Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Bed Side Assessment of Adult PatientDocument60 pagesBed Side Assessment of Adult PatientDheeraj RaiPas encore d'évaluation
- ACLS Pre-TestDocument24 pagesACLS Pre-TestBaltej Sidhu80% (10)
- CDC Finally Released Its VAERS Safety Monitoring Analyses For COVID Vaccines Via FOIA - DailyCloutDocument23 pagesCDC Finally Released Its VAERS Safety Monitoring Analyses For COVID Vaccines Via FOIA - DailyCloutAndersonPas encore d'évaluation
- Classic Autopsy TechniquesDocument27 pagesClassic Autopsy TechniquesYenny BelindaPas encore d'évaluation
- Holistic Handbook: Andrew Williams, JRDocument32 pagesHolistic Handbook: Andrew Williams, JRAndrew Williams JrPas encore d'évaluation
- Vedic Astro 2013 05Document39 pagesVedic Astro 2013 05ramapvkPas encore d'évaluation
- Certificate: Dr. Desya Beatriks SilayaDocument1 pageCertificate: Dr. Desya Beatriks SilayaDesya SilayaPas encore d'évaluation
- DyspneaDocument2 pagesDyspneaDesya SilayaPas encore d'évaluation
- ReleaseNotes Vitrea6.5.3Document29 pagesReleaseNotes Vitrea6.5.3Humayun KhanPas encore d'évaluation
- The Curious Incident of The Dog in The Night TimeDocument227 pagesThe Curious Incident of The Dog in The Night TimeMarina MujicaPas encore d'évaluation
- Melasma 1Document4 pagesMelasma 1Desya SilayaPas encore d'évaluation
- Dok Baru 2020-07-08 18.43.51Document2 pagesDok Baru 2020-07-08 18.43.51Desya SilayaPas encore d'évaluation
- TOP LEADERBOARD 28 Nop 2020Document4 pagesTOP LEADERBOARD 28 Nop 2020Desya SilayaPas encore d'évaluation
- Certificate: Dr. Desya Beatriks SilayaDocument1 pageCertificate: Dr. Desya Beatriks SilayaDesya SilayaPas encore d'évaluation
- Ria Laporan PartusDocument24 pagesRia Laporan PartusDesya SilayaPas encore d'évaluation
- 08 05 2020 09.19.33Document1 page08 05 2020 09.19.33Desya SilayaPas encore d'évaluation
- Malaria Pregnancy NgassaDocument30 pagesMalaria Pregnancy NgassaMazterMaztermaztermazter MaztermaztermazterYandePas encore d'évaluation
- Status Pasien Slama PKMDocument8 pagesStatus Pasien Slama PKMDesya SilayaPas encore d'évaluation
- Angka Kejadian, Karakteristik Dan Gambaran Radiologi Foto Polos Abdomen Pada Pasien Ileus Obstruktif Di Rumah Sakit Al-Ihsan Bandung Tahun 2014-2015Document7 pagesAngka Kejadian, Karakteristik Dan Gambaran Radiologi Foto Polos Abdomen Pada Pasien Ileus Obstruktif Di Rumah Sakit Al-Ihsan Bandung Tahun 2014-2015susy susiatinPas encore d'évaluation
- Scan Akte ReducedDocument1 pageScan Akte ReducedDesya SilayaPas encore d'évaluation
- Scan KK ReducedDocument2 pagesScan KK ReducedDesya SilayaPas encore d'évaluation
- MalariaDocument1 pageMalariaDesya SilayaPas encore d'évaluation
- Malaria Pregnancy NgassaDocument30 pagesMalaria Pregnancy NgassaMazterMaztermaztermazter MaztermaztermazterYandePas encore d'évaluation
- Pathophysiology of Dyspnea: New England Journal of Medicine January 1996Document7 pagesPathophysiology of Dyspnea: New England Journal of Medicine January 1996Dilan RasyidPas encore d'évaluation
- Malaria Pregnancy NgassaDocument30 pagesMalaria Pregnancy NgassaMazterMaztermaztermazter MaztermaztermazterYandePas encore d'évaluation
- Pathophysiology of Dyspnea: New England Journal of Medicine January 1996Document7 pagesPathophysiology of Dyspnea: New England Journal of Medicine January 1996Dilan RasyidPas encore d'évaluation
- Dyspnoea: Pathophysiology and A Clinical Approach: ArticleDocument5 pagesDyspnoea: Pathophysiology and A Clinical Approach: ArticleadninhanafiPas encore d'évaluation
- Autopsy Report For Jonathan FerrellDocument11 pagesAutopsy Report For Jonathan FerrellWFAE 90.7 FMPas encore d'évaluation
- 7 PENYAKIT JANTUNG BAWAAN DR - YusraDocument57 pages7 PENYAKIT JANTUNG BAWAAN DR - YusraSurya ArhPas encore d'évaluation
- Nt-Probnp: The Gold Standard Biomarker in Heart FailureDocument3 pagesNt-Probnp: The Gold Standard Biomarker in Heart FailureRiuin23Pas encore d'évaluation
- Ace InhibitorsDocument26 pagesAce InhibitorsDeipa KunwarPas encore d'évaluation
- AUTOPSY ReezuDocument16 pagesAUTOPSY ReezuBnB UsmlePas encore d'évaluation
- Myocardial Infarction: Presentation by 1605-Abubakkar Raheel 1622 - Haider Ali 1606 - Ahmed Arsalan 1611 - Amaila AnamDocument38 pagesMyocardial Infarction: Presentation by 1605-Abubakkar Raheel 1622 - Haider Ali 1606 - Ahmed Arsalan 1611 - Amaila Anamfurr singhPas encore d'évaluation
- Cir 0000000000000899Document25 pagesCir 0000000000000899hanifa ambPas encore d'évaluation
- The Basics of Ekg: Presented byDocument31 pagesThe Basics of Ekg: Presented byRoiPas encore d'évaluation
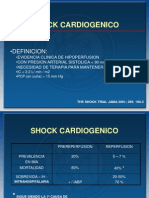
- Shock CardiogenicoDocument28 pagesShock CardiogenicoIngrid Robledo100% (1)
- 2nd Year Bio Mcqs For E.testDocument58 pages2nd Year Bio Mcqs For E.testMuhammad Sohail 845-FSL/LLB5Y/S22Pas encore d'évaluation
- RACE 2017 MegacodeDocument33 pagesRACE 2017 MegacodemickeyPas encore d'évaluation
- Circulatory SystemDocument44 pagesCirculatory SystemAdonai Jireh Dionne BalitePas encore d'évaluation
- Market Broiler Pens: Their Care and Management For 4-H and FFA MembersDocument22 pagesMarket Broiler Pens: Their Care and Management For 4-H and FFA MembersmutsaPas encore d'évaluation
- Submitted To: Endalkachew: Wolaita Sodo EthiopiaDocument32 pagesSubmitted To: Endalkachew: Wolaita Sodo Ethiopiaassefag92Pas encore d'évaluation
- Medical Treatment of Aortic Stenosis: in DepthDocument19 pagesMedical Treatment of Aortic Stenosis: in DepthAlexandra NalgomPas encore d'évaluation
- Circulatory System Class 5Document20 pagesCirculatory System Class 5zoey9099747888Pas encore d'évaluation
- ManifestFromTheHeart SDocument24 pagesManifestFromTheHeart Sjuliet rubyPas encore d'évaluation
- Sample Final Exam Questions-f14-KEYDocument6 pagesSample Final Exam Questions-f14-KEYAlias HedgePas encore d'évaluation
- Nellcor N-3000 - Service ManualDocument136 pagesNellcor N-3000 - Service ManualPaul Eduardo MunozPas encore d'évaluation
- Biol 1700 - Assignment 2Document16 pagesBiol 1700 - Assignment 2api-456450673100% (1)
- Cir 0000000000000549Document120 pagesCir 0000000000000549MSPas encore d'évaluation
- B1+ UNIT 7 Life Skills Video WorksheetDocument1 pageB1+ UNIT 7 Life Skills Video WorksheetMariana FernandesPas encore d'évaluation