Vous aimerez peut-être aussi
- Health and Safety Induction - ChecklistDocument3 pagesHealth and Safety Induction - ChecklistPerwez21100% (1)
- Netsmart Home Care and Hospice Survival GuideDocument8 pagesNetsmart Home Care and Hospice Survival GuidenishmehtaPas encore d'évaluation
- Nursing Process - Physical AssessmentDocument29 pagesNursing Process - Physical AssessmentFresie Belle Partosa100% (5)
- Prelim Exam PharmaDocument2 pagesPrelim Exam Pharmamj CanilangPas encore d'évaluation
- Testing and Beyond - Strategies and Tools For Evaluating and Assessing Infants and ToddlersDocument25 pagesTesting and Beyond - Strategies and Tools For Evaluating and Assessing Infants and ToddlersMargareta Salsah BeePas encore d'évaluation
- ArticleDocument5 pagesArticleJay StonePas encore d'évaluation
- Standardized Informed Consent Is A Key To Improving Patient SafetyDocument4 pagesStandardized Informed Consent Is A Key To Improving Patient SafetyNatasha BhasinPas encore d'évaluation
- Komunikasi Perawat 100322Document132 pagesKomunikasi Perawat 100322Shinta Azzahra PujihanPas encore d'évaluation
- 1.komunikasi Perawat 120719Document132 pages1.komunikasi Perawat 120719DIFP PROJECTPas encore d'évaluation
- Komunikasi Perawat 2017Document106 pagesKomunikasi Perawat 2017Komang PaulanggaPas encore d'évaluation
- Improving Discharge Planning Communication Between Hospitals and PatientsDocument6 pagesImproving Discharge Planning Communication Between Hospitals and PatientsHelmi JuwitaPas encore d'évaluation
- DOCUMENTATIONDocument9 pagesDOCUMENTATIONNashleyah AnayatinPas encore d'évaluation
- 10 1016@j Auec 2019 01 004Document5 pages10 1016@j Auec 2019 01 004Ervin WidhiantyasPas encore d'évaluation
- CHI ST Alexius Case StudyDocument4 pagesCHI ST Alexius Case StudysagarPas encore d'évaluation
- Clinical JudgementDocument6 pagesClinical Judgementapi-664535132Pas encore d'évaluation
- Nursing Documentation and Recording SystemsDocument8 pagesNursing Documentation and Recording SystemsDr Magda Bayoumi67% (3)
- GRP2 DocumentationDocument4 pagesGRP2 DocumentationHPas encore d'évaluation
- Hourly Rounds - An Evidence-Based PracticeDocument1 pageHourly Rounds - An Evidence-Based Practicesharvesh mahadeoPas encore d'évaluation
- Nur 410 Project On Informatics With Title Page 1Document11 pagesNur 410 Project On Informatics With Title Page 1api-597634889Pas encore d'évaluation
- Komunikasi Efektif Dan Keselamatan Pasien - Bahan Bu TikaDocument44 pagesKomunikasi Efektif Dan Keselamatan Pasien - Bahan Bu TikaZara Yuliani PutriPas encore d'évaluation
- Communication: Improving Patient Safety With SbarDocument7 pagesCommunication: Improving Patient Safety With Sbarria kartini panjaitanPas encore d'évaluation
- Estudio SupportDocument8 pagesEstudio Supportdaniel.rebel13Pas encore d'évaluation
- Discharge Delay in Acute Care Reasons and DeterminantsDocument9 pagesDischarge Delay in Acute Care Reasons and DeterminantsGabriela ObonPas encore d'évaluation
- Nejmp 1215594Document4 pagesNejmp 1215594Cj AlmazanPas encore d'évaluation
- Topic 15, 17, 18 Nurse's Notes, Curriculum VitaeDocument15 pagesTopic 15, 17, 18 Nurse's Notes, Curriculum VitaeSimran Josan100% (1)
- Safely Practicing in A New Environment: A Qualitative Study To Inform Physician Onboarding PracticesDocument7 pagesSafely Practicing in A New Environment: A Qualitative Study To Inform Physician Onboarding PracticesBuluguTraianLucianPas encore d'évaluation
- Bmjopen 2017 021107Document8 pagesBmjopen 2017 021107apouakone apouakonePas encore d'évaluation
- Ebp PosterDocument1 pageEbp Posterapi-283540594Pas encore d'évaluation
- Frontline Nurses' Clinical Judgment in Recognizing, Understanding, andDocument11 pagesFrontline Nurses' Clinical Judgment in Recognizing, Understanding, andPaulaPas encore d'évaluation
- Nur 410 Final PaperDocument7 pagesNur 410 Final Paperapi-377091267Pas encore d'évaluation
- Literature Review On Appointment Scheduling in Hospitals ManagementDocument4 pagesLiterature Review On Appointment Scheduling in Hospitals ManagementNatukwatsa NazetiPas encore d'évaluation
- Final Paper Nur410Document10 pagesFinal Paper Nur410api-598929897Pas encore d'évaluation
- Quality Improvement Proposal WorksheetDocument8 pagesQuality Improvement Proposal Worksheetapi-465165917Pas encore d'évaluation
- One Message January 2009Document2 pagesOne Message January 2009St George's Healthcare NHS TrustPas encore d'évaluation
- Improving Communication With Primary Care Physicians at The Time of Hospital DischargeDocument9 pagesImproving Communication With Primary Care Physicians at The Time of Hospital DischargeEmily MoriartyPas encore d'évaluation
- Bari 11Document104 pagesBari 11etsabayomiPas encore d'évaluation
- The Design of Inpatient Administration Information System at Midwife Clinic Hj. Aswilda JakartaDocument7 pagesThe Design of Inpatient Administration Information System at Midwife Clinic Hj. Aswilda JakartaLuis Andres GutierrezPas encore d'évaluation
- Nursing OperantDocument10 pagesNursing OperantMade Va RaiyawanPas encore d'évaluation
- Scholarly Research Paper - Reagan ToddDocument6 pagesScholarly Research Paper - Reagan Toddapi-735430277Pas encore d'évaluation
- Week 2 - 410 NURDocument5 pagesWeek 2 - 410 NURCherie BoyerPas encore d'évaluation
- Computerized Patient Information SystemDocument12 pagesComputerized Patient Information SystemChristianPas encore d'évaluation
- HA425M6 Domains of QualityDocument14 pagesHA425M6 Domains of QualityIsabella SydneyPas encore d'évaluation
- Ghosh 2021Document6 pagesGhosh 2021Yonatan MeshaPas encore d'évaluation
- Clinical Nursing Judgment Paper 1Document5 pagesClinical Nursing Judgment Paper 1api-740431489Pas encore d'évaluation
- Funda Finals Lec NotesDocument20 pagesFunda Finals Lec NotesPauline AñesPas encore d'évaluation
- Interdiscplinary Obstetric Case - Jaya KusumaDocument37 pagesInterdiscplinary Obstetric Case - Jaya KusumaBayu KurniawanPas encore d'évaluation
- (Pubmed) Protocolised Approach To End-Of-Life Care in The ICU-the ICU PALCare Pilot ProjectDocument6 pages(Pubmed) Protocolised Approach To End-Of-Life Care in The ICU-the ICU PALCare Pilot ProjectRahmida RahmyPas encore d'évaluation
- A 2020 Vision of Patient CenteredDocument13 pagesA 2020 Vision of Patient CenteredElya Amaliia100% (1)
- dlt1107 1447a 1449Document3 pagesdlt1107 1447a 1449abdulariifPas encore d'évaluation
- How To Normalize Emergencies in PracticeDocument3 pagesHow To Normalize Emergencies in PracticeMabe AguirrePas encore d'évaluation
- 1 PBDocument7 pages1 PBAngie MandeoyaPas encore d'évaluation
- Diagnostic Efficiency: Effects Communication Skills Training On Students'Document7 pagesDiagnostic Efficiency: Effects Communication Skills Training On Students'Yunita AiniPas encore d'évaluation
- Getting The Most From Your History and PhysicalDocument9 pagesGetting The Most From Your History and PhysicalSamian QuaziPas encore d'évaluation
- Failure Mode and Effect Analysis 1 PDFDocument3 pagesFailure Mode and Effect Analysis 1 PDFVina AfilianiPas encore d'évaluation
- Socko Low 2014Document8 pagesSocko Low 2014Tri Monarita JohanPas encore d'évaluation
- Clinical Nursing JudgementDocument8 pagesClinical Nursing Judgementapi-546517574Pas encore d'évaluation
- Fundamentals of Nursing (Midterm Topic 1)Document7 pagesFundamentals of Nursing (Midterm Topic 1)Manuel, Precious Marie B.Pas encore d'évaluation
- Accucare Clinic MGT SystDocument13 pagesAccucare Clinic MGT SystFred LisalitsaPas encore d'évaluation
- Tugas Summary Artikel 2-DikonversiDocument10 pagesTugas Summary Artikel 2-DikonversiAyu WulansariPas encore d'évaluation
- Capstone-Scholarly Capstone PaperDocument5 pagesCapstone-Scholarly Capstone Paperapi-653324233Pas encore d'évaluation
- Improving Documentation Using A Nursing ModelDocument10 pagesImproving Documentation Using A Nursing ModelLaraBindePas encore d'évaluation
- Enhancing Nursing Practice by Utilizing Voice RecoDocument8 pagesEnhancing Nursing Practice by Utilizing Voice RecosarvitaPas encore d'évaluation
- Primary Care Procedures in Women's Health: An International Guide for the Primary Care SettingD'EverandPrimary Care Procedures in Women's Health: An International Guide for the Primary Care SettingPas encore d'évaluation
- WHO Core Nurse Educator CompetenciesDocument1 pageWHO Core Nurse Educator Competenciesmj CanilangPas encore d'évaluation
- Pharmacology MCQDocument1 pagePharmacology MCQmj CanilangPas encore d'évaluation
- Chapter 46 Chest AssessmentDocument12 pagesChapter 46 Chest Assessmentmj CanilangPas encore d'évaluation
- Wifi HackingDocument3 pagesWifi Hackingmj CanilangPas encore d'évaluation
- Soliman SchedDocument1 pageSoliman Schedmj CanilangPas encore d'évaluation
- Grading System For NCM 103 - 103A - Funda SL and RDDocument2 pagesGrading System For NCM 103 - 103A - Funda SL and RDmj CanilangPas encore d'évaluation
- Grading System For NCM 100 - Skills Lectute and RDDocument2 pagesGrading System For NCM 100 - Skills Lectute and RDmj CanilangPas encore d'évaluation
- Alignment Matrix For PLOs Health AssessmentDocument4 pagesAlignment Matrix For PLOs Health Assessmentmj CanilangPas encore d'évaluation
- Funda RLE RD Time TableDocument4 pagesFunda RLE RD Time Tablemj CanilangPas encore d'évaluation
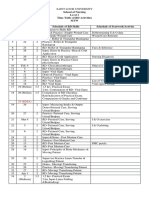
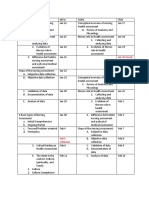
- School of Nursing Level 1 Time Table of RD Activities MTW Day Dates Hrs. Schedule of RD Skills Schedule of Seatwork/ActivityDocument4 pagesSchool of Nursing Level 1 Time Table of RD Activities MTW Day Dates Hrs. Schedule of RD Skills Schedule of Seatwork/Activitymj CanilangPas encore d'évaluation
- PA Lec SchedDocument5 pagesPA Lec Schedmj CanilangPas encore d'évaluation
- Grading System For NCM 100 - Skills Lectute and RDDocument2 pagesGrading System For NCM 100 - Skills Lectute and RDmj CanilangPas encore d'évaluation
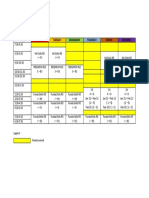
- Time Monday Tuesday Wednesday Thursday Friday SaturdayDocument1 pageTime Monday Tuesday Wednesday Thursday Friday Saturdaymj CanilangPas encore d'évaluation
- Schedule For Faculty Use - DHDocument1 pageSchedule For Faculty Use - DHmj CanilangPas encore d'évaluation
- Time Monday Tuesday Wednesday Thursday Friday SaturdayDocument1 pageTime Monday Tuesday Wednesday Thursday Friday Saturdaymj CanilangPas encore d'évaluation
- Teaching Problem Solving in Large Introductory Classes: The View From PhysicsDocument48 pagesTeaching Problem Solving in Large Introductory Classes: The View From PhysicsAlvaro H GalvisPas encore d'évaluation
- Wound CareDocument3 pagesWound Caremj CanilangPas encore d'évaluation
- Grade 3 - Password Power-Up - Lesson 2Document14 pagesGrade 3 - Password Power-Up - Lesson 2Sherel Jade CalixtoPas encore d'évaluation
- The American Dream of Tennessee Williams: The Social Dimension of Williams's DramaDocument15 pagesThe American Dream of Tennessee Williams: The Social Dimension of Williams's DramaEdin Spijodic100% (1)
- Anecdotal Record and Program 1 & 2Document12 pagesAnecdotal Record and Program 1 & 2Susan Llanes Katimbang100% (1)
- BALCO: The Disinvestment Story: Case Details: PriceDocument3 pagesBALCO: The Disinvestment Story: Case Details: PriceEkta KotwaniPas encore d'évaluation
- Software Development Apprenticeship Program VacancyDocument3 pagesSoftware Development Apprenticeship Program VacancyOmbatoPas encore d'évaluation
- 8607Document45 pages8607Emaan50% (2)
- Doctrine of The MeanDocument2 pagesDoctrine of The MeanstevePas encore d'évaluation
- 13-007 - Social Innovation - Business Invention and Social Solutions PDFDocument44 pages13-007 - Social Innovation - Business Invention and Social Solutions PDFGloria Lambo GillacoPas encore d'évaluation
- Other Side of The Dale - G. PhinnDocument195 pagesOther Side of The Dale - G. PhinnSalman MhdPas encore d'évaluation
- 7em SocDocument226 pages7em Socvenkat_nsnPas encore d'évaluation
- CV - Simon LockettDocument2 pagesCV - Simon LockettSimon LockettPas encore d'évaluation
- Aleksandra Vuletic, Censuse in 19th Century in SerbiaDocument25 pagesAleksandra Vuletic, Censuse in 19th Century in SerbiaDejan ZivanovicPas encore d'évaluation
- Tech Ops Strat - 2022-23 - PGP - 25may2022Document8 pagesTech Ops Strat - 2022-23 - PGP - 25may2022Rashesh S VPas encore d'évaluation
- The Heroes of Olympus - The Son of Neptune Discussion GuideDocument2 pagesThe Heroes of Olympus - The Son of Neptune Discussion GuideDisney Hyperion100% (1)
- Risnauli Tondang ResumeDocument3 pagesRisnauli Tondang ResumeBoslanPas encore d'évaluation
- Science Clinicals 5e Lesson PlanDocument5 pagesScience Clinicals 5e Lesson Planapi-214216212Pas encore d'évaluation
- Doing Business in SeoulDocument38 pagesDoing Business in SeoulJust BasumataryPas encore d'évaluation
- Anne R. Teppo. Qualitative Research Methods in Mathematics Education 11Document185 pagesAnne R. Teppo. Qualitative Research Methods in Mathematics Education 11Ryna WidyaPas encore d'évaluation
- Mental Status ExamDocument44 pagesMental Status ExamHershey Cordero Briones100% (1)
- The Hebrew University and ETeacherBiblicDocument54 pagesThe Hebrew University and ETeacherBiblicVicente AlmelaPas encore d'évaluation
- Asuncion, Alwin C. (Learning Task 2)Document1 pageAsuncion, Alwin C. (Learning Task 2)Alwin AsuncionPas encore d'évaluation
- 2 Organizational Citizenship BehivaorDocument18 pages2 Organizational Citizenship BehivaorShelveyElmoDiasPas encore d'évaluation
- ABET Professional Skills RubricDocument3 pagesABET Professional Skills Rubrictherond7Pas encore d'évaluation
- Ryan Boser's ResumeDocument1 pageRyan Boser's ResumeboserrPas encore d'évaluation
- 2020 School Directory Campus ListDocument56 pages2020 School Directory Campus ListAldo CatalanPas encore d'évaluation
- CSN Education Department - : Alternative Field Observation Activities PacketDocument12 pagesCSN Education Department - : Alternative Field Observation Activities Packetapi-533991072Pas encore d'évaluation
- Discipline Summary and Code of ConductDocument4 pagesDiscipline Summary and Code of ConductSky jacob PorrasPas encore d'évaluation
- Grade 11 Ela Course OutlineDocument3 pagesGrade 11 Ela Course Outlineapi-246304404Pas encore d'évaluation