Vous aimerez peut-être aussi
- Smith Slides CH 4Document26 pagesSmith Slides CH 4USHA RANI SONOWALPas encore d'évaluation
- A Quick Guide To Project DPro (PMD Pro) Second Edition PDFDocument32 pagesA Quick Guide To Project DPro (PMD Pro) Second Edition PDFMarcos Romairone100% (1)
- Physiotherapy As An Initial Treatment Option For Femoroacetabular ImpingementDocument9 pagesPhysiotherapy As An Initial Treatment Option For Femoroacetabular ImpingementNicolas ParejaPas encore d'évaluation
- Ankle Stabilization With Arthroscopic Versus Open With Suture Tape Augmentation Techniques X1D XJ. George DeVries PDFDocument5 pagesAnkle Stabilization With Arthroscopic Versus Open With Suture Tape Augmentation Techniques X1D XJ. George DeVries PDFcrpcsxfdkgPas encore d'évaluation
- Clinical Outcomes of Rehabilitation For Patients Following Lateral Patellar Dislocation: A Systematic ReviewDocument13 pagesClinical Outcomes of Rehabilitation For Patients Following Lateral Patellar Dislocation: A Systematic ReviewHarshoi KrishannaPas encore d'évaluation
- Comparative Study of Posterior Stabilizing VS Cruciate Retaining Prosthesis in Total Knee ReplacementDocument15 pagesComparative Study of Posterior Stabilizing VS Cruciate Retaining Prosthesis in Total Knee ReplacementIJAR JOURNALPas encore d'évaluation
- Full Length Research Article: ISSN: 2230-9926Document4 pagesFull Length Research Article: ISSN: 2230-9926Anonymous mnN7WfCoPas encore d'évaluation
- Is The Prognosis of Osgood-Schlatter Poorer Than Anticipated?Document9 pagesIs The Prognosis of Osgood-Schlatter Poorer Than Anticipated?gastón giosciaPas encore d'évaluation
- Does Total Knee Replacement Restore NormDocument9 pagesDoes Total Knee Replacement Restore NormSahithya MPas encore d'évaluation
- Approach Sports Health: A MultidisciplinaryDocument8 pagesApproach Sports Health: A MultidisciplinaryLorena WinklerPas encore d'évaluation
- DiGiovanni 2003 PDFDocument8 pagesDiGiovanni 2003 PDFPhooi Yee LauPas encore d'évaluation
- Schuster Case Report2 Draft 4 - Brief For PortfolioDocument47 pagesSchuster Case Report2 Draft 4 - Brief For Portfolioapi-528037163Pas encore d'évaluation
- Evidence-Based Treatment Choices For Acute Lateral Ankle Sprain: A Comprehensive Systematic ReviewDocument9 pagesEvidence-Based Treatment Choices For Acute Lateral Ankle Sprain: A Comprehensive Systematic ReviewMilton RezzaPas encore d'évaluation
- The Hip Joint Arthroscopic Procedures AnDocument11 pagesThe Hip Joint Arthroscopic Procedures AnwladjaPas encore d'évaluation
- PTH 790-Case ReportDocument10 pagesPTH 790-Case Reportapi-551496110Pas encore d'évaluation
- WeasDocument9 pagesWeasJorge Alejandro Soto LevicoyPas encore d'évaluation
- 10 - Long-Term Outcome of Planovalgus Foot Surgical Correction in Children With Cerebral PalsyDocument7 pages10 - Long-Term Outcome of Planovalgus Foot Surgical Correction in Children With Cerebral PalsyJoe MehannaPas encore d'évaluation
- Low-Level Laser Therapy at 635 NM For Treatment of Chronic Plantar Fasciitis. A Placebo-Controlled, Randomized StudyDocument5 pagesLow-Level Laser Therapy at 635 NM For Treatment of Chronic Plantar Fasciitis. A Placebo-Controlled, Randomized StudymarioPas encore d'évaluation
- Manual Therapy For Plantar Heel PainDocument6 pagesManual Therapy For Plantar Heel PainMarychell SantiagoPas encore d'évaluation
- Activity Modification and Knee Strengthening For Osgood-Schlatter DiseaseDocument9 pagesActivity Modification and Knee Strengthening For Osgood-Schlatter DiseaseSebastian FandiñoPas encore d'évaluation
- Physical Therapy in The Postoperative of Proximal Femur Fracture in Elderly. Literature ReviewDocument4 pagesPhysical Therapy in The Postoperative of Proximal Femur Fracture in Elderly. Literature ReviewEcsekiel MirandaPas encore d'évaluation
- 45 Llps Vs HlbsDocument4 pages45 Llps Vs HlbsSudhir MishraPas encore d'évaluation
- 1 s2.0 S0003999319303892 MainDocument8 pages1 s2.0 S0003999319303892 MainRizkyrafiqoh afdinPas encore d'évaluation
- Research Article: Gait Patterns in Hemiplegic Patients With Equinus Foot DeformityDocument8 pagesResearch Article: Gait Patterns in Hemiplegic Patients With Equinus Foot DeformityCamila VargasPas encore d'évaluation
- Colgan 2016Document6 pagesColgan 2016Wahyu InsanPas encore d'évaluation
- Plantar FasciitisDocument23 pagesPlantar FasciitisMoses PaulPas encore d'évaluation
- 1 s2.0 S0929664619300567 MainDocument8 pages1 s2.0 S0929664619300567 Mainananta restyPas encore d'évaluation
- Physiotherapy After Tibial Plateau Fracture Fixation A Systematic Review of The Literature - PMCDocument1 pagePhysiotherapy After Tibial Plateau Fracture Fixation A Systematic Review of The Literature - PMCmf6wj6ccxqPas encore d'évaluation
- SiaiDocument8 pagesSiaimassimo bertoniPas encore d'évaluation
- Abstracts / Manual Therapy 25 (2016) E57 Ee169 E132Document2 pagesAbstracts / Manual Therapy 25 (2016) E57 Ee169 E132NICOLÁS ANDRÉS AYELEF PARRAGUEZPas encore d'évaluation
- Capstone 1 Final PaperDocument31 pagesCapstone 1 Final Paperapi-413271136Pas encore d'évaluation
- Outcomes of Hip Arthroscopy in Patients Aged 50 Years or Older Compared With A Matched-Pair Control of Patients Aged 30 Years or YoungerDocument8 pagesOutcomes of Hip Arthroscopy in Patients Aged 50 Years or Older Compared With A Matched-Pair Control of Patients Aged 30 Years or Youngersuad5stambuliePas encore d'évaluation
- Physical Examination Tests For Hip Dysfunction and Injury: March 2015Document8 pagesPhysical Examination Tests For Hip Dysfunction and Injury: March 2015wladjaPas encore d'évaluation
- Integrated Review WeeblyDocument10 pagesIntegrated Review Weeblyapi-401390929Pas encore d'évaluation
- Quiroprática e Osteopatia 2Document19 pagesQuiroprática e Osteopatia 2Pedro FonsecaPas encore d'évaluation
- v062p01162 PDFDocument6 pagesv062p01162 PDFPilar Riquelme AguilarPas encore d'évaluation
- A Pragmatic Regional Interdependence Approach To Primary Frozen Shoulder: A Retrospective Case SeriesDocument2 pagesA Pragmatic Regional Interdependence Approach To Primary Frozen Shoulder: A Retrospective Case SeriesVizaPas encore d'évaluation
- A Comprehensive Exercise Program Improves Foot Alignment in People With Flexible Flat Foot: A Randomised TrialDocument5 pagesA Comprehensive Exercise Program Improves Foot Alignment in People With Flexible Flat Foot: A Randomised Trial黃子庭Pas encore d'évaluation
- Tangtiphaiboontana 2021Document8 pagesTangtiphaiboontana 2021翁嘉聰Pas encore d'évaluation
- FinalDocument44 pagesFinalapi-512383088Pas encore d'évaluation
- Annals of Internal Medicine: Effectiveness of Manual Physical Therapy and Exercise in Osteoarthritis of The KneeDocument9 pagesAnnals of Internal Medicine: Effectiveness of Manual Physical Therapy and Exercise in Osteoarthritis of The KneeKhadija AkhundPas encore d'évaluation
- Mulligan Knee TapingDocument8 pagesMulligan Knee TapingVinicius MascarenhasPas encore d'évaluation
- Deepti - 2016 Effects of Retrowalking On Osteoarthritis of Knee in GeriatricDocument7 pagesDeepti - 2016 Effects of Retrowalking On Osteoarthritis of Knee in Geriatricnur pratiwiPas encore d'évaluation
- Intervenções Terapêuticas para Aumentar A Dorsiflexão Do Tornozelo Após Entorse Do TornozeloDocument14 pagesIntervenções Terapêuticas para Aumentar A Dorsiflexão Do Tornozelo Após Entorse Do TornozeloThiago Penna ChavesPas encore d'évaluation
- Tendinopatia RotulianaDocument12 pagesTendinopatia RotulianaPablo GFPas encore d'évaluation
- Foot Orthoses For Adults With Flexible Pes Planus: A Systematic ReviewDocument18 pagesFoot Orthoses For Adults With Flexible Pes Planus: A Systematic ReviewDonna KrawczykPas encore d'évaluation
- KT Revisão Sistemática, JOP 2014Document10 pagesKT Revisão Sistemática, JOP 2014Ju ChangPas encore d'évaluation
- New Synopsis FormatDocument8 pagesNew Synopsis FormatUpadhayayAnkurPas encore d'évaluation
- Heel Pain Plantar Fascitis Hard Vs Sorft Orthotics and Heels PadDocument11 pagesHeel Pain Plantar Fascitis Hard Vs Sorft Orthotics and Heels PadDik 40Pas encore d'évaluation
- Assessment of The Lequesne Index of Severity For Osteoarthritis of The Hip in An Elderly PopulationDocument7 pagesAssessment of The Lequesne Index of Severity For Osteoarthritis of The Hip in An Elderly PopulationKanliajie Kresna KastiantoPas encore d'évaluation
- ChiroandosteoDocument6 pagesChiroandosteoapi-3701230Pas encore d'évaluation
- Comparison Between Outcomes of Dry Needling With Conventional Protocol and Rood's Approach With Conventional Protocol On Pain, Strength and Balance in Knee OsteoarthritisDocument29 pagesComparison Between Outcomes of Dry Needling With Conventional Protocol and Rood's Approach With Conventional Protocol On Pain, Strength and Balance in Knee OsteoarthritisDrPratibha SinghPas encore d'évaluation
- JRRD 2014 05 0132Document12 pagesJRRD 2014 05 0132Jivanjot S. KohliPas encore d'évaluation
- Esska Knee Munich Doc 18Document16 pagesEsska Knee Munich Doc 18Avram GeorgievPas encore d'évaluation
- Riginal Research: LucasDocument11 pagesRiginal Research: Lucas'fanny Quenhita'Pas encore d'évaluation
- Current Evidence Does Not Support The Use of Kinesio Taping in Clinical Practice - A Systematic ReviewDocument9 pagesCurrent Evidence Does Not Support The Use of Kinesio Taping in Clinical Practice - A Systematic Reviewhrvoje09Pas encore d'évaluation
- A Clinical Test of Lumbopelvic ControlDocument7 pagesA Clinical Test of Lumbopelvic ControlFlávio GuimarãesPas encore d'évaluation
- O Fortalecimento Combinado Do Abdutor Do Quadril e Do Rotador Externo e o Alongamento Do Rotador Interno Do Quadril Melhoram A Dor e A Função em Pacientes Com Síndrome Da Dor Femoropatelar Um EnsaiDocument6 pagesO Fortalecimento Combinado Do Abdutor Do Quadril e Do Rotador Externo e o Alongamento Do Rotador Interno Do Quadril Melhoram A Dor e A Função em Pacientes Com Síndrome Da Dor Femoropatelar Um EnsaiLeticia ZaniniiPas encore d'évaluation
- Predictors of Chronic Ankle InstabilityDocument6 pagesPredictors of Chronic Ankle InstabilityLeydi LondoñoPas encore d'évaluation
- The Effectiveness of Proprioceptive Balance Board Training Program: An Intervention Mechanism in The Reduction of Ankle SprainDocument8 pagesThe Effectiveness of Proprioceptive Balance Board Training Program: An Intervention Mechanism in The Reduction of Ankle SprainchikitaPas encore d'évaluation
- Giray 2019Document13 pagesGiray 2019Felix LoaizaPas encore d'évaluation
- Sports Hernia and Athletic Pubalgia: Diagnosis and TreatmentD'EverandSports Hernia and Athletic Pubalgia: Diagnosis and TreatmentDavid R. DiduchPas encore d'évaluation
- Week Beginning Monday January 1, 2018: Monday Tuesday Wednesday Thursday Friday Saturday SundayDocument3 pagesWeek Beginning Monday January 1, 2018: Monday Tuesday Wednesday Thursday Friday Saturday SundayMae DoctoleroPas encore d'évaluation
- Anti InfectiveDocument9 pagesAnti InfectiveMae DoctoleroPas encore d'évaluation
- CPM17th RabiesDocument15 pagesCPM17th RabiesMae DoctoleroPas encore d'évaluation
- Tagalog Foot Care PDFDocument1 pageTagalog Foot Care PDFMae DoctoleroPas encore d'évaluation
- Effects of Bracing in Adult With Scoliosis: A Retrospective StudyDocument4 pagesEffects of Bracing in Adult With Scoliosis: A Retrospective StudyMae DoctoleroPas encore d'évaluation
- Medical FormDocument7 pagesMedical FormMae DoctoleroPas encore d'évaluation
- Disease of The Biliary TractDocument7 pagesDisease of The Biliary TractMae DoctoleroPas encore d'évaluation
- Why Do We Need To Adopt The I.M.C.I. Approach or The Integrated Management of Childhood Illness in The Philippines ?Document15 pagesWhy Do We Need To Adopt The I.M.C.I. Approach or The Integrated Management of Childhood Illness in The Philippines ?Mae DoctoleroPas encore d'évaluation
- Why Do We Need To Adopt The I.M.C.I. Approach or The Integrated Management of Childhood Illness in The Philippines ?Document15 pagesWhy Do We Need To Adopt The I.M.C.I. Approach or The Integrated Management of Childhood Illness in The Philippines ?Mae DoctoleroPas encore d'évaluation
- HEENTDocument2 pagesHEENTMae DoctoleroPas encore d'évaluation
- Sedative Hypnotics PDFDocument8 pagesSedative Hypnotics PDFMae DoctoleroPas encore d'évaluation
- Respondents or The Target Population of The Study Will Be Discussed and ExplainedDocument5 pagesRespondents or The Target Population of The Study Will Be Discussed and ExplainedKatherine MacasilhigPas encore d'évaluation
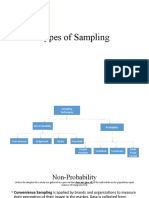
- Types of SamplingDocument13 pagesTypes of SamplingCAELUM ONLINEPas encore d'évaluation
- Customer Satisfaction AirtelDocument62 pagesCustomer Satisfaction AirtelBhavi GolchhaPas encore d'évaluation
- Principles, Values and Regulation in The Health and Social Care SectorDocument15 pagesPrinciples, Values and Regulation in The Health and Social Care SectorAkinrinade SamuelPas encore d'évaluation
- Deflectionproblems in ACI-318Document42 pagesDeflectionproblems in ACI-318imzee25Pas encore d'évaluation
- Capacity Enhancement On Research Conduct..Document39 pagesCapacity Enhancement On Research Conduct..robertPas encore d'évaluation
- Learning Activity Sheet in Entrepreneurship: Hinunangan National High SchoolDocument8 pagesLearning Activity Sheet in Entrepreneurship: Hinunangan National High SchoolMarife CulabaPas encore d'évaluation
- Assessment in The Language ClassroomDocument17 pagesAssessment in The Language ClassroomHamda NasrPas encore d'évaluation
- Rintamaki, Et Al., (2006)Document19 pagesRintamaki, Et Al., (2006)Linda PertiwiPas encore d'évaluation
- Reviewing For The Final Exam STAT 1350Document4 pagesReviewing For The Final Exam STAT 1350mattPas encore d'évaluation
- Conflicts and Multicultural Team: Developing Competencies For ManagersDocument54 pagesConflicts and Multicultural Team: Developing Competencies For ManagersUlysses GamayonPas encore d'évaluation
- The Implementation and Evaluation of OASIS: A Web-Based Learning and Assessment Tool For Large ClassesDocument7 pagesThe Implementation and Evaluation of OASIS: A Web-Based Learning and Assessment Tool For Large Classesnur hayatiPas encore d'évaluation
- Verity & Ss Ansys West PNGDocument32 pagesVerity & Ss Ansys West PNGcklconPas encore d'évaluation
- STROBE Checklist Cross-SectionalDocument2 pagesSTROBE Checklist Cross-SectionalAmalia Riska G100% (1)
- Assessment of Investors' Investment Behaviour: Mediating Effect of Risk Tolerance: A Case of Pakistan Stock ExchangeDocument11 pagesAssessment of Investors' Investment Behaviour: Mediating Effect of Risk Tolerance: A Case of Pakistan Stock ExchangeanuPas encore d'évaluation
- Noe9e PPT Ch03 Accessible1Document33 pagesNoe9e PPT Ch03 Accessible1Darshilla Rive ChandramPas encore d'évaluation
- UK Home Office: Aud05Document14 pagesUK Home Office: Aud05UK_HomeOfficePas encore d'évaluation
- An Introduction To Quantitative Research Methods: DR Iman ArdekaniDocument74 pagesAn Introduction To Quantitative Research Methods: DR Iman ArdekaniSaranya SekharPas encore d'évaluation
- PMI Pulse of The Profession 2023 ReportDocument22 pagesPMI Pulse of The Profession 2023 ReportThauan GonçalvesPas encore d'évaluation
- How To Write A Research QuestionDocument7 pagesHow To Write A Research QuestionĐặng Thị Thu VânPas encore d'évaluation
- Designing Written Assessment of Student LearningDocument243 pagesDesigning Written Assessment of Student LearningCarlo Magno100% (18)
- Critical Thinking BasicsDocument84 pagesCritical Thinking BasicsMerly Torregoza Arandia100% (2)
- Feasibility Study: Dr. Rhia D. CervantesDocument49 pagesFeasibility Study: Dr. Rhia D. CervantesPatricia Camille Dela CruzPas encore d'évaluation
- Clinical Audit Report Aug 2013 WordDocument4 pagesClinical Audit Report Aug 2013 WordPiaPas encore d'évaluation
- Tableau Exasol WhitePaperDocument9 pagesTableau Exasol WhitePaperSagar NaiduPas encore d'évaluation
- Empathy With Fictional StoriesDocument11 pagesEmpathy With Fictional StoriesFranPas encore d'évaluation
- Examination PR 2Document6 pagesExamination PR 2ariane lagaticPas encore d'évaluation
- Sting MKTDocument8 pagesSting MKTVasu BansalPas encore d'évaluation