes with increased cardiac output and vasodilation
substances include vasoactive
41%14. Thus, sepsis is likely to be at least a contributing are likely to be accompanied by endothelial and renal
proteins (for example,
bradykinin, histamine), factor to AKI in many cases, and an understanding of tubular cell inflammatory injuries that consequently
complement and molecules the mechanistic basis of septic AKI is essential for the induce glomerular hypofiltration, which becomes refrac
involved in coagulation (for development of improved therapeutic approaches for tory to global haemodynamic manipulation as afferent
example, plasmin, thrombin). individuals with septic AKI. vasoconstriction occurs in established AKI22.
Cytokines (for example, TNF,
IL‑6, IL‑10), chemokines (for
Many mechanisms by which septic AKI causes
example, IL‑8) and eicosanoids Pathophysiology. Sepsis is characterized by a systemic renal tubular injury have been proposed, including
(for example, leukotrienes, inflammatory response to infection. The pathogenesis ultrafiltration of circulating microbial toxins and the
prostaglandins) are the major of septic AKI is still not fully understood; however, pro release of inflammatory mediators that trigger tubular cell
mediators of inflammation
found differences are apparent between experimental stress and injury 25. Circulating toxins might act on the
during infection. Although
some molecules are often models of ischaemic AKI (see below) and related clini endothelium, which triggers reduced microcirculatory
labelled pro-inflammatory cal settings. Post-mortem studies of patients with septic flow and interstitial infiltration of inflammatory cells26.
(for example, IL‑6) and others AKI revealed heterogeneous tubular cellular injury with Concurrently with these inflammatory processes, local
anti-inflammatory (for example, apical cellular vacuolization but without the character ischaemia can still occur despite increased RBF due to
IL‑10), the actions of each
mediator may be complex and
istic features of extensive tubular apoptosis or necrosis alterations in microcirculatory flow associated with
context-dependent, making found in severe ischaemic injury 15. Similarly, necrosis is endothelial activation as well as the effects of locally
simple classification difficult. uncommon in experimental septic AKI16. and systemically acting inflammatory mediators (such
218 | APRIL 2018 | VOLUME 14 www.nature.com/nrneph
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Damage-associated as TNF and transforming growth factor‑β (TGFβ)). induces angiopoietin 2 expression and release, reduces
molecular patterns These alterations cause redistribution of perfusion angiopoietin 1 receptor activation and leads to vascular
(DAMPs; also known as away from the renal medulla to the cortex, leading to leakage33. Renal tubular responses to this inflammatory
danger-associated molecular medullary hypoxaemia27–30, which implies intrarenal milieu — including autophagy, mitochondrial dys
patterns). Endogenous
molecules often released from
shunting 31. The inflammatory processes involved in function, loss of cell polarity and, to a limited degree,
damaged tissues or dying cells. septic AKI might be mediated by Toll-like receptors necroptosis and apoptosis34 — lead to sustained AKI
They can be detected by (TLRs) expressed on tubular and endothelial cells that and potentially to fibrosis and development of chronic
various receptors on cells, recognize damage-associated molecular patterns (DAMPs) kidney disease (CKD).
including TLRs and receptor for
and pathogen-associated molecular patterns (PAMPs), Finally, the relationship between inflammatory
advanced glycosylation end
products (RAGE; also known as
such as lipopolysaccharide, as well as receptors for responses and AKI in sepsis might not be unidirec
AGER). Typical DAMPs include cytokines and other inflammatory mediators32. Receptor tional. One study reported that in 40% of ICU patients
high mobility group protein B1 activation then triggers local release of additional with sepsis and AKI, sepsis occurred after the onset of
(HMGB1), RNA, DNA and pro-inflammatory mediators and the recruitment of AKI; however, this number is likely to be an underesti
myoglobin.
peritubular inflammatory infiltrating cells. Sepsis also mate because AKI diagnosis based on serum creatinine
Pathogen-associated
molecular patterns
(PAMPs). Similar to DAMPs, Box 1 | Definitions and concepts of acute kidney injury
PAMPs are molecules released
from pathogens. Many of the The standardization of definitions and diagnostic criteria into three stages based on serum creatinine level and urine
same receptors that recognize output122,123 (see the table) has been crucial in advancing the field of acute kidney injury (AKI). These stages serve as the
DAMPs also recognize PAMPs, basis for AKI diagnosis, biomarker discovery and validation118 and aid epidemiological studies as well as patient
leading to similar cellular stratification in clinical trials. Furthermore, the staging specified by these definitions has been validated in terms of their
responses when either are
associations with the short-term and long-term risks of death and end-stage renal disease3,4. However, this
encountered. Typical PAMPs
include lipopolysaccharide
standardization obscures the reality that AKI is a collection of extremely heterogeneous clinical syndromes. For example,
(LPS; also known as endotoxin), utilizing the Kidney Disease: Improving Global Outcomes (KDIGO) definition, AKI may manifest as changes in only serum
lipoteichoic acid from creatinine (12% of patients), only urine output (38%) or both (50%)124. Importantly, these varying manifestations are
Gram-positive bacteria, strongly associated with different outcomes: hospital mortality within these groups is 9.2% (only serum creatinine),
peptidoglycan and nucleic acid 7.5% (only urine output) and 26.7% (both), and a similar pattern exists for 1‑year survival124.
variants normally associated Taking these differences into account, understanding of the underlying processes that cause the physiological changes
with viruses. leading to AKI is of paramount importance. Creatinine excretion decreases during a sustained decrease in glomerular
filtration rate (GFR), which causes serum creatinine concentration to increase over time until creatinine excretion once
again equals production at the reduced GFR. Similarly, a sustained period of low urine output (oliguria) can be caused by
either an intact urinary-concentrating mechanism that works at increased capacity or a system that has failed because of
injury, in which GFR is so low that urine output cannot be maintained. In this light, more severe oliguria can be seen as an
additional marker of AKI severity through the indication of a substantial decline in GFR that may be difficult to appreciate
from early changes in serum creatinine in the dynamic setting of acute illness. For example, in the AWARE study,
a substantial number of AKI cases in children were missed when urine output was not considered125. Certain aetiologies
for AKI seem more likely to manifest as oliguric (such as sepsis and cardiorenal syndrome) or non-oliguric (such as
nephrotoxicity); however, this observation may be due to the systemic physiological milieu in these conditions (for
example, vasodilatory shock in sepsis). Thus, although both urine output and serum creatinine can indirectly give insight
into renal excretory function and are important as indicators of organ dysfunction and the potential need for supportive
therapy, in isolation, they give little information about the underlying renal pathology.
In addition, certain clinical conditions are usually termed ‘AKI’, whereas other conditions that may meet the
biochemical definition are generally not categorized as AKI because they constitute specific diagnoses. The term ‘AKI’
generally excludes specific disease states that cause acute renal dysfunction due to transient urinary obstruction unless
actual cellular damage has occurred as a result. Similarly, intrinsic renal conditions such as glomerulonephritis or
interstitial nephritis are usually thought of as specific diseases that are part of the differential diagnosis for AKI, but they
are uncommon causes. Instead, the term ‘AKI’ often refers to a syndrome of renal dysfunction arising in the context of a
systemic illness or toxin exposure, usually pathologically manifested as renal tubular cell dysfunction or injury, utilizing
other terms for intrinsic renal diagnosis such as glomerulonephritis. Thus, the ‘modern concept of AKI’ is a disorder
caused by a variety of haemodynamic, toxic and inflammatory insults, often occurring in combination, that result in a
disease spectrum ranging from a transient reduction in GFR — with, at most, mild tubular dysfunction — to severe
tubular injury, resulting in sustained anuria for days to weeks. Thus, in some aspects, this concept recapitulates the
historic categories of ‘prerenal failure’ and so‑called acute tubular necrosis, which are not truly distinct clinical entities
but extremes in a spectrum of the severity and nature of injury in the AKI syndrome. However, this observation does not
mean that diagnostic evaluation should focus on distinguishing transient or reversible AKI from established injury as this
approach historically has not proved useful owing to broad clinical overlap.
AKI KDIGO stage Serum creatinine Urine output
1 1.5–1.9 × baseline in 7 days or ≥0.3 mg/dl (26.5 μmol/l) in 48 h <0.5 ml/kg per h for 6–12 h
2 2.0–2.9 × baseline <0.5 ml/kg per h for ≥12 h
3 ≥3 × baseline or ≥4.0 mg/dl (35.4 μmol/l) or initiation of RRT <0.3 ml/kg per h for ≥24 h
or eGFR <35 ml/min/1.73 m2 in patients aged <18 years or anuria for ≥12 h
eGFR, estimated GFR; RRT, renal replacement therapy.
NATURE REVIEWS | NEPHROLOGY VOLUME 14 | APRIL 2018 | 219
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
is often delayed35. Another study found that bacterial of the more well-established literature on the effects of
invasion and lung injury were more severe in mice with CKD on innate immune pathways and, taken together,
experimental AKI and pneumonia than in mice support a key role for the kidney in the regulation of
with pneumonia alone. Moreover, neutrophils isolated immune function37–39.
from mice with AKI had impaired function in vitro
compared with that of wild-type mice36. Together with Outcomes. Because of a lack of studies, the long-term
the emerging literature on the various pathophysio effects of septic AKI, or indeed the long-term effects of
logical effects of AKI11, these results provide evidence sepsis in general, are not well understood40. However, the
supporting an effect of AKI on the immune system and inflammation associated with septic AKI is coupled to
on the risk of sepsis. These findings are also reminiscent long-term outcomes, as elevated plasma concentrations
Macrocirculation
Anaesthesia Major surgery Infection Kidney
Blood and Antimicrobial drugs
Redistribution of
fluid losses perfusion away
Venodilation from renal medula
Cardiopulmonary Tissue injury
bypass
Myocardial Obstruction
depression to venous
Hypovolaemia outflow
Arteriodilation Elevated
intrarenal
Capillary pressure
leakage Innate and acquired
Systemic
immune responses
hypotension
Extrinsic
renal
compression
Circulating mediators
↓ Renal
Large-volume perfusion
fluid resuscitation Sympathetic nervous pressure
system activation
Interstitial oedema Efferent
and fluid overflow arteriole
Afferent arteriole constriction dilation
Tubuloglomerular
feedback
Peritubular Proximal
Interstitium capillary tubule Lumen Intraglomerular
hypotension
↑ Tubular
Endothelial pressure
activation and Filtered
injury mediators
↓ GFR
Loss of Impaired urinary
endothelial concentrating Tubular
cell–cell Rouleaux capacity cell injury
junctions formation
↑ Capillary Tubular cell injury
permeability • De-differentiation
• Loss of cell–cell junctions Nephron
Leukocyte– Cytokines • Cell shedding
endothelial Chemokines Oxidative
stress • Vacuolation
adhesion and • Loss of polarity • Baseline O2 supply
interaction • Loss of transmembrane channels dependence
Larger O2 • Mitochondrial dysfunction • Oxidative stress
Coagulation Transendothelial diffusion • G1 cell-cycle arrest
Impaired migration distances • Apoptosis
blood flow
Renal microcirculation
Potential for rapid reversibility Red blood cell Inflammatory cell DAMPs Cytokines Cell adhesion
molecule
Likely to be associated with Dendritic cell TLRs PAMPs Toxins
sustained AKI Platelets
Nature Reviews | Nephrology
220 | APRIL 2018 | VOLUME 14 www.nature.com/nrneph
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
of inflammatory and apoptosis biomarkers (such as IL‑8) is whether known or novel biomarkers can predict the
have been associated with nonrecovery of renal function subsequent risk of cardiovascular events or recurrent
and death in critically ill patients receiving renal replace infection after an episode of AKI with or without evi
ment therapy (RRT)41. These data suggest that sepsis and dence of renal recovery. This level of understanding is
AKI have long-term effects on inflammation, coagula necessary so that interventions (such as statin treatment
tion and possibly other systems that might be critical in or immune stimulation) can be developed for patients
determining long-term outcomes as well as in identifying at risk of long-term sequelae, as opposed to waiting for
potential targets for therapy. However, septic AKI might these events to occur.
represent a different phenotype from that of other forms
of AKI that have inflammation and bioenergetic failure Surgery-associated AKI
as major pathophysiological features (for example, AKI Epidemiology. Surgery and trauma have long been
secondary to trauma or major surgery). In patients with recognized as a leading cause of AKI in hospitalized
sepsis-associated AKI, renal recovery — even partial patients46,47. According to crude estimates, 310 million
recovery — seems to confer significant benefits such that surgical procedures were undertaken worldwide in 2012,
1‑year survival is indistinguishable from that of patients an increase of one-third in 8 years48. In the USA, 1.5
with sepsis but without AKI42. However, this seemingly million patients develop a medical complication within
good prognosis for patients with renal recovery may dis 30 days after surgery, and at least 150,000 patients die
guise substantial underlying kidney damage that could each year 49. Importantly, AKI occurring after surgery is
take years to manifest. Specifically, it will be important to strongly associated with risk of death50–55.
determine whether septic AKI increases the risk of CKD Employing modern consensus definitions of AKI
years later, even in patients who recover renal function (BOX 1), the incidence of AKI among patients under
prior to hospital discharge. For example, whether these going surgery varies by surgical setting: ~18% of patients
patients are left with interstitial fibrosis and tubular atro undergoing cardiac surgery develop AKI56 compared
phy or demonstrate apparent recovery from AKI due to with ~13% of patients undergoing major abdominal
hyperfiltration in remaining nephrons, which ultimately surgery; however, the incidence is ≥50% in procedures
leads to glomerulosclerosis, should be investigated. If so, such as liver transplantation or emergency aortic sur
angiotensin-converting enzyme (ACE) or angiotensin gery 55. Although most surgery-associated AKI is mild,
receptor inhibition might be effective at preventing pro these complications remain consistently associated
gression of CKD, as has been shown in animal models with greater short-term and long-term risks of death,
of AKI and CKD43–45. Determining whether septic AKI especially in cases of severe AKI46,57.
increases the risk of cardiovascular events and/or infec
tion even in the absence of CKD is also important, as Pathophysiology. Multiple aetiological factors predis
pose to perioperative AKI; depending on the surgi
cal context, these include haemodynamic alterations,
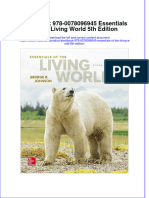
◀ Figure 1 | Principal pathogenic mechanisms of acute kidney injury in the context of exposure to exogenous and endogenous nephrotoxins,
sepsis or major surgery. In both settings, alterations in systemic and glomerular
ischaemia–reperfusion injury, renal artery embolization,
haemodynamics — arising from the vasodilatory effects of systemic inflammatory
mediators or anaesthesia, decreases in actual or effective in plasma volume and activation of neurohormonal responses to hypotension
myocardial depression — may cause an early decrease in glomerular filtration rate (GFR) and tissue injury (the sympathetic nervous system and
with potential for rapid reversibility (dotted arrows). Depending on the clinical context, the renin–angiotensin–aldosterone system), inflam
these changes can be associated with high, normal or low cardiac output. However, both mation and oxidative stress. However, as these factors
sepsis and tissue injury in surgery result in the generation of damage-associated coexist and influence each other throughout the peri
molecular patterns (DAMPs) — including high mobility group protein B1 (HMGB1), operative period, determining the extent to which
histones, cell-free RNA and DNA, ribonuclear proteins, S100 proteins and heat-shock individual components contribute to the development
proteins — or pathogen-associated molecular patterns (PAMPs) — prototypically of AKI is difficult. Furthermore, patients requiring sur
lipopolysaccharide but also including a vast array of other bacterial-specific or gery often have multiple comorbidities (for example,
viral-specific molecules. These ‘molecular patterns’ are recognized by Toll-like receptors
CKD, diabetes, hypertension and heart disease) that
(TLRs), triggering systemic and local release of pro-inflammatory mediators, such as IL‑1,
IL‑2, IL‑6, IL‑8 IL‑12, IL‑18, transforming growth factor‑β (TGFβ), tumour necrosis factor may impair renal autoregulation, chronically activate
(TNF), IFNγ, C‑C chemokine ligand 2 (CCL2) and CCL5. Furthermore, antimicrobial drugs neurohormonal responses and predispose to tubular
that are used for the treatment of infections can contribute to nephrotoxicity (FIG. 3). injury. The prevalence of comorbid conditions might be
The effects of DAMPs and PAMPs are combined with those of specific immune particularly high in specific high-risk surgical contexts
responses and the generation of other inflammatory mediators, including products of such as among patients undergoing cardiac and vascular
coagulation and complement activation, leading to the recruitment of a peritubular surgery 55. Importantly, pre-existing CKD is an impor
inflammatory cell infiltrate (neutrophils, monocytes, macrophages and lymphocytes). tant risk factor for postoperative mortality 58 and has
Importantly, these circulating toxins and mediators may act directly on the endothelium been consistently identified as the strongest risk factor
or may be filtered in the glomerulus, where they interact with tubular cells and cause for perioperative AKI51,52,59.
injury. The renal inflammatory response can cause injury to the endothelium,
Multiple factors and procedures can result in haemo
microcirculation and tubular cells. If this damage is severe, it will lead to sustained
clinical acute kidney injury (AKI) that is unresponsive to the correction of systemic dynamic instability during surgery, including the dila
haemodynamic abnormalities. Finally, during critical illness, the effects of fluid overload, tory properties of anaesthetic agents, blood and fluid
elevated venous pressure and development of abdominal compartment syndrome can losses, poor cardiovascular reserve and artificial circu
also contribute to the persistence of AKI by an increase in tubular pressure and reduction lation during cardiopulmonary bypass (CPB) (FIG. 1).
of glomerular perfusion. Importantly, appropriate management of intraoperative
NATURE REVIEWS | NEPHROLOGY VOLUME 14 | APRIL 2018 | 221
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
haemodynamic changes, and preoperative and postoper intravenous radiocontrast agents. Some of these com
ative optimization of intravascular volume, cardiac out pounds predominantly affect renal haemodynamics,
put and oxygen delivery is associated with a substantial whereas others are directly nephrotoxic (see below). In
reduction in the incidence and severity of periopera addition, release of endogenous nephrotoxins — such as
tive AKI among high-risk patients60,61. In retrospective myoglobin in trauma and haemoglobin or free haem in
analyses of noncardiac surgical populations comprising CPB — may also cause AKI.
~5,000 patients, the presence of intraoperative hypo
tension was predictive of adverse cardiac-related and Outcomes. Despite great heterogeneity in its patho
renal-related outcomes62,63, with the risk increasing in physiology, perioperative AKI of any severity remains
association with the duration and severity of hypo associated with an ongoing increased risk of death,
tension for individuals with a mean arterial pressure even many years after surgery. For example, patients
<65 mmHg (REF. 64). Overall, the relationship between with RIFLE (risk, injury, failure, loss, and end stage)
haemodynamics and AKI during surgery suggests a role stage F after cardiothoracic surgery have a significantly
for altered renal perfusion in the development of post lower survival over 10 years than patients without AKI
operative AKI. In some circumstances, such as in aortic (adjusted HR 2.14, 95% CI 1.73–2.66)73. Importantly —
surgery, this alteration may be unmistakably ischaemic, and unlike what has been observed in sepsis-associated
whereas in other cases, changes in GFR may be rapidly AKI — even in cases of complete resolution, periopera
reversible, with a correction of haemodynamics in the tive AKI is associated with increased risks of CKD and
absence of other sources of renal injury. For example, death in the years after surgery 52,73–78. After cardiac sur
experimental reduction of RBF to 10% of baseline levels gery in particular, perioperative AKI is also associated
causes an abrupt loss of glomerular filtration but is com with higher risks of CKD78, end-stage renal disease78
pletely and rapidly reversible with restoration of normal and death79,80. Importantly, as serum creatinine levels
RBF in the absence of other renal insults65. Conversely, tend to fall during hospitalization for surgery, an overt
in a porcine animal model of aortic cross-clamping, RBF decline in renal function may not be evident at the point
and microvascular oxygenation were initially compara of hospital discharge in patients who have apparently
ble to those of control animals but rapidly fell over the recovered from perioperative AKI. This decline might
next 4 hours after release of a suprarenal clamp66. This become apparent only at follow-up54, which partially
observation suggests that evolving reperfusion injury explains the poor prognosis and emphasizes the need
in the context of surgery compromises renal micro for long-term follow‑up.
circulation and macrocirculation rather than having an
immediate effect of ischaemia. AKI associated with renal hypoperfusion
Both cardiac and noncardiac surgical proce Epidemiology. Aetiologies of AKI that are compatible
dures result in a systemic immune and inflammatory with sustained renal hypoperfusion — such as major
response to injury as well as the release and recognition obstetric haemorrhage and crush injury with prolonged
of DAMPs67. Such responses are well recognized in the extraction — as well as exposure to potent exogenous
context of CPB procedures, in which these responses are nephrotoxins or similar insults, including incompatible
thought to be triggered by contact between blood and blood transfusion, were commonly reported in the 1940s
the artificial surfaces of the CPB68. Although the exact and 1950s81. These observations led to the concept that
contribution of the upregulated inflammatory response tubular necrosis is the dominant pathology of AKI, which
to kidney injury in humans undergoing CPB is not translated into widespread popularity that continues to
known, it is likely to be substantial69. In a multicentre this day, even in the use of animal models of AKI caused
cohort study including 960 individuals, increased post by renal ischaemia–reperfusion injury or exposure to
operative concentrations of both pro-inflammatory and potent nephrotoxins. However, AKI that is directly
anti-inflammatory cytokines (IL‑6 and IL‑10, respec attributable to a gross reduction in RBF is less common in
tively) were associated with an increased risk of AKI after contemporary, integrated, medical settings in the devel
cardiac surgery, demonstrating a correlation between oped world. Nevertheless, severe reductions in RBF can
systemic inflammatory responses and AKI70. It should still occur, most commonly in specific contexts, such as
be noted that this relationship may also be bidirectional, following abdominal aortic dissection, sustained cardiac
given the importance of the kidney in clearing inflam arrest or exsanguinating trauma. It should be noted that
matory mediators from the circulation71. Sustained sys even in cardiac arrest, in which RBF can be very low for
temic inflammatory responses are also common after a long period, development of AKI is not universal and
major abdominal surgery, and increased IL‑6 production is most strongly associated with persistent cardiogenic
and upregulation of TLR4 and TLR5 expression in the shock in the period after arrest 82. Therefore, it seems that
postoperative period have been proposed as potential hypoperfusion is more commonly a contributing factor
biomarkers for increased AKI risk72. These responses are rather than the sole driver of AKI in many clinical set
also associated with the d evelopment of AKI in other tings. However, certain individuals have an inherently
settings such as sepsis. high risk of developing AKI following mild to moderate
Finally, patients undergoing surgery are exposed reductions in kidney perfusion owing to the presence of
to multiple potential nephrotoxins, such as antibiot comorbidities (such as chronic hypertension and diabe
ics, nonsteroidal anti-inflammatory drugs (NSAIDs), tes) and certain medications (for example, NSAIDs and
ACE inhibitors, angiotensin receptor blockers and calcineurin inhibitors)82. Conversely, even in situations
222 | APRIL 2018 | VOLUME 14 www.nature.com/nrneph
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
in which systemic ischaemia is not present, microcircula By contrast, in mild forms of AKI, changes in glo
tory abnormalities may cause local ischaemia at the tissue merular haemodynamics are reversible and may be
level. Although these abnormalities may be an impor associated with increased serum creatinine levels and
tant mediator of injury, they would not be expected to oliguria in the absence of severe tubular injury. Such
be responsive to vasopressor or fluid therapy targeted reversible AKI encompasses severe volume depletion
at the macrocirculation as the ischaemic insult occurs at or low cardiac output states that cause renal hypoperfu
the local tissue level rather than the whole-organ level. sion. Together, these different states have been consid
Thus, despite ischaemia being a historically dominant ered under the umbrella term ‘prerenal’ AKI; however,
paradigm of AKI, its epidemiology is difficult to define. considerable overlap exists in terms of risk factors and
For example, one epidemiological study attributed ~20% aetiologies with tubular injury, which may often evolve
of cases of RRT-requiring AKI in the ICU to cardiogenic in concert with acute haemodynamic changes that con
shock or hypovolaemia82, both of which are likely to be tribute to oliguria and/or a fall in GFR. Importantly,
associated with renal hypoperfusion but with differing cardiac dysfunction can reduce renal perfusion either
underlying causes and approaches to treatment. through decreased forward flow or by increasing back
pressure and venous congestion. Right-sided heart fail
Pathophysiology. Various pathophysiological states ure and raised venous pressure may actually be more
and medications can contribute to a reduction of important as a cause of cardiorenal syndrome than
RBF and have been described as causing generalized left-sided heart failure, especially in settings such as
or localized ischaemia in the kidney, leading to AKI83. cardiac surgery. As such, high venous pressures have
These contributing factors include intravascular volume been shown to predict deterioration of renal function
depletion and hypotension through internal or external in hospitalized patients with advanced chronic cardiac
fluid losses from the circulation (for example gastrointes failure; however, cardiac output and left ventricular
tinal bleeding, dermal losses and haemorrhage), condi function did not 86,87. This deterioration presumably
tions associated with chronic neurohormonal activation, occurs because the venous outflow pressure from the
systemic hypotension and fluid retention (for example, kidney is normally low but increases with right-sided
congestive heart failure and cirrhosis) and medications heart failure. Furthermore, because the kidney is in a
that cause renal vasoconstriction (for example, NSAIDs, poorly compliant capsule, it is more sensitive to venous
radiocontrast agents and calcineurin inhibitors) (FIG. 2). congestion. Pericardial disease, cirrhosis with ascites
Furthermore, endothelial and vascular injury after and even abdominal compartment syndrome88 can
ischaemia as well as the role of innate and adaptive produce similar results because they all increase back
immune responses in microcirculatory dysfunction after pressure on the kidney. Even in the absence of these
reperfusion are important in the pathogenesis of ischae disease manifestations, fluid overload itself can com
mic AKI83,84. Thus, the microvascular and inflammatory promise renal (and other tissue) perfusion89. Finally,
responses to reperfusion are likely to be key determinants loss of glomerular perfusion pressure can also occur in
of the clinical course of ischaemic AKI. Of note, owing to vasodilatory states with systemic hypotension — such
the anatomy of the nephron microcirculation, the renal as early septic shock and chronic liver disease — and
medulla and corticomedullary junction receive poorly through exposure to vasoactive nephrotoxins, poten
oxygenated blood in the context of renal hypoperfusion tially resulting in reversible, haemodynamically medi
and are therefore much less well perfused than the renal ated AKI despite preserved or elevated cardiac output.
cortex. As a consequence, these areas are susceptible to Taken together, reversible AKI can arise in very diverse
multiple sources of renal injury (inflammatory, oxida settings, and in practice, the dominant underlying
tive, ischaemic or toxic insults), particularly in zones of mechanism is often apparent only as the clinical course
the nephron (for example, in the proximal tubule) that of AKI progresses.
require high oxygen consumption for active ion trans
port. Thus, even without overt renal ischaemia, base Outcomes. In contrast to sepsis and surgery, less informa
line oxygen supply levels might render the renal tubules tion on clinical outcomes in settings of hypoperfusion-
susceptible to non-ischaemic renal injury and to subtle associated AKI is available. Patient outcomes are likely
disruptions of the renal microcirculation83. to be strongly determined by the underlying conditions,
Distinguishing whether a reduction in RBF is a cause with advanced chronic heart or liver failure conferring
or a consequence of already established AKI is also chal a poor prognosis. However, in the specific context of
lenging. Various studies have demonstrated that, once myocardial infarction-related cardiogenic shock, RRT-
established, all types of AKI may be associated with a requiring AKI has been shown to predict substantially
reduction in RBF, in many cases with normal systemic elevated short-term mortality as well as long-term risks
blood pressure and cardiac output 85. This observation of chronic dialysis and death90.
suggests that intrarenal factors specifically increase
renal vascular resistance in response to AKI, resulting in Nephrotoxic AKI
decreased RBF. Such renal vasoconstriction is mediated Epidemiology. The true contribution of nephrotoxicity
by the tubuloglomerular feedback mechanism and is to the incidence of AKI is difficult to determine given
therefore preferentially pre-glomerular, causing a dispro the inevitable indication bias in which the use of a
portionate decrease in glomerular filtration by reducing drug is associated with the presence of an underlying
both intraglomerular hydrostatic pressure and flow. disease state. In the ICU, some forms of nephrotoxic
NATURE REVIEWS | NEPHROLOGY VOLUME 14 | APRIL 2018 | 223
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Macrocirculation Heart Kidney
Redistribution of
perfusion away
Haemorrhage or from renal medula
hypovolaemia
Acute heart failure Obstruction
Low cardiac Central PE to venous
output Tamponade outflow
Cardiac arrest Elevated
Capillary Systemic intrarenal
leakage hypotension pressure
Venodilation Hypoperfusion
Arteriodilation ↓ Renal perfusion
pressure
Direct ischaemic Reperfusion
tissue injury injury
Activation of
sympathetic
system
Circulating inflammatory
mediators and toxins Afferent
arteriole ↓ GFR
constriction
Peritubular Proximal Efferent
Interstitium capillary tubule Lumen arteriole Intraglomerular
dilation hypotension
↑ Tubular
Endothelial pressure
activation and Tubuloglomerular
injury feedback
Filtered
Loss of mediators Impaired urinary
endothelial Tubular cell
concentrating
cell–cell Rouleaux injury
capacity
junctions formation
↑ Capillary Tubular cell injury
permeability • De-differentiation
• Loss of cell–cell junctions Nephron
Leukocyte– Cytokines • Cell shedding
endothelial Chemokines Oxidative
stress • Vacuolation
adhesion and • Loss of polarity • Baseline O2 supply
interaction • Loss of transmembrane channels dependence
Larger O2 • Mitochondrial dysfunction • Oxidative stress
Coagulation Transendothelial diffusion
migration • G1 cell-cycle arrest
Impaired distances • Apoptosis
blood flow
Renal microcirculation
Potential for rapid reversibility Red blood cell Inflammatory cell DAMPs Cytokines Cell adhesion
molecule
Likely to be associated with Dendritic cell TLRs Toxins Platelets
sustained AKI
Figure 2 | Principal pathogenic mechanisms of acute kidney injury in the context of global hypoperfusion.
Nature Low
Reviews | Nephrology
cardiac output and systemic perfusion may arise in the context of major haemorrhage, profound hypovolaemia or an
intrinsic or obstructive cause of acute heart failure or cardiac arrest. On the one hand, acute haemodynamic changes can
mediate reversible falls in glomerular filtration rate (GFR) after profound global hypoperfusion (dotted arrows). On the
other hand, both the direct effects of ischaemia and reperfusion on the kidney and the local and systemic effects of
damage-associated molecular patterns (DAMPs) and other inflammatory mediators produced in response to injury
and reperfusion may drive sustained acute kidney injury (AKI; solid arrows). The ongoing inflammatory nature of the
renal injury after the initial insult shares features with the pathogenesis of other forms of AKI (FIGS 1,3) and explains
the persistence of injury, even if systemic perfusion is restored, and may also be associated with a second
systemic vasodilatory response as commonly seen after resuscitated cardiac arrest. PE, pulmonary embolus;
TLRs, Toll-like receptors.
224 | APRIL 2018 | VOLUME 14 www.nature.com/nrneph
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
exposure are unavoidable, as >20% of the 100 drugs Outcomes. The long-term outcomes of nephrotoxic AKI
most frequently administered to adult patients are clas are not well established. Most cases of nephrotoxicity are
sified as nephrotoxic91. Reports suggest that nephro acute, non-oliguric and resolve with discontinuation of
toxicity contributes to ~8–60% of AKI among patients the causal drug. However, for some drugs, or when other
in hospital92–96, whereas in the ICU, drug nephrotoxi AKI risk factors coexist, mixed patterns of injury result
city has been reported to contribute to 19% of RRT- in heterogeneity of recovery. For example, in cisplatin-
requiring AKI cases9. Nephrotoxic exposure is likely mediated nephrotoxicity, the GFR decline tends to be
to be increasing 95 owing to the more aggressive med reversible, whereas tubular dysfunction may persist 103.
ical management of complex conditions with nephro A retrospective cohort study of 100 children with AKI
toxic drugs, in p articular in oncology and with bone in the context of high nephrotoxic exposure reported
marrow transplantation97. evidence of CKD 6 months after AKI in 70% of cases104.
Thus, in common with AKI in other settings, devel
Pathophysiology. To achieve adequate glomerular ultra opment of CKD might be a common and important
filtration, the renal vascular bed receives a dispropor consequence of nephrotoxic AKI.
tionately large blood flow fraction of the resting cardiac
output (20–25%) compared with most other organs. Understanding paradigms of AKI
Consequently, the renal vasculature, nephrons and the The scientific foundation for acute kidney injury. We
interstitium are exposed to large quantities of blood- have described AKI as a clinical syndrome that arises in
borne toxins (FIG. 3). Furthermore, tubular epithelial several prototypical acute settings, including sepsis, fol
cells are especially prone to toxic injury, as they concen lowing major surgery, in states of low cardiac output and
trate filtered toxins along the nephron and express spe nephrotoxin exposure and often in combination with
cific transporters that result in high intracellular uptake pre-morbid chronic risk factors. Within these settings,
of toxins and their metabolites. The biological effects of a number of common themes emerge with patterns of
nephrotoxins are highly varied. Injury to the kidney inflammatory, ischaemic and nephrotoxic renal injury
may occur secondary to renal haemodynamic altera that can occur with all of these exposures. Considerable
tions, tubular cell damage by direct toxicity or osmotic overlap exists even within these categories of injury; for
injury, obstruction of the tubular lumen due to precip instance, inflammatory mechanisms can mediate rep
itation, direct or indirect (immunological) interstitial erfusion injury after ischaemia or certain nephrotoxins,
inflammation and/or vascular injury triggering throm whereas abnormalities of microvascular flow can result
botic microangiopathy 98. Although haemodynamic- in local ischaemia in the settings of sepsis or toxic injury
mediated alterations in GFR may be rapidly reversible (FIGS 1–3). The extent of overlap is often difficult to pre
by withdrawal of the relevant toxin, long-term exposure dict at the point of clinical presentation. Furthermore,
to renal vasoconstrictors can result in chronic ischaemic in almost all settings, changes in GFR can be caused by
nephropathy. Importantly, some toxins are associated renal or systemic haemodynamic abnormalities and can
with multiple forms of injury, and patients are fre either be reversible or result in tubular cell injury.
quently exposed to multiple nephrotoxins at the same Importantly, the apparent return of GFR to normal
time. In addition to drug-related causes, haemoglobin levels may not guarantee resolution of AKI105, as the
or myoglobin, released to the bloodstream through remaining nephrons may increase their function to
haemolysis or myocyte injury, may act as endogenous maintain GFR while masking nephron loss and tubular
nephrotoxins in the kidney by mechanisms similar to atrophy. Thus, clinical assessment of pathological versus
those of exogenous nephrotoxins through causing oxi physiological reductions in GFR may be impossible.
dative and inflammatory stress as well as having vaso As described in this Review, strong clinical reasons
active effects (for example, by depletion of endothelial cast doubt on the notion that all AKI syndromes are cre
nitric oxide). ated equal in terms of their aetiology, pathogenesis and
As with hypoperfusion, nephrotoxic renal injury prognosis. Even among patients with septic AKI, some
may recapitulate the AKI pathophysiology seen in other seem to have a more ‘pure’ form of disease, whereas dis
settings. For example, the pathophysiology of cisplatin- ease progression in others is complicated by nephrotoxic
induced AKI involves multiple mechanisms, including exposures and complex underlying illnesses. Therefore,
proximal tubular injury, oxidative stress and vascu a rational clinical approach to an AKI diagnosis requires
lar injury in the kidney 99. Proximal tubular cell injury assessment of the underlying mechanisms to help estab
encompasses several different mechanisms in common lish a prognosis and identify potentially beneficial inter
with other forms of AKI, such as apoptosis, autophagy, ventions. At present, this approach relies on clinical
cell-cycle arrest and mitochondrial dysfunction. In addi assessment and serial measurement of serum creatinine
tion, the pro-inflammatory nature of cisplatin-induced and urine output until either recovery has occurred or
AKI has been well documented100,101: the chemotherapy nonrecovery has been established — usually requiring
drug induces the phosphorylation and subsequent trans several days or more105. However, novel diagnostics
location of nuclear factor‑κB, leading to transcriptional might one day provide greater insights into the likely
upregulation of inflammatory mediators, including TNF, short-term, medium-term and long-term courses of AKI.
which, in turn, induces the expression of other inflam Hence, well-defined animal models, human
matory cytokines and recruitment of inflammatory cells epidemiological studies and biological samples are
into the kidney tissue102. required to establish a better scientific foundation for
NATURE REVIEWS | NEPHROLOGY VOLUME 14 | APRIL 2018 | 225
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Macrocirculation Kidney
Nephrotoxins • Ciclosporin
• NSAIDs
• ACE inhibitors Chronic renal
• ARBs ischaemia
• IL-2
• Proton-pump inhibitors
• Gentamicin • β-Lactams
• Cisplatin • Allopurinol
Arteriodilation • Hydroxyethyl starch • Aristolochic acids
• Radiocontrast agents Allergic
• Myoglobin interstitial
• Haem and/or iron nephritis
Systemic ↓ Renal perfusion
hypotension pressure
• Mitomycin • ACE inhibitors
• Ciclosporin • Ciclosporin • ARBs
• NSAIDs • IL-2
• Radiocontrast • Aciclovir
agents • Foscarnet
• Myoglobin • Methotrexate
• Haem and/or iron • Myoglobin
Sympathetic nervous Efferent ↓ GFR
system activation arteriole
dilation
↑ Tubular
Peritubular Proximal Afferent pressure
Interstitium capillary tubule Lumen arteriole Intraglomerular
constriction hypotension
Endothelial Tubular
activation and obstruction
injury Tubuloglomerular
Filtered feedback
Loss of toxins
endothelial Impaired urinary Tubular cell
cell–cell Rouleaux concentrating injury
junctions formation capacity
↑ Capillary Tubular cell injury
permeability • De-differentiation
• Loss of cell–cell junctions Nephron
Leukocyte– Cytokines • Cell shedding
Chemokines Oxidative
endothelial • Vacuolation
stress • Baseline O2 supply
adhesion and • Loss of polarity
interaction • Loss of transmembrane channels dependence
Larger O2 • Mitochondrial dysfunction • Oxidative stress
Transendothelial
Coagulation migration diffusion • G1 cell-cycle arrest
Impaired distances • Apoptosis
flow
Renal microcirculation
Potential for rapid reversibility Red blood cell Inflammatory cell DAMPs Cytokines Cell adhesion
molecule
Likely to be associated with Dendritic cell TLRs Toxins Platelets
sustained AKI
Figure 3 | Principal pathogenic mechanisms of acute kidney injury in the context of exogenous and
Nature Reviews | Nephrology
endogenous nephrotoxins, including typical examples. Many potential pathways for nephrotoxicity exist, and
individual nephrotoxins may exploit more than one mechanism. Changes in systemic and/or glomerular haemodynamics
may mediate changes in the glomerular filtration rate (GFR) related to nephrotoxin exposure; however, direct tubular
cellular injury from filtered toxins or (in some cases) direct toxic endothelial injury (including thrombotic microangiopathy)
is more likely to lead to acute kidney injury (AKI) that is sustained even with withdrawal of the toxic exposure. The
inflammatory response to tissue injury may be important in potentiating and sustaining the initial toxic insult, with
mechanisms in common with other AKI settings (FIGS 1,2). In addition to direct cellular injury, tubular obstruction by
precipitates of substances filtered and concentrated along the nephron is an important mechanism of nephrotoxicity.
Finally, chronic ischaemia from renal vasoconstrictor exposure and drug-induced allergic tubulointerstitial nephritis may
present subacutely with worsening renal function due to nephrotoxin exposure with distinct pathogenesis from the
typical AKI mechanisms discussed elsewhere in this Review. Importantly, acute and chronic nephrotoxin exposure often
involves multiple agents and occurs in the context of other AKI aetiologies further overlapping with mechanisms
illustrated in FIGS 1,2. ACE, angiotensin-converting enzyme; ARBs, angiotensin receptor blockers; DAMPs,
damage-associated molecular patterns; NSAIDs, nonsteroidal anti-inflammatory drugs; TLRs, Toll-like receptors.
226 | APRIL 2018 | VOLUME 14 www.nature.com/nrneph
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Table 1 | Selected clinical and preclinical studies exploring acute kidney injury endotypes
Model systems Technique Findings Potential clinical benefit Refs
Comparison of ischaemia– Microarray analysis Spatiotemporal differences in RNA • Improved diagnosis 108
reperfusion-induced and mercuric expression levels, such as haem oxygenase 1. • Identification of drug
chloride-induced rat models of AKI targets
Comparison of ischaemia– Chromatin Upregulated expression of some genes (such Identification of potential 109
reperfusion-induced and immunoprecipitation as those encoding TNF and NGAL) in both drug targets
LPS-induced mouse models of AKI models with some insult-specific expression
patterns.
Porcine model of septic AKI Whole-kidney gene Differences in gene expression between • Identification of 110
expression analysed by sepsis AKI and sepsis without AKI. potential drug targets
quantitative real-time PCR Inflammation, metabolism and apoptotic • Guiding mechanistic
molecular responses in early septic AKI. research
• Dehydration versus ischaemia– • RNA sequencing of Activated genes included different, • Identification of 112
reperfusion injury in mice specific kidney regions functionally unrelated signal transduction potential drug targets
• Humans with brief (<72 h) isolated by laser pathways and were expressed in different • Guiding mechanistic
or long-term (>7 day) AKI microdissection regions of the kidney. Brief and long-term research
• RNA sequencing of AKI in humans also showed different RNA
human urine expression.
NGAL luciferase reporter assays NGAL expression via LPS resulted in kidney NGAL expression, Clarify specificity of NGAL 113
in mice exposed to dehydration luciferase reporter whereas a 50% increase in creatinine with for intrinsic AKI
versus LPS dehydration did not.
Multicentre study of 744 patients 340 candidate molecules Urinary TIMP2 and IGFBP7 were topic Discovery and validation 117,
with a mixed aetiology of AKI examined in urine and candidates in discovery and validation of biomarkers 118
plasma for stage 2–3 AKI within 12 h. TIMP2 was
somewhat better for septic AKI according
to the AUC.
AKI, acute kidney injury; AUC, area under the curve; IGFBP7, insulin-like growth factor-binding protein 7; LPS, lipopolysaccharide; NGAL, neutrophil gelatinase-
associated lipocalin. TIMP2, tissue inhibitor metalloproteinases 2; TNF, tumour necrosis factor.
phenotyping AKI. Although current animal models fail genes differentially expressed according to the specific
to recapitulate the multiple renal insults and comorbid type of renal injury 109. Not only might transcriptional
diseases that are present in most clinical cases of AKI, changes reflect the nature of the injury but also the elici
understanding the common features and differences ted host response. For example, in a porcine model of
among the various causes of AKI that may coexist within septic AKI, only 50% of animals developed AKI despite
an individual may be established by studying phenotypes similar initial haemodynamic responses to experimental
of pure forms of AKI. Progress in AKI research has also sepsis; however, development of AKI was preceded by
been substantially limited by a lack of available patientthe differential expression of genes with inflammatory,
biopsy tissue, as emphasized by multiple investigators106.
metabolic and apoptotic functions110. Beyond the level
Furthermore, as AKI contributes to the development of of gene expression, microRNAs (miRNAs) play a cru
CKD107, patient biopsy samples could represent a con cial part in the post-transcriptional regulation of almost
siderable asset to the scientific communities trying to all biological cell functions. In this regard, alterations in
understand this relationship. levels of circulating tissue miRNAs have been demon
strated in several experimental and clinical AKI settings,
Endophenotyping of acute kidney injury. Apart from with some miRNAs commonly detected across many
describing the paradigms of AKI by aetiology, several forms of AKI and others u pregulated or downregulated
investigators have also sought to define AKI subtypes in specific circumstances111.
by examining patterns of gene expression in response to RNA sequencing (RNAseq) of anatomically dis
kidney injury. These subtypes are sometimes referred tinct domains of the kidney from ischaemic AKI and
to as ‘endophenotypes’ or simply ‘endotypes’ to distin volume-depletion mouse models, which cause a simi
guish them from phenotypes that are directly observ lar rise in serum creatinine levels, revealed distinct and
able without the aid of molecular diagnostics. In a largely nonoverlapping sets of genes that are expressed
comparison of ischaemia–reperfusion-induced and in response to these differing renal insults112. Similar
nephrotoxin (mercuric chloride)-induced rat models differences were seen among urinary proteomic pro
of kidney injury, spatiotemporal differences of renal files of selected cases of human AKI with rapidly revers
transcriptomes were reported108 (TABLE 1). Similarly, in ible (<72 hours) or sustained (≥7 day) time courses112.
another comparison study of ischaemia–reperfusion- In murine models, ischaemic AKI was accompanied by
induced and lipopolysaccharide-induced AKI mouse expression of genes related to cytokines and inflamma
models, transcriptional and epigenetic heterogeneity tory mediators, the cell cycle, coagulation and TLR sig
was observed, with some genes (for example, those nalling, whereas volume depletion was associated with
encoding TNF and neutrophil gelatinase-associated a smaller set of activated genes associated with bioener
lipocalin (NGAL)) commonly upregulated but other getics and cellular transport 112. This study suggests that
NATURE REVIEWS | NEPHROLOGY VOLUME 14 | APRIL 2018 | 227
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Recovery Good health Furthermore, patients with increased AKI biomarkers
(NGAL or kidney injury molecule 1 (KIM1; also known
Delayed recovery as HAVCR1)) but without significantly elevated serum
creatinine levels remained at increased risk of a com
CVD and other posite of dialysis or death compared with those without
AKI Nonrecovery complications
increased NGAL, KIM1 or creatinine levels114.
Indeed, the concept of ‘subclinical AKI’ has been sug
CKD gested as a way to understand kidney injury detected by
biomarkers in cases that are clinically ‘silent’ in terms of
Death (early) AKI AKD AKI Death creatinine level and urine output115. However, NGAL has
proved less discriminating in the development of septic-
Time
associated or adult cardiac-surgery-associated AKI than
in other types of AKI, possibly because subclinical AKI
Days to weeks Weeks to months Months to years
is common in these settings or because neutrophils
themselves may be a source of NGAL in the setting of
Figure 4 | Potential patient outcomes following acute systemic inflammation116. Conversely, tissue inhibitor
kidney injury. As a result of anNature
episodeReviews | Nephrology
of acute kidney of metalloproteinases 2 (TIMP2) and insulin-like growth
injury (AKI), patients may recover, be discharged without factor-binding protein 7 (IGFBP7), which are involved
recovery of renal function or die. Patients who seem to
in G1 cell-cycle arrest, were shown to predict the devel
recover may also later develop chronic kidney disease
(CKD) or cardiovascular disease (CVD) (dashed lines).
opment of severe AKI in both adults and children after
Although information exists on in‑hospital events and final ICU admission in the context of sepsis, surgery, trauma
outcomes, the pathways leading to these outcomes are and nephrotoxic exposure117,118. As G1 cell-cycle arrest
virtually unknown. Owing to the high complexity, not all is a common response to tubular injury, these mark
relationships are displayed. AKD, acute kidney disease. ers might reflect the presence of injury rather than the
underlying aetiology. However, some differences exist
in terms of the ability of these biomarkers to identify
although volume depletion and ischaemia–reperfusion different AKI insults, with TIMP2 and IGFBP7 being
both involve renal hypoperfusion, they represent very better discriminants of AKI in the contexts of sepsis and
different clinical entities, with confirmation of the surgery, respectively 117,119.
importance of inflammatory pathways in ischaemia– Biomarker signatures might also improve disease
reperfusion leading to sustained renal impairment. prognosis. Although uncertainty remains regarding the
This differing pathology might not be evident from determinants of long-term outcomes in AKI120 (FIG. 4),
a snapshot assessment of serum creatinine level but various studies have reported that plasma biomarker
will become evident as the clinical course of illness alterations correlate with recovery (or lack of it), sug
progresses over time. However, distinguishing severe gesting targets for therapy and/or methods to identify
dehydration (for example, through diarrhoea and/or patients for clinical trials. Measuring a panel of urinary
vomiting) from situations in which the renal circulation markers (NGAL, matrix metalloproteinase protein 9
has been stopped and restarted (for example, in vascular (MMP9), IL‑18, hepatocyte growth factor (HGF) and
surgery or cardiac arrest) is not difficult in clinical prac cystatin C) at 14 days after onset of RRT-requiring AKI41
tice. Instead, a better understanding of likely outcomes is proved very predictive of renal recovery within 60 days
needed for the majority of clinical cases, in which multi from the start of RRT (area under the curve = 0.88–0.94
ple, but less severe, renal insults coexist. These cases are in a model that included clinical variables), although
poorly reflected by current animal models. no individual marker performed well in isolation,
Importantly and as mentioned earlier, profound which may indicate that differing phenotypes of recov
hypovolemic states are unlikely to arise in patients in ery from AKI were captured by the broader model.
modern ICUs, where volume overload is the prevailing When concentrations of TIMP2 and IGBP7 exceeded
clinical picture. Although it is true that extravascular 2.0 (ng/ml)2 × 1,000, the risk of death or dialysis at
volume may not reflect circulating blood volume, the 9 months was increased (HR 2.11, 95% CI 1.37–3.23),
development of AKI in the ICU is far more likely to be a which suggests a connection with both underlying renal
result of sepsis, nephrotoxins and/or major surgery than injury and its recovery as well as potential utility in tar
hypovolaemia. Disparities between physiological reduc geting patients for interventions aimed at long-term
tions in GFR and established tubular injury could be outcomes from AKI121.
revealed by novel AKI biomarkers. In an Ngal reporter
mouse, ischaemia–reperfusion, cisplatin and endotoxin Conclusions
insults induced renal NGAL expression, whereas volume The various common settings of AKI seem to involve
depletion that was sufficient to induce a 50% increase inflammatory, ischaemic and direct toxin-mediated
in serum creatinine level did not 113. In clinical practice, injury, which may induce rapidly reversible or persis
urinary detection of NGAL in 1,635 unselected patients tent renal dysfunction depending on the nature, con
predicted reversible versus nonrapidly reversible AKI text and severity of the injury. Furthermore, resolution
(with 81% specificity and 68% sensitivity at a thresh of dysfunction may not guarantee resolution of injury.
old of 104 ng/ml) at emergency room presentation114. Whereas these paradigms can be distinct in animal
228 | APRIL 2018 | VOLUME 14 www.nature.com/nrneph
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
models, they are often blurred in clinical practice. risks of death, cardiovascular disease and recurrent AKI
Furthermore, various AKI paradigms, although distinct in later years. Although we believe that some progress
from each other, seem to be heterogeneous at the sub has been made in terms of targeting individual AKI
clinical level, and multiple endophenotypes may exist syndromes, clinical phenotyping may not be sufficiently
within each paradigm. Although sepsis is the leading specific, and efforts are needed to develop classifications
cause of AKI, our understanding of the distinguish that can guide therapy — both at the bedside today and
ing features of its pathophysiology remains limited25. for the development of new therapies tomorrow.
Overall, despite some advances in biomarker develop Finally, a crucial need exists for longitudinal epi
ment, the scientific foundation for distinct phenotypes demiological studies and samples (blood, urine and tis
of clinical AKI is weak, and early tissue analysis of sue) that would enable the testing of multiple hypotheses
human AKI has not been carried out on a large scale. as to the nature of AKI and its pathophysiology and out
Our current understanding is that long-term outcomes comes. Only then can new interventions be developed
of AKI are linked to the development of CKD; however, — existing interventions have failed owing to our lack
this relationship is complex. Although recent evidence of understanding of the diverse underlying pathophysi
suggests that most deaths after ICU discharge occur ology of AKI as well as its common and contrasting
within 90 days42, even in patients who seem to recover features that are poorly encompassed within current
renal function, CKD may develop, conferring ongoing functional definitions of AKI.
1. Kellum, J. A., Bellomo, R. & Ronco, C. Kidney Attack. 20. Langenberg, C., Wan, L., Egi, M., May, C. N. & may improve the survival of transplant failure patients.
JAMA 307, 2265–2266 (2012). Bellomo, R. Renal blood flow in experimental septic J. Am. Soc. Nephrol. 18, 1331–1337 (2007).
2. Bedford, M., Stevens, P. E., Wheeler, T. W. K. & acute renal failure. Kidney Int. 69, 1996–2002 38. Sarnak, M. J., Sarnak, M. J., Jaber, B. L. & Jaber, B. L.
Farmer, C. K. T. What is the real impact of acute (2006). Mortality caused by sepsis in patients with end-stage
kidney injury? BMC Nephrol. 15, 95 (2014). 21. Di Giantomasso, D., May, C. N. & Bellomo, R. Vital renal disease compared with the general population.
3. United States Renal Data System. 2013 Annual Data organ blood flow during hyperdynamic sepsis. Chest Kidney Int. 58, 1758–1764 (2000).
Report Vol. 1 Ch. 6 (USRDS, 2013). 124, 1053–1059 (2003). 39. Vanholder, R. & Ringoir, S. Infectious morbidity and
4. Kane-Gill, S. L. et al. Risk factors for acute 22. Prowle, J. R. & Bellomo, R. Sepsis-associated acute defects of phagocytic function in end-stage renal
kidney injury in older adults with critical illness: kidney injury: macrohemodynamic and disease: a review. J. Am. Soc. Nephrol. 3, 1541–1554
a retrospective cohort study. Am. J. Kidney Dis. 65, microhemodynamic alterations in the renal circulation. (1993).
860–869 (2015). Semin. Nephrol. 35, 64–74 (2015). 40. Winters, B. D. et al. Long-term mortality and quality of
5. Murugan, R. et al. Acute kidney injury in non-severe 23. Maiden, M. J. et al. Structure and function of the life in sepsis: a systematic review. Crit. Care Med. 38,
pneumonia is associated with an increased immune kidney in septic shock. a prospective controlled 1276–1283 (2010).
response and lower survival. Kidney Int. 77, Exp. Study. Am. J. Respir. Crit. Care Med. 194, 41. Murugan, R. et al. Plasma inflammatory and apoptosis
527–535 (2010). 692–700 (2016). markers are associated with dialysis dependence and
6. Sileanu, F. E. et al. AKI in low-risk versus high-risk 24. Benes, J. et al. Searching for mechanisms that matter death among critically ill patients receiving renal
patients in intensive care. Clin. J. Am. Soc. Nephrol. in early septic acute kidney injury: an experimental replacement therapy. Nephrol. Dial. Transplant 29,
10, 187–196 (2015). study. Crit. Care 15, R256 (2011). 1854–1864 (2014).
7. Pickkers, P. et al. The intensive care medicine agenda 25. Gomez, H. et al. A unified theory of sepsis-induced 42. Kellum, J. A. et al. The effects of alternative
on acute kidney injury. Intensive Care Med. 8, acute kidney injury: inflammation, microcirculatory resuscitation strategies on acute kidney injury in
R204–R212 (2017). dysfunction, bioenergetics, and the tubular cell patients with septic shock. Am. J. Respir. Crit. Care
8. Barasch, J., Zager, R. & Bonventre, J. V. Acute kidney adaptation to injury. Shock, 41, 3–11 (2014). Med. 193, 281–287 (2016).
injury: a problem of definition. Lancet 389, 779–781 26. Verma, S. K. & Molitoris, B. A. Renal endothelial injury 43. Brunner, F. P., Thiel, G., Hermle, M., Bock, H. A. &
(2017). and microvascular dysfunction in acute kidney injury. Mihatsch, M. J. Long-term enalapril and verapamil
9. Uchino, S. et al. Acute renal failure in critically ill Semin. Nephrol. 35, 96–107 (2015). in rats with reduced renal mass. Kidney Int. 36,
patients: a multinational, multicenter study. JAMA 27. Post, E. H., Kellum, J. A., Bellomo, R. & Vincent, J.‑L. 969–977 (1989).
294, 813–818 (2005). Renal perfusion in sepsis: from macro- to 44. Ikoma, M., Kawamura, T., Kakinuma, Y., Fogo, A. &
10. Bagshaw, S. M. et al. A multi-centre evaluation of the microcirculation. Kidney Int. 91, 45–60 (2017). Ichikawa, I. Cause of variable therapeutic efficiency of
RIFLE criteria for early acute kidney injury in critically 28. Calzavacca, P., Evans, R. G., Bailey, M., Bellomo, R. & angiotensin converting enzyme inhibitor on glomerular
ill patients. Nephrol. Dial. Transplant 23, 1203–1210 May, C. N. Cortical and medullary tissue perfusion and lesions. Kidney Int. 40, 195–202 (1991).
(2007). oxygenation in experimental septic acute kidney injury. 45. Cheng, S.‑Y. et al. Losartan reduces ensuing chronic
11. Singbartl, K. & Kellum, J. A. AKI in the ICU: definition, Crit. Care Med. 43, e431–e439 (2015). kidney disease and mortality after acute kidney injury.
epidemiology, risk stratification, and outcomes. 29. Lankadeva, Y. R. et al. Intrarenal and urinary Sci. Rep. 6, 34265 (2016).
Kidney Int. 81, 819–825 (2012). oxygenation during norepinephrine resuscitation in 46. Carmichael, P. & Carmichael, A. R. Acute renal failure in
12. Angus, D. C. et al. Epidemiology of severe sepsis in ovine septic acute kidney injury. Kidney Int. 90, the surgical setting. ANZ J. Surg. 73, 144–153 (2003).
the United States: analysis of incidence, outcome, 100–108 (2016). 47. Shusterman, N. et al. Risk factors and outcome of
and associated costs of care. Crit. Care Med. 29, 30. Bezemer, R. et al. Real-time assessment of renal hospital-acquired acute renal failure. Clinical
1303–1310 (2001). cortical microvascular perfusion heterogeneities using epidemiologic study. Am. J. Med. 83, 65–71 (1987).
13. Bouchard, J. et al. A prospective international near-infrared laser speckle imaging. Opt. Express 18, 48. Weiser, T. G. et al. Estimate of the global volume of
multicenter study of AKI in the intensive care 15054–15061 (2010). surgery in 2012: an assessment supporting improved
unit. Clin. J. Am. Soc. Nephrol. 10, 1324–1331 31. Casellas, D. & Mimran, A. Aglomerular pathways in health outcomes. Lancet 385 (Suppl. 2), S11 (2015).
(2015). intrarenal microvasculature of aged rats. Am. J. Anat. 49. Weiser, T. G. et al. An estimation of the global volume
14. Vincent, J.‑L. et al. Sepsis in European intensive 156, 293–299 (1979). of surgery: a modelling strategy based on available
care units: results of the SOAP study. Crit. Care Med. 32. Dellepiane, S., Marengo, M. & Cantaluppi, V. data. Lancet 372, 139–144 (2008).
34, 344–353 (2006). Detrimental cross-talk between sepsis and acute kidney 50. Kork, F. et al. Minor postoperative increases of
15. Takasu, O. et al. Mechanisms of cardiac and renal injury: new pathogenic mechanisms, early biomarkers creatinine are associated with higher mortality and
dysfunction in patients dying of sepsis. Am. J. Respir. and targeted therapies. Crit. Care 20, 61 (2016). longer hospital length of stay in surgical patients.
Crit. Care Med. 187, 509–517 (2013). 33. Ghosh, C. C. et al. Gene control of tyrosine kinase TIE2 Anesthesiology 123, 1301–1311 (2015).
16. Langenberg, C., Gobe, G., Hood, S., May, C. N. & and vascular manifestations of infections. Proc. Natl 51. Korenkevych, D. et al. The pattern of longitudinal
Bellomo, R. Renal histopathology during Acad. Sci. USA 113, 2472–2477 (2016). change in serum creatinine and 90‑day mortality
experimental septic acute kidney injury and recovery. 34. Mariano, F. et al. Circulating plasma factors induce after major surgery. Ann. Surg. 263, 1219–1227
Crit. Care Med. 42, e58–e67 (2014). tubular and glomerular alterations in septic burns (2016).
17. De Backer, D., Creteur, J., Preiser, J.‑C., Dubois, M.‑J. patients. Crit. Care 12, R42 (2008). 52. Grams, M. E. et al. Acute kidney injury after major
& Vincent, J.‑L. Microvascular blood flow is altered in 35. Mehta, R. L. et al. Sepsis as a cause and consequence surgery: a retrospective analysis of veterans health
patients with sepsis. Am. J. Respir. Crit. Care Med. of acute kidney injury: program to improve care in administration data. Am. J. Kidney Dis. 67, 872–880
166, 98–104 (2002). acute renal disease. Intensive Care Med. 37, 241–248 (2016).
18. Spronk, P. E. et al. Nitroglycerin in septic shock after (2010). 53. Grams, M. E. et al. Candidate surrogate end points for
intravascular volume resuscitation. Lancet 360, 36. Singbartl, K. et al. Differential effects of kidney–lung ESRD after AKI. J. Am. Soc. Nephrol. 27, 2851–2859
1395–1396 (2002). cross-talk during acute kidney injury and bacterial (2016).
19. Donati, A. et al. The aPC treatment improves pneumonia. Kidney Int. 80, 633–644 (2011). 54. O’Connor, M. E. et al. Acute kidney injury and mortality
microcirculation in severe sepsis/septic shock 37. Johnston, O., Zalunardo, N., Rose, C. & Gill, J. S. 1 year after major non-cardiac surgery. Br. J. Surg.
syndrome. BMC Anesthesiol. 13, 25 (2013). Prevention of sepsis during the transition to dialysis 104, 868–876 (2017).
NATURE REVIEWS | NEPHROLOGY VOLUME 14 | APRIL 2018 | 229
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
55. O’Connor, M. E., Kirwan, C. J., Pearse, R. M. & 79. Leacche, M. et al. Outcomes in patients with normal 105. Kellum, J. A., Sileanu, F. E., Bihorac, A., Hoste, E. A. J.
Prowle, J. R. Incidence and associations of acute kidney serum creatinine and with artificial renal support for & Chawla, L. S. Recovery after acute kidney injury.
injury after major abdominal surgery. Intensive Care acute renal failure developing after coronary artery Am. J. Respir. Crit. Care Med. 195, 784–791 (2017).
Med. 42, 521–530 (2016). bypass grafting. Am. J. Cardiol. 93, 353–356 (2004). 106. Molitoris, B. A. et al. Design of clinical trials in AKI:
56. Thiele, R. H., Isbell, J. M. & Rosner, M. H. AKI 80. Thakar, C. V. et al. Predicting acute renal failure after a report from an NIDDK workshop. Trials of patients
associated with cardiac surgery. Clin. J. Am. Soc. cardiac surgery: validation and re‑definition of a risk- with sepsis selected hospital settings. Clin. J. Am. Soc.
Nephrol. 10, 500–514 (2015). stratification algorithm. Hemodial. Int. 7, 143–147 Nephrol. 7, 856–860 (2012).
57. Chertow, G. M. et al. Preoperative renal risk (2003). 107. Chawla, L. S., Eggers, P. W., Star, R. A. & Kimmel, P. L.
stratification. Circulation 95, 878–884 (1997). 81. Oliver, J., MacDowell, M. & Tracy, A. The pathogenesis Acute kidney injury and chronic kidney disease as
58. Prowle, J. R. et al. Preoperative renal dysfunction and of acute renal failure associated with traumatic and interconnected syndromes. N. Engl. J. Med. 371,
mortality after non-cardiac surgery. Br. J. Surg. 103, toxic injury; renal ischemia, nephrotoxic damage and 58–66 (2014).
1316–1325 (2016). the ischemic episode. J. Clin. Invest. 30, 1307–1439 108. Yuen, P. S. T., Jo, S.‑K., Holly, M. K., Hu, X. & Star, R. A.
59. Kheterpal, S. et al. Development and validation of an (1951). Ischemic and nephrotoxic acute renal failure are
acute kidney injury risk index for patients undergoing 82. Sandroni, C. et al. Acute kidney injury after cardiac distinguished by their broad transcriptomic responses.
general surgery: results from a national data set. arrest: a systematic review and meta-analysis of clinical Physiol. Genom. 25, 375–386 (2006).
Anesthesiology 110, 505–515 (2009). studies. Minerva Anestesiol. 82, 989–999 (2016). 109. Mar, D. et al. Heterogeneity of epigenetic changes at
60. Brienza, N., Giglio, M. T., Marucci, M. & Fiore, T. 83. Bonventre, J. V. & Yang, L. Cellular pathophysiology ischemia/reperfusion- and endotoxin-induced acute
Does perioperative hemodynamic optimization protect of ischemic acute kidney injury. J. Clin. Invest. 121, kidney injury genes. Kidney Int. 88, 734–744 (2015).
renal function in surgical patients? A meta-analytic 4210–4221 (2011). 110. Matejovic, M. et al. Molecular differences in
study. Crit. Care Med. 37, 2079–2090 (2009). 84. Sharfuddin, A. A. & Molitoris, B. A. Pathophysiology susceptibility of the kidney to sepsis-induced kidney
61. Prowle, J. R., Chua, H.‑R., Bagshaw, S. M. & of ischemic acute kidney injury. Nat. Rev. Nephrol. 7, injury. BMC Nephrol. 18, 183 (2017).
Bellomo, R. Clinical review: volume of fluid 189–200 (2011). 111. Fan, P.‑C., Chen, C.‑C., Chen, Y.‑C., Chang, Y.‑S. &
resuscitation and the incidence of acute kidney injury 85. Prowle, J. R., Ishikawa, K., May, C. N. & Bellomo, R. Chu, P.‑H. MicroRNAs in acute kidney injury.
— a systematic review. Crit. Care 16, 230 (2012). Renal blood flow during acute renal failure in man. Hum. Genom. 10, 29 (2016).
62. Sun, L. Y., Wijeysundera, D. N., Tait, G. A. & Blood Purif. 28, 216–225 (2009). 112. Xu, K. et al. Unique transcriptional programs identify
Beattie, W. S. Association of intraoperative 86. Mullens, W. et al. Importance of venous congestion subtypes of AKI. J. Am. Soc. Nephrol. 28, 1729–1740
hypotension with acute kidney injury after elective for worsening of renal function in advanced (2017).
noncardiac surgery. Anesthesiology 123, 515–523 decompensated heart failure. J. Am. Coll. Cardiol. 53, 113. Paragas, N. et al. The Ngal reporter mouse detects the
(2015). 589–596 (2009). response of the kidney to injury in real time. Nat. Med.
63. Walsh, M. et al. Relationship between intraoperative 87. Damman, K. et al. Increased central venous pressure is 17, 216–222 (2011).
mean arterial pressure and clinical outcomes after associated with impaired renal function and mortality 114. Nickolas, T. L. et al. Diagnostic and prognostic
noncardiac surgery: toward an empirical definition of in a broad spectrum of patients with cardiovascular stratification in the emergency department using
hypotension. Anesthesiology 119, 507–515 (2013). disease. J. Am. Coll. Cardiol. 53, 582–588 (2009). urinary biomarkers of nephron damage: a multicenter
64. Salmasi, V. et al. Relationship between intraoperative 88. Dalfino, L., Tullo, L., Donadio, I., Malcangi, V. & prospective cohort study. J. Am. Coll. Cardiol. 59,
hypotension, defined by either reduction from baseline Brienza, N. Intra-abdominal hypertension and acute 246–255 (2012).
or absolute thresholds, and acute kidney and renal failure in critically ill patients. Intensive Care 115. Haase, M., Kellum, J. A. & Ronco, C. Subclinical AKI —
myocardial injury after noncardiac surgery: Med. 34, 707–713 (2008). an emerging syndrome with important consequences.
a retrospective cohort analysis. Anesthesiology 126, 89. O’Connor, M. E. & Prowle, J. R. Fluid Overload. Nat. Rev. Nephrol. 8, 735–739 (2012).
47–65 (2017). Crit. Care Clin. 31, 803–821 (2015). 116. Borregaard, N. & Cowland, J. B. Granules of the
65. Saotome, T., Ishikawa, K., May, C. N., Birchall, I. E. & 90. Lauridsen, M. D. et al. Acute kidney injury treated with human neutrophilic polymorphonuclear leukocyte.
Bellomo, R. The impact of experimental hypoperfusion renal replacement therapy and 5‑year mortality after Blood 89, 3503–3521 (1997).
on subsequent kidney function. Intensive Care Med. myocardial infarction-related cardiogenic shock: 117. Kashani, K. et al. Discovery and validation of cell cycle
36, 533–540 (2010). a nationwide population-based cohort study. Crit. Care arrest biomarkers in human acute kidney injury.
66. Siegemund, M. et al. Aortic cross-clamping and 19, 452 (2015). Crit. Care 17, R25 (2013).
reperfusion in pigs reduces microvascular oxygenation 91. Taber, S. S. & Mueller, B. A. Drug-associated renal 118. Bihorac, A. et al. Validation of cell-cycle arrest
by altered systemic and regional blood flow dysfunction. Crit. Care Clin. 22, 357–374 (2006). biomarkers for acute. Am. J. Respir. Crit. Care Med.
distribution. Anesth. Analg. 111, 345–353 (2010). 92. Hou, S. H., Bushinsky, D. A., Wish, J. B., Cohen, J. J. & 189, 932–939 (2014).
67. Akira, S. & Takeda, K. Toll-like receptor signalling. Harrington, J. T. Hospital-acquired renal insufficiency: 119. Honore, P. M. et al. Urinary tissue inhibitor of
Nat. Rev. Immunol. 4, 499–511 (2004). a prospective study. Am. J. Med. 74, 243–248 (1983). metalloproteinase‑2 and insulin-like growth factor-
68. Cremer, J. et al. Systemic inflammatory response 93. Hui-Stickle, S., Brewer, E. D. & Goldstein, S. L. Pediatric binding protein 7 for risk stratification of acute kidney
syndrome after cardiac operations. Ann. Thorac. Surg. ARF epidemiology at a tertiary care center from 1999 injury in patients with sepsis. Crit. Care Med. 44,
61, 1714–1720 (1996). to 2001. Am. J. Kidney Dis. 45, 96–101 (2005). 1851–1860 (2016).
69. Rosner, M. H., Portilla, D. & Okusa, M. D. Cardiac 94. Liaño, F., Junco, E., Pascual, J., Madero, R. & Verde, E. 120. Murugan, R. & Kellum, J. A. Acute kidney injury:
surgery as a cause of acute kidney injury: pathogenesis The spectrum of acute renal failure in the intensive care what’s the prognosis? Nat. Rev. Nephrol. 7, 209–217
and potential therapies. J. Intensive Care Med. 23, unit compared with that seen in other settings. The (2011).
3–18 (2008). Madrid Acute Renal Fail. Study Group. Kidney Int. 121. Koyner, J. L. et al. Tissue inhibitor metalloproteinase‑2
70. Zhang, W. R. et al. Plasma IL‑6 and IL‑10 Suppl. 66, S16–S24 (1998). (TIMP‑2)⋅IGF-binding protein‑7 (IGFBP7) levels are
concentrations predict AKI and long-term mortality in 95. Nash, K., Hafeez, A. & Hou, S. Hospital-acquired renal associated with adverse long-term outcomes in
adults after cardiac surgery. J. Am. Soc. Nephrol. 26, insufficiency. Am. J. Kidney Dis. 39, 930–936 (2002). patients with AKI. J. Am. Soc. Nephrol. 26,
3123–3132 (2015). 96. Schetz, M., Dasta, J., Goldstein, S. & Golper, T. Drug- 1747–1754 (2015).
71. Andres-Hernando, A. et al. Cytokine production induced acute kidney injury. Curr. Opin. Crit. Care 11, 122. Bellomo, R. et al. Acute renal failure — definition,
increases and cytokine clearance decreases in mice 555–565 (2005). outcome measures, animal models, fluid therapy and
with bilateral nephrectomy. Nephrol. Dial. Transplant 97. Rosner, M. H. & Perazella, M. A. Acute Kidney Injury in information technology needs: the Second
27, 4339–4347 (2012). Patients with Cancer. N. Engl. J. Med. 376, 1770–1781 International Consensus Conference of the Acute
72. Lahiri, R. et al. Systemic inflammatory response (2017). Dialysis Quality Initiative (ADQI) Group. Crit. Care 8,
syndrome after major abdominal surgery predicted by 98. de Broe, M. E. & Porter, G. A. Clinical Nephrotoxins R204–R212 (2004).
early upregulation of TLR4 and TLR5. Ann. Surg. 263, (eds De Broe, M. E., Porter, G. A., Bennett, W. M. & 123. Kidney Disease: Improving Global Outcomes (KDIGO)
1028–1037 (2016). Deray, G.) (Springer, 2008). Acute Kidney Injury Work Group. KDIGO clinical
73. Hobson, C. E. et al. Acute kidney injury is associated 99. Ozkok, A. & Edelstein, C. L. Pathophysiology of practice guideline for acute kidney injury. Kidney Int.
with increased long-term mortality after cardiothoracic cisplatin-induced acute kidney injury. Biomed. Res. Int. Suppl. 2, 1–138 (2012).
surgery. Circulation 119, 2444–2453 (2009). 2014, 967826 (2014). 123. Kellum, J. A. et al. Classifying AKI by urine output
74. Bihorac, A. et al. National surgical quality 100. Faubel, S. et al. Cisplatin-induced acute renal failure is versus serum creatinine level. J. Am. Soc. Nephrol. 26,
improvement program underestimates the risk associated with an increase in the cytokines interleukin 2231–2238 (2015).
associated with mild and moderate postoperative (IL)-1beta, IL‑18, IL‑6, and neutrophil infiltration in the 124. Kaddourah, A., Basu, R. K., Bagshaw, S. M.,
acute kidney injury. Crit. Care Med. 41, 2570–2583 kidney. J. Pharmacol. Exp. Ther. 322, 8–15 (2007). Goldstein, S. L. & AWARE Investigators. Epidemiology
(2013). 101. Ramesh, G. & Reeves, W. B. TNF-alpha mediates of acute kidney injury in critically ill children and young
75. van Kuijk, J.‑P. et al. Temporary perioperative decline chemokine and cytokine expression and renal injury in adults. N. Engl. J. Med. 376, 11–20 (2017).
of renal function is an independent predictor for cisplatin nephrotoxicity. J. Clin. Invest. 110, 835–842
chronic kidney disease. Clin. J. Am. Soc. Nephrol. 5, (2002). Author contributions
1198–1204 (2010). 102. Sánchez-González, P. D., López-Hernández, F. J., J.A.K. and J.R.P. researched the data, discussed the article’s
76. Bihorac, A. et al. Incidence, clinical predictors, López-Novoa, J. M. & Morales, A. I. An integrative view content, wrote the text and reviewed or edited the article
genomics, and outcome of acute kidney injury among of the pathophysiological events leading to cisplatin before submission.
trauma patients. Ann. Surg. 252, 158–165 (2010). nephrotoxicity. Crit. Rev. Toxicol. 41, 803–821 (2011).
77. Bihorac, A. et al. Long-term risk of mortality and acute 103. Skinner, R. et al. Cisplatin dose rate as a risk factor Competing interests statement
kidney injury during hospitalization after major surgery. for nephrotoxicity in children. Br. J. Cancer 77, J.A.K. has received consulting fees and grant support from
Ann. Surg. 249, 851–858 (2009). 1677–1682 (1998). Astute Medical and Bioporto. J.R.P. declares no competing
78. Ishani, A. et al. The magnitude of acute serum 104. Menon, S., Kirkendall, E. S., Nguyen, H. & interests.
creatinine increase after cardiac surgery and the risk Goldstein, S. L. Acute kidney injury associated with
of chronic kidney disease, progression of kidney high nephrotoxic medication exposure leads to chronic Publisher’s note
disease, and death. Arch. Intern. Med. 171, 226–233 kidney disease after 6 months. J. Pediatr. 165, Springer Nature remains neutral with regard to jurisdictional
(2011). 522–527 (2014). claims in published maps and institutional affiliations.
230 | APRIL 2018 | VOLUME 14 www.nature.com/nrneph
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
Vous aimerez peut-être aussi
- Biochemical Correlates of Brain Structure and FunctionD'EverandBiochemical Correlates of Brain Structure and FunctionA.N. DavisonPas encore d'évaluation
- 10 1038@nrneph 2017 85 PDFDocument13 pages10 1038@nrneph 2017 85 PDFSirGonzPas encore d'évaluation
- CSA-AKI PatophysiologyDocument15 pagesCSA-AKI PatophysiologyOğuz KayıkçıPas encore d'évaluation
- Scleroderma Renal Crisis and Renal Involvement in Systemic SclerosisDocument14 pagesScleroderma Renal Crisis and Renal Involvement in Systemic Sclerosiszlaticab4246Pas encore d'évaluation
- Redefining Lupus Nephritis, Clinical Implications of Pathophysiologic Subtypes PDFDocument14 pagesRedefining Lupus Nephritis, Clinical Implications of Pathophysiologic Subtypes PDFaneliatiarasuciPas encore d'évaluation
- Tsokos 2016Document15 pagesTsokos 2016karen rinconPas encore d'évaluation
- Potpara2018 PDFDocument15 pagesPotpara2018 PDFNorlando RuizPas encore d'évaluation
- Dyslipidaemia in Nephrotic Syndrome: Mechanisms and TreatmentDocument14 pagesDyslipidaemia in Nephrotic Syndrome: Mechanisms and TreatmentEss liPas encore d'évaluation
- Giant Cell Arteritis and Polymyalgia Rheumatica: Current Challenges and OpportunitiesDocument15 pagesGiant Cell Arteritis and Polymyalgia Rheumatica: Current Challenges and OpportunitiesSue BarrPas encore d'évaluation
- A Systemic View of Alzheimer Disease 2017Document12 pagesA Systemic View of Alzheimer Disease 2017Jaime Arevalo PanduroPas encore d'évaluation
- Reviews: Obesity-Related Glomerulopathy: Clinical and Pathologic Characteristics and PathogenesisDocument19 pagesReviews: Obesity-Related Glomerulopathy: Clinical and Pathologic Characteristics and Pathogenesisthaynara robertoPas encore d'évaluation
- Cardiomiopatia Hipertrofica 2016 PDFDocument25 pagesCardiomiopatia Hipertrofica 2016 PDFBlanca Herrera MoralesPas encore d'évaluation
- Hormona Tiroidea y Sistema Cardiovascular - Nature 2017Document17 pagesHormona Tiroidea y Sistema Cardiovascular - Nature 2017Cristian MuñozPas encore d'évaluation
- Hormonas Tiroideas y Enfermedades Cardiovasculares Nature, 2016Document17 pagesHormonas Tiroideas y Enfermedades Cardiovasculares Nature, 2016Ruber Ballesteros LoraPas encore d'évaluation
- Reviews: Epidemiology, Diagnosis and Management of Hypertension Among Patients On Chronic DialysisDocument12 pagesReviews: Epidemiology, Diagnosis and Management of Hypertension Among Patients On Chronic DialysisConnie alvaPas encore d'évaluation
- Nrgastro 2017 38Document15 pagesNrgastro 2017 38Fasya DaffaPas encore d'évaluation
- Oligometastatic Prostate Cancer. Definitions, Clinical Outcomes, and Treatment Considerations (2017) .Document11 pagesOligometastatic Prostate Cancer. Definitions, Clinical Outcomes, and Treatment Considerations (2017) .Orlando SotoPas encore d'évaluation
- Membranosa 2Document17 pagesMembranosa 2Carolina CastroPas encore d'évaluation
- Diabetic Emergencies PDFDocument11 pagesDiabetic Emergencies PDFJuan C. Salazar PajaresPas encore d'évaluation
- Smolen2018 PDFDocument23 pagesSmolen2018 PDFJose Correa100% (1)
- Food KKDocument11 pagesFood KKNerissaArvianaShintaraPas encore d'évaluation
- Nrgastro 2017 1Document12 pagesNrgastro 2017 1Golam ZakariaPas encore d'évaluation
- AdrenolukodistropyDocument10 pagesAdrenolukodistropymary uwuPas encore d'évaluation
- Nontraumatic Intracerebral Haemorrhage in Young AdultsDocument14 pagesNontraumatic Intracerebral Haemorrhage in Young AdultsAmalia Gh,Pas encore d'évaluation
- MalariaDocument13 pagesMalariaAndres Felipe DuquePas encore d'évaluation
- Loeser PDFDocument9 pagesLoeser PDFGaudeamus IgiturPas encore d'évaluation
- Tahrani 2016Document27 pagesTahrani 2016Henry Leroy Lewis BatresPas encore d'évaluation
- Diabetic Emergencies - Ketoacidosis, Hyperglycaemic Hyperosmolar State and Hypoglycaemia, 2016, NatureDocument11 pagesDiabetic Emergencies - Ketoacidosis, Hyperglycaemic Hyperosmolar State and Hypoglycaemia, 2016, Naturexoxiv41110Pas encore d'évaluation
- Manifestaciones Neurologicas VIH NatureDocument13 pagesManifestaciones Neurologicas VIH NatureGeral D. VelascoPas encore d'évaluation
- Potential New Therapy For OphthalmopathyDocument1 pagePotential New Therapy For OphthalmopathyEsteban Martin Chiotti KaneshimaPas encore d'évaluation
- Nrneurol 2016 107Document12 pagesNrneurol 2016 107Eduard Antonio Maury SintjagoPas encore d'évaluation
- 12 - The Genetics of Myelodysplastic Syndrome - From Clonal Haematopoiesis To Secondary LeukaemiaDocument15 pages12 - The Genetics of Myelodysplastic Syndrome - From Clonal Haematopoiesis To Secondary LeukaemiaJosuéPas encore d'évaluation
- Barturen 2018Document20 pagesBarturen 2018jezy2014Pas encore d'évaluation
- Escobar Mor Real e 2018Document15 pagesEscobar Mor Real e 2018HIDAYATUL RAHMIPas encore d'évaluation
- Nature - Antithrombotic Therapy For PatientsDocument19 pagesNature - Antithrombotic Therapy For PatientsMatheus Augusto Salerno Miguel e SousaPas encore d'évaluation
- Alzheimer e Diabetes Nature 2018Document14 pagesAlzheimer e Diabetes Nature 2018Viviane MacedoPas encore d'évaluation
- Panes Rimola 2017Document13 pagesPanes Rimola 2017Natasya DarrelPas encore d'évaluation
- Nrclinonc 2017 95Document13 pagesNrclinonc 2017 95김현수Pas encore d'évaluation
- Engineering and Physical Sciences in Oncology - Challenges and OpportunitiesDocument17 pagesEngineering and Physical Sciences in Oncology - Challenges and OpportunitiesAlessandroPas encore d'évaluation
- ES GastrointestinalDocument12 pagesES GastrointestinalMateus ValentePas encore d'évaluation
- Brain insulin resistance in type 2Document14 pagesBrain insulin resistance in type 2costarlrafaelaPas encore d'évaluation
- Wiles 2018Document20 pagesWiles 2018Andreas NatanPas encore d'évaluation
- ANTYPHOSPHODocument20 pagesANTYPHOSPHOLuis David Beltran OntiverosPas encore d'évaluation
- Ya EstasDocument19 pagesYa EstasMedranoReyesLuisinPas encore d'évaluation
- SAFDocument19 pagesSAFnowimsunheePas encore d'évaluation
- Synovial Tissue Research State of The Art ReviewDocument13 pagesSynovial Tissue Research State of The Art ReviewDeliana Nur Ihsani RahmiPas encore d'évaluation
- 2017 Nature Adult-Onset Autoimmune DiabetesDocument13 pages2017 Nature Adult-Onset Autoimmune Diabetesguanyulin01Pas encore d'évaluation
- Nrneurol 2018 30 PDFDocument16 pagesNrneurol 2018 30 PDFFathan MustafidPas encore d'évaluation
- Living KidneyDocument9 pagesLiving KidneyEss liPas encore d'évaluation
- Yazici Et Al - 2018 - Behçet SyndromeDocument13 pagesYazici Et Al - 2018 - Behçet SyndromeantonioivPas encore d'évaluation
- Modelling Diabetic Nephropathy in MiceDocument9 pagesModelling Diabetic Nephropathy in MiceKarina ThiemePas encore d'évaluation
- Renal CellDocument10 pagesRenal CellEss liPas encore d'évaluation
- Hipertensión Arterial NRPDocument21 pagesHipertensión Arterial NRPEnrique UrraPas encore d'évaluation
- HongosDocument21 pagesHongosCristian ChávezPas encore d'évaluation
- Pancreatitis 2Document8 pagesPancreatitis 2Romina GonzálezPas encore d'évaluation
- Otto 2017Document23 pagesOtto 2017yankusumaPas encore d'évaluation
- Primer: Chronic PancreatitisDocument18 pagesPrimer: Chronic PancreatitisFrancisco FigueiredoPas encore d'évaluation
- Grupo 6 - Pancreatitis Crónica (01-15)Document15 pagesGrupo 6 - Pancreatitis Crónica (01-15)Romina GonzálezPas encore d'évaluation
- Reviews: A Clinicopathological Approach To The Diagnosis of DementiaDocument16 pagesReviews: A Clinicopathological Approach To The Diagnosis of DementiaLeonardo Barrera ArizaPas encore d'évaluation
- Alhmeimer 23445Document15 pagesAlhmeimer 23445safia osmanPas encore d'évaluation
- Nephrotic Syndrome: Components, Connections, and Angiopoietin-Like 4 - Related TherapeuticsDocument6 pagesNephrotic Syndrome: Components, Connections, and Angiopoietin-Like 4 - Related TherapeuticsDiego Kaleth BastidasPas encore d'évaluation
- Pi Is 0272638623005917Document55 pagesPi Is 0272638623005917hemer hadyn calderon alvitesPas encore d'évaluation
- Short-Term Effects of Very-Low-Phosphate andDocument9 pagesShort-Term Effects of Very-Low-Phosphate andhemer hadyn calderon alvitesPas encore d'évaluation
- Article: A Secondary Analysis From A Controlled Diet Balance StudyDocument11 pagesArticle: A Secondary Analysis From A Controlled Diet Balance Studyhemer hadyn calderon alvitesPas encore d'évaluation
- Biomarcadores en AKIDocument14 pagesBiomarcadores en AKIhemer hadyn calderon alvitesPas encore d'évaluation
- Calcifilaxis PDFDocument11 pagesCalcifilaxis PDFhemer hadyn calderon alvitesPas encore d'évaluation
- Nutrition in Kidney Disease Core 2022Document13 pagesNutrition in Kidney Disease Core 2022hemer hadyn calderon alvitesPas encore d'évaluation
- Vitamin D Therapy in Adults With CKD A Systemati 230628 105811Document36 pagesVitamin D Therapy in Adults With CKD A Systemati 230628 105811hemer hadyn calderon alvitesPas encore d'évaluation
- KDIGO CKD-MBD Guideline Summary: Changes and RecommendationsDocument11 pagesKDIGO CKD-MBD Guideline Summary: Changes and Recommendationshemer hadyn calderon alvitesPas encore d'évaluation
- NefroDocument7 pagesNefrohemer hadyn calderon alvitesPas encore d'évaluation
- Kidney Support in Children Using An UltrafiltrationDocument9 pagesKidney Support in Children Using An Ultrafiltrationhemer hadyn calderon alvitesPas encore d'évaluation
- Short-Term Effects of Very-Low-Phosphate andDocument9 pagesShort-Term Effects of Very-Low-Phosphate andhemer hadyn calderon alvitesPas encore d'évaluation
- Guideline ADA 2010 in Hyperglicemia CrisisDocument9 pagesGuideline ADA 2010 in Hyperglicemia CrisisAissyiyah Nur An NisaPas encore d'évaluation
- Diagnostic Use of Base Excess in Acid-BaseDocument10 pagesDiagnostic Use of Base Excess in Acid-Basejcarl_20063003Pas encore d'évaluation
- Hypertension Management in Transition From CKD A ERDS 2016Document7 pagesHypertension Management in Transition From CKD A ERDS 2016hemer hadyn calderon alvitesPas encore d'évaluation
- Management of Patients at Risk of Acute Kidney Injury 2017 PDFDocument13 pagesManagement of Patients at Risk of Acute Kidney Injury 2017 PDFhemer hadyn calderon alvitesPas encore d'évaluation
- Hyperkalemia and Hypokalemia in CKD: Prevalence, Risk Factors, and Clinical OutcomesDocument4 pagesHyperkalemia and Hypokalemia in CKD: Prevalence, Risk Factors, and Clinical Outcomeshemer hadyn calderon alvitesPas encore d'évaluation
- Management of The Metabolic Acidosis of Chronic Kidney DiseaseDocument7 pagesManagement of The Metabolic Acidosis of Chronic Kidney Diseasehemer hadyn calderon alvitesPas encore d'évaluation
- 10 1056@NEJMra1700312Document12 pages10 1056@NEJMra1700312Victor CarrenoPas encore d'évaluation
- Antimicrobial Resistance in Nephrology 2019 PDFDocument19 pagesAntimicrobial Resistance in Nephrology 2019 PDFhemer hadyn calderon alvitesPas encore d'évaluation
- Pi Is 1548559519301144Document20 pagesPi Is 1548559519301144hemer hadyn calderon alvites0% (1)
- Poliquistosis RenalDocument10 pagesPoliquistosis Renalhemer hadyn calderon alvitesPas encore d'évaluation
- IgA Nephropathy in Elderly PatientsDocument10 pagesIgA Nephropathy in Elderly Patientshemer hadyn calderon alvitesPas encore d'évaluation
- Renal Perfusion During Hemodialysis: Intradialytic Blood Flow Decline and Effects of Dialysate CoolingDocument10 pagesRenal Perfusion During Hemodialysis: Intradialytic Blood Flow Decline and Effects of Dialysate Coolinghemer hadyn calderon alvitesPas encore d'évaluation
- Efficacy and Safety of MMF Patients With IgA Nephropathy An Update Meta AnalysisDocument10 pagesEfficacy and Safety of MMF Patients With IgA Nephropathy An Update Meta Analysishemer hadyn calderon alvitesPas encore d'évaluation
- Mechanisms, Clinical Implications, and Treatment of Intradialytic HypotensionDocument7 pagesMechanisms, Clinical Implications, and Treatment of Intradialytic Hypotensionhemer hadyn calderon alvitesPas encore d'évaluation
- 10.2215@Cjn.13191118 Aki y PancreatitisDocument10 pages10.2215@Cjn.13191118 Aki y Pancreatitishemer hadyn calderon alvitesPas encore d'évaluation
- Rituximab Vs Ciclosporina en GMN MenbranosaDocument11 pagesRituximab Vs Ciclosporina en GMN Menbranosahemer hadyn calderon alvitesPas encore d'évaluation
- Antimicrobial Resistance in Nephrology 2019Document19 pagesAntimicrobial Resistance in Nephrology 2019hemer hadyn calderon alvitesPas encore d'évaluation
- The History of Cells and Cell TheoryDocument12 pagesThe History of Cells and Cell TheoryReyna Pearl PalisboPas encore d'évaluation
- PLOTKINDocument6 pagesPLOTKINElPaisUyPas encore d'évaluation
- Exercise 8-Life ScienceDocument2 pagesExercise 8-Life ScienceKarinaPas encore d'évaluation
- Impact of Plant Breeding On The Genetic Diversity of Cultivated Strawberry As Revealed by Expressed Sequence Tag-Derived Simple Sequence Repeat MarkersDocument12 pagesImpact of Plant Breeding On The Genetic Diversity of Cultivated Strawberry As Revealed by Expressed Sequence Tag-Derived Simple Sequence Repeat MarkersJuan Diego DuquePas encore d'évaluation
- OsmosisDocument11 pagesOsmosisIscariot PriestPas encore d'évaluation
- Book Review: FOOD WARS: THE GLOBAL BATTLE FOR MOUTHS, MINDS AND MARKETS BY TIM LANG AND MICHAEL HEASMAN. PUBLISHED IN 2004 BY EARTHSCAN, LONDON. ISBN 1 - 85383-702-4 (PAPERBACK), 365 PAGESDocument3 pagesBook Review: FOOD WARS: THE GLOBAL BATTLE FOR MOUTHS, MINDS AND MARKETS BY TIM LANG AND MICHAEL HEASMAN. PUBLISHED IN 2004 BY EARTHSCAN, LONDON. ISBN 1 - 85383-702-4 (PAPERBACK), 365 PAGESRandyPas encore d'évaluation
- READ How A Common Soup ThickenerDocument4 pagesREAD How A Common Soup ThickenerOgooNkem100% (1)
- Life Science Evidence 1Document5 pagesLife Science Evidence 1Cintia Mtz0% (1)
- Etextbook 978 0078096945 Essentials of The Living World 5th EditionDocument61 pagesEtextbook 978 0078096945 Essentials of The Living World 5th Editionmark.dame383100% (44)
- FungicidesDocument548 pagesFungicideshalmasti73730% (1)
- Daily Lesson Log Grade 10Document4 pagesDaily Lesson Log Grade 10Ezekiel LapitanPas encore d'évaluation
- Lecture Note Plant Structure and FunctionDocument22 pagesLecture Note Plant Structure and FunctionMilka Rahman100% (1)
- Anthropology Lab Report 1Document5 pagesAnthropology Lab Report 1api-285362626Pas encore d'évaluation
- Byjus Com Biology Plant PhysiologyDocument14 pagesByjus Com Biology Plant PhysiologyVikas PratikPas encore d'évaluation
- Science 10-Pretest Third QuarterDocument4 pagesScience 10-Pretest Third QuarterCristian PortugalPas encore d'évaluation
- COVID-19 mRNA Vaccine BNT162b2 UKPAR PFIZER BIONTECH 15dec2020Document51 pagesCOVID-19 mRNA Vaccine BNT162b2 UKPAR PFIZER BIONTECH 15dec2020gio malicoPas encore d'évaluation
- Evolution of Social BehaviorDocument48 pagesEvolution of Social BehaviorNaniPas encore d'évaluation
- Distinguish Between Energy Flow and Nutrient Cycling Within An EcosystemDocument3 pagesDistinguish Between Energy Flow and Nutrient Cycling Within An EcosystemPrince RichardsPas encore d'évaluation
- 10 Cambridge Grade 8 Biology Exam Style Questions and AnswersDocument2 pages10 Cambridge Grade 8 Biology Exam Style Questions and AnswersqhlwjuvrvqygwglzegPas encore d'évaluation
- Biosynthetic Studies & Basic Metabolic Pathways: Prepared by Pooja H. Khanpara Asst. Professor Apip, JamnagarDocument89 pagesBiosynthetic Studies & Basic Metabolic Pathways: Prepared by Pooja H. Khanpara Asst. Professor Apip, Jamnagaranurag srivastavaPas encore d'évaluation
- Lesson Plan Cycle of InfectionDocument7 pagesLesson Plan Cycle of InfectionJeanette Bonifacio CorpuzPas encore d'évaluation
- PDFDocument198 pagesPDFDanica BalanayPas encore d'évaluation
- Human Biological DiversityDocument5 pagesHuman Biological DiversityJoyce Sarmiento100% (1)
- Functional Anatomy of Prokaryotic CellsDocument28 pagesFunctional Anatomy of Prokaryotic CellsGabz GabbyPas encore d'évaluation
- Physical Properties of Sugarcane for Harvester DesignDocument6 pagesPhysical Properties of Sugarcane for Harvester DesignKen MaglintePas encore d'évaluation
- Immunology - Must To KnowDocument3 pagesImmunology - Must To KnowSakthi VelPas encore d'évaluation
- Grade 12 Biology Model QuestionsDocument9 pagesGrade 12 Biology Model Questionsmmree yyttPas encore d'évaluation
- ImunosenecenceDocument272 pagesImunosenecenceLorenzzo StringariPas encore d'évaluation
- Lbybio4 Cell DivisionDocument2 pagesLbybio4 Cell DivisionAlyssaPas encore d'évaluation
- Cell Cycle StagesDocument6 pagesCell Cycle StagesCathy MoronioPas encore d'évaluation