Académique Documents
Professionnel Documents
Culture Documents
Va Medica: Atypical Swallowing: A Review
Transféré par
Julio AbarzuaTitre original
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Va Medica: Atypical Swallowing: A Review
Transféré par
Julio AbarzuaDroits d'auteur :
Formats disponibles
not permitted.
It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
REVIEWS
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
MINERVA STOMATOL 2014;63:217-27
Atypical swallowing: a review
C. MASPERO, C. PREVEDELLO, L. GIANNINI, G. GALBIATI, G. FARRONATO
® A
T C
H DI
Aim. Atypical swallowing is a myofunctional Maxillo-Facial and Odontostomatological Unit
problem consisting of an altered tongue po- Fondazione Ca’ Granda IRCCS,
sition during the act of swallowing. High in- Ospedale Maggiore Policlinico
IG E
cidence in population, multifactorial etiology
and the recurring connection with the pres-
ence of malocclusions made it a topic of strong
Department of Orthodontics
University of Milan, Milan, Italy
R M
interest and discussion in science. The purpose
of this review is to illustrate the current ori-
entation on the topic of atypical swallowing, nent results. There is also proof of a substan-
trying in particular to answer two questions: tial difference between the results obtained
P A
1) what kind of connection is there between from early (deciduous or primary mixed den-
atypical swallowing and malocclusion; 2) what tition) or later treatments.
O V
kind of therapy should be used to solve it. Conclusion. The biunique causal relation be-
Methods. This review was conducted on the tween atypical swallowing and malocclusion
Medline database [www.ncbi.nim.nih.gov/ suggests a multidisciplinary therapeutic ap-
C ER
pubmed] searching for the keywords “atypi- proach, orthodontic and myofunctional, to
cal swallowing” and “tongue thrust”. We ex- temporarily solve both problems. An early
Y
amined all the documents from the year 1990 diagnosis and a prompt intervention have a
onwards, excluding the ones about syndro- significantly positive influence on the thera-
mic cases of the central motor system. py outcome.
IN
Results. The causal relation between the two
problems seems to be biunique: some au- KEY WORDS: Dental occlusion - Orthodontics -
thors affirm that this oral habit starts as a Deglutition.
compensation mechanism for a preexisting
M
malocclusion (especially in case of open-
bite); other texts show that it has a tenden-
cy to exacerbate cases of malocclusion; it is
also proven that a non-physiological tongue
S wallowing is a complex physiological act
that allows the progression and transpor-
tation of bolus, saliva and liquids from the
thrust can negatively influence the progress oral cavity to the stomach. This essential life
of an ongoing orthodontic therapy. Thereby,
or other proprietary information of the Publisher.
the best therapeutic approach seems to be a
function implies an elaborate neuromuscu-
multidisciplinary one: beside orthodontics, lar mechanism induced by nerve impulses
which is necessary to correct the malocclu- transmitted by sensory receptors from the
sion, it is essential to set up a myofunctional tongue and lips.1-4
rehabilitation procedure to correct the oral The swallowing mechanism model in
habit, therefore granting long time perma- childhood physiologically implies the in-
terposition of the tongue between the
Corresponding author: Prof. G. Farronato, Università di
Milano, Via Commenda 10, 20100 Milan, Italy. bony bases, while in adults the tip of the
E-mail address: giampietro.farronato@unimi.it. tongue places itself on level with the in-
Vol. 63 - No. 6 MINERVA STOMATOLOGICA 217
not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
MASPERO ATYPICAL SWALLOWING
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
cisive papilla. The transition between the high incidence. According to Profit,7 only
two phases takes place gradually in a 12- 85-90% of adults show a proper swallow-
15 months period,together with the dental ing. This oral habit is frequently connected
eruption. 1-8 A failed transition to the adult with the presence of malocclusions.
model and the persistence of a childlike In particular:
deglutition mechanism is a pathologic con- — skeletal problems like open bite, ante
dition called atypical swallowing. In this inclination of the maxilla and post inclina-
altered tongue posture, the tip touches the tion of mandibular plane;
palatal surface of the front teeth or be- — dental problems like diastem, maxil-
tween the arches rather than the palate, lar incisor protrusion, overjet increase and
the dorsum is curved downwards and the overbite decrease.
base touches the posterior part of the pal- Rix studied a sample of 93 children be-
® A
ate and the anterior pharyngeal wall. This tween 7 and 12 years old: 61 of them suf-
condition causes a reduced contraction of fered from atypical swallowing and, be-
T C
the lower jaw elevator muscles while the tween these 61, 36% had a malocclusion.11
perioral muscles show a significant activ- Werlich visited 640 children from elemen-
H DI
ity, missing in physiological conditions.8 tary and junior high schools, and found that
30.4% suffered from atypical swallowing.
50.7% of these showed a class II – division
Kinds of atypical swallowing
IG E 1 and 98.5% had an open bite. Moreover, in
older children, he found a significant rela-
From the etiologic point of view, there tion between atypical swallowing and pos-
R M
are two kinds of atypical swallowing: pri- terior crossbite.12
mary and secondary. Primary atypical swal- Rogers compared a group of pediatric or-
lowing has a psychological cause, parental thodontic patients with a sample of children
over-nursing, and is often associated with a from public school, some of whom had or-
P A
general childish behavior, sleeping, appe- thodontic problems, and noticed that the in-
tite, digestion and mood disorders (a de- cidence of atypical swallowing was high in
O V
fensive attitude towards external stressful both groups (56.9% of students and 62.8%
situations). Secondary atypical swallowing, of orthodontic patients), and even more in
C ER
on the other hand, is caused by concurrent patients with open bite (98.2% and 92.8%
physical factors, such as: respectively).13
Y
— oral habits as thumb sucking, nail bit- Complex etiopathogenesis, high inci-
ing, bruxism, prolonged pacifier use; dence in population and the correlation
IN
— prolonged artificial breastfeeding and with dental-skeletal problems make atypical
weaning; swallowing a topic of strong interest in the
— short frenulum; orthodontic, myologic and speech-language
— genetic factors as palate and airways field, and it’s still a subject of discussion.
M
morphology and hereditary dysmorphia; This literature review is intended to re-
— hypertrophic adenoids and tonsils think the current scientific orientation, in
with a tendency to oral breathing; order to answer two fundamental questions:
— allergic rhinitis; 1) what kind of relation exists between
— abnormal head, lower jaw and tongue
or other proprietary information of the Publisher.
atypical swallowing and malocclusion;
posture. 2) what kind of therapy should be ar-
Atypical swallowing can also be simple or ranged to solve it.
complex, depending on the kind of tongue
thrust and the degree of contraction of the
mimic muscles (labial, facial and mental) Materials and methods
and of the lower jaw elevator muscles.
The failed transition from childhood to Searching for the keywords “atypical
adult deglutition is a problem with a very swallowing” and “tongue thrust” on the
218 MINERVA STOMATOLOGICA June 2014
not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
ATYPICAL SWALLOWING MASPERO
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
Pubmed Medline database (www.ncbi.nim. thodontic and myofunctional, to guarantee
nih.gov/pubmed), a systematic literature a long-term optimal result.
review on the topic of atypical swallowing Give the strong statistical association be-
has been done. tween atypical swallowing, oral breathing
Between the sources identified, we ex- and, subsequently, acute otitis media, many
cluded any text prior to the 1990s, since of the selected studied were both of od-
the object of our review has to be current; ontological and otolaryngological relevance
moreover, we didn’t take into consideration (about 13%)
texts about diseases of the central nervous Atypical swallowing is also topic of study
system, because they didn’t have any odon- in the gnathologic and posturologic fields
tological relevance. (11% of the articles selected). On one hand,
Some useful general considerations were the percentage of subjects with dysfunc-
® A
taken from textbooks relevant to the topic. tions on the TMJ showing atypical swallow-
ing as well is high; on the other, there is
T C
a statistic relation between altered tongue
Results position and altered cranial posture. The
H DI
causal relation between these problems,
With this method 82 articles, ranging 1990 though, is not investigated.
to 2014, have been selected. Not all of them
dealt with the casual relation between atyp-
IG E
ical swallowing and malocclusion. In most Discussion
of the articles the fact that atypical swallow-
R M
ing causes morphological anomalies was The first problem faced in doing this lit-
considered to be an axiom, inferred from erature review was to verify that the term
scientific evidence from the past. “atypical swallowing” is used by the major-
Within the authors that still choose to in- ity of authors with a wider meaning than
P A
vestigate this topic, about the 86% says that the definition we gave at the beginning. In
atypical swallowing is a risk factor of: general, it would be considered oral habit
O V
— alterations in teeth position (anteri- not only the tongue movement during the
or open bite, posterior cross-bite, incisors act of swallowing, but also an alteration
C ER
proinclination); of the resting position of the tongue itself.
— alterations in mimic and mastication Therefore it would be more appropriate
Y
muscles (hyperactivity and hypotony re- to talk about “tongue thrust” rather than
spectively). “swallowing disorders” or “atypical swal-
IN
We couldn’t find articles that proved its lowing” in the strict sense. The pressure of
influence on the growth of maxillar bones. the tongue alone during swallowing hap-
Other studies (about 14%) state that the pens in less than a second and wouldn’t be
altered morphofunctional development of enough to explain the correlation that it has
M
the stomatognathic apparatus is not caused with problems of the development of the
by atypical swallowing. Instead, the tongue dental-skeletal complex.
posture alteration would be the result of a This fact could have consequences on
physical defect, therefore being a compen- the moment of the diagnosis: if we had to
analyze the swallowing act alone, it would
or other proprietary information of the Publisher.
sation mechanism to overcome a preexist-
ing structural anomaly. be more likely to notice an alteration with a
Thirty-five percent of the articles selected simple objective test. But to analyze the rest-
discussed the type of therapy to set up for ing position would be harder and it could
an orthodontic patient with atypical swal- be necessary to use instrumental methods
lowing. All of them assert that orthodon- of diagnosis.
tics, as the only treatment, is not enough Some of the studies selected during this
to solve the problem. It would therefore be literature review aimed at evaluating the re-
necessary a multidisciplinary approach, or- liability of some instrumental investigation
Vol. 63 - No. 6 MINERVA STOMATOLOGICA 219
not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
MASPERO ATYPICAL SWALLOWING
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
to observe the position of the tongue in its on the other there is an adaptation swal-
different functional moments. Sonography lowing with interposition of the tongue be-
(real time B-mode sonography, M-mode tween the dental arches. Both factors could
ultrasounds) seems to be an effective and result in very hard to solve open-bites. Ac-
non-invasive procedure to see the tongue’s cording to the author, it would be primarily
movements in the different plans of the important to put the orthodontic patient in
space; cineradiography, carried out putting a program of myofunctional rehabilitation.
a lead marker on the tongue dorsum, would In support of this thesis are the authors
also be an effective method, but it’s invasive discussing the kind of therapy to set up for
using ionizing radiations; kinesiography al- orthodontic patients with “tongue thrust”,
lows to see any difference between the usu- saying that a multidisciplinary therapy
al occlusal position of the lower jaw and the is necessary for an ideal and long lasting
® A
position while swallowing; electromyogra- result. Orthodontic patients that cure the
phy of the perioral and mastication muscles malocclusion and not the oral habit are go-
T C
can spot an alteration in their activity (hy- ing to have a relapse.
peractivity of the labial and mentalis mus- Atypical swallowing is one of the most
cles, hypotonia of the masseter muscle).
H DI
frequent oral habits in pediatric population,
The point, though, is to determine if the but is rarely shown alone: it has a strong
“tongue thrust”, it being while swallow- association with prolonged thumb sucking
ing or during the resting position, is cause
IG E and oral breathing.
or consequence of the development of a Through the cephalometric tracings car-
malocclusion: there are different opinions ried out by Machado et al. (2011) it could
R M
about this. be noticed how individuals with “tongue
The majority of the texts analyzed sup- thrust” have a different position of the hy-
ports the hypothesis that the “tongue thrust” oid bone (more distance between the hyoid
can lead to dysgnathia. All the studies ana- bone and the maxillary plane) and a re-
P A
lyzed, though, prove their final thesis on duced pharyngeal airspace compared to in-
purely statistc data. Nobody can describe dividuals with a physiological swallowing.
O V
the series of biological moments that would This could influence the type of breathing,
lead, starting from the presence of a “tongue which in turn would increase the risk of de-
C ER
thrust”, to the consolidation of a structural veloping infections of the acoustic complex.
defect. According to the authors, the causal D’Alatri et al. (2012), in his study con-
Y
relation between dysfunction and dysmor- ducted on 35 children with acute otitis me-
phia would be therefore biunique. dia, atypical swallowing and oral breathing,
IN
Moreover, we found some case reports states that the myofunctional rehabilitation
that would prove how atypical swallowing of the Eustachian tubes, together with the
could complicate, or even prevent the prop- elimination of the oral habits, could be con-
er progress of an ongoing orthodontic ther- sidered a useful therapy for the treatment of
M
apy. In these cases, only after removing the subjects with a tendency to develop infec-
oral habit and putting the patient through tion of the middle ear.
myofunctional rehabilitation it would be It was interesting to notice how many au-
possible to finalize the orthodontic therapy. thors affirm that subjects with atypical swal-
In a study by Pedrazzi (1997) about the
or other proprietary information of the Publisher.
lowing have both TMJ problems and a dif-
open-bite therapy, he states that the first ferent posture compared to those who don’t
causes of a dental open-bite would be the have this oral habit. Machado et al. (2012)
“tongue thrust” and the masseter hypotony. conducted an investigation on teleradiogra-
During the orthodontic therapy, in those phies. Form the cephalometric tracings the
phases when the interarch relationship isn’t inclination of the cranial base proves to be
optimal and it’s not possible to take the altered compared to the body and the tooth
maximum intercuspation position, on one of the epistropheus (axis).
side the masseter muscular tone is reduced, It is not clear whether swallowing is a
220 MINERVA STOMATOLOGICA June 2014
not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
ATYPICAL SWALLOWING MASPERO
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
consequence or a cause, in this sense. It is mine a situation of atypical swallowing with
a fact though that the diagnosis for atypical subsequent neuromuscular disorders.
swallowing should bring up the diagnostic If the oral habit is contemporary to a mis-
question of other dysfunctions: respiratory, fortune, it is necessary a multidisciplinary
articular and postural. therapeutic approach that solves both prob-
All the articles about the type of therapy lems, since the persistence of the “tongue
to set up, when treating a subject with atyp- thrust” could prevent the success of the or-
ical swallowing, state that the orthodontic thodontic therapy and cause relapses in the
therapy as the only treatment is not enough long term.
to solve the problem, but it’s necessary to With an early diagnosis we can signifi-
have a multidisciplinary, orthodontic and cantly improve the prognosis, in fact, we
myofunctional approach, to ensure an ideal get better results in terms of quality and
® A
and long lasting result. durability with therapies that started with
Another important fact is that many think deciduous or primary mixed dentition.
T C
it’s necessary to intervene as soon as pos- A “tongue thrust” diagnosis is less easy
sible to remove the oral habit. In particular, than the one of an anomalous tongue ac-
according to Condò et al. (2012), a therapy
H DI
tivity while swallowing. If it’s not possible
carried out during the deciduous or the pri- to identify the situation from the objective
mary mixed dentition would have signifi- analysis, we can count on some instrumen-
cantly better results compared to therapies
IG E tal methods, such as electromyography, ki-
started later. nesiography and sonography.
It has to be taken into consideration that Since we saw that the presence of a
R M
many of the studies here analyzed start “tongue thrust” does not necessarily imply
from the premise that “tongue thrust” caus- the presence of a malocclusion, there’s no
es malocclusion, taking this as an axiom need for instrumental screening analysis for
from past researches. all the subjects in pediatric age, despite the
P A
As previously mentioned, atypical swal- high incidence of atypical swallowing in
lowing can influence otolaryngologic prob- population.
O V
lems, as acute otitis media, ad is often as- Viceversa, in case of patients with par-
sociated to TMJ dysfunctions. Anyhow, it is ticular malocclusions (especially anterior
C ER
a dysfunction of the stomatognathic system open-bite, posterior cross-bite, incisors pro-
that needs to be corrected. inclination), it is advisable to verify that
Y
there’s no negative influence by the tongue.
If that happened, it wouldn’t be possible to
IN
Conclusions carry on the orthodontic therapy regardless
of myofunctional rehabilitation.
Atypical swallowing is a complex prob- The planning of the most suitable thera-
lem, whose study has been a source of in- py has necessarily to be done based on the
M
terest for decades and still remains a subject subject’s features: the presence of any oral
of discussion under many aspects: etiology, habit, head and body posture, the degree
treatment and the association with dysfunc- of compliance of the patient. Any oral habit
tions and dysmorphias more or less located needs to be always detected precociously.
in the facial region.
or other proprietary information of the Publisher.
If the subject is still in deciduous or pri-
The relationship between the presence of mary mixed dentition, so still growing up, it
oral habits and the onset of disorders of the is worthy to try a re-educational approach
stomatognathic apparatus can be defined as before the orthodontic one. There are case
biunique. As atypical swallowing and the reports showing that just suspending oral
persistence of childhood oral habits can habits can lead to the self correction of the
affect the proper dental-skeletal develop- morphological defect. On the other hand,
ment, in the same way anatomical disorders if the subject is more mature from a den-
of the stomatognathic apparatus can deter- tal-skeletal point of view, an orthodontic
Vol. 63 - No. 6 MINERVA STOMATOLOGICA 221
not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
MASPERO ATYPICAL SWALLOWING
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
operation will be needed, still keeping the evaluation in skeletal Class II and Class III patients.
Prog Orthod 2012;13:226-36.
association with the myofunctional rehabili- 22. Machado AJ Jr, Crespo AN. A lateral cephalometric
tation. x-ray study of selected vertical dimensions in chil-
dren with atypical deglutition, Int J Orofacial Myol-
ogy 2010;36:17-26.
23. Emmerich A, Fonseca L, Elias AM, de Medeiros UV.
References The relationship between oral habits, oronasopha-
ryngeal alterations, and malocclusion in preschool
children in Vitória, Espírito Santo, Brazil. Cad saude
1. Giannì E. La nuova ortognatodonzia. Padua: Piccin; publica 2004;20:689-97.
1980. 24. Mason RM. Myths that persist about orofacial mycol-
2. Ramfjord SP, Ash MM. Occlusion. Philadelphia-Lon- ogy. Int J Orofacial Myology 2011;37:26-38.
don: Saunders Co; 1966. 25. Giuca MR, Pasini M, Pagano A, Mummolo S, Vanni
3. Farronato G, Giannini L, Riva R, Galbiati G, Maspero A. Longitudinal study on a rehabilitative model for
C., Correlations between malocclusions and dyslalias. correction of atypical swallowing. Eur J Paediatr Dent
Eur J Paediatr Dent 2012;13:13-8.
® A
2008;9:170-4.
4. Farronato GP, Preteroti AM, Salvato A, Bruno E. Rela- 26. Ciavarella D, Mastrovincenzo M, Sabatucci A, Parziale
tion between skeletal open bite and atypical degluti- V, Chimenti C. Effect of the Enveloppe Linguale Noc-
tion Arch Stomatol (Napoli) 1982;23:53-74. turne on atypical swallowing: surface electromyogra-
T C
5. Farronato G. Ortognatodonzia Vol I. Milan: Ediermes; phy and computerised postural test evaluation. Eur J
2013. Paediatr Dent 2010;11:141-5.
6. Stormer K, Pancherz H. Electromyography of the 27. Saccomanno S, Antonini G, D’Alatri L, D’Angelantonio
H DI
perioral and masticatory muscles in orthodontic M, Fiorita A, Deli R. Causal relationship between
patients with atypical swallowing. J Orofac Orthop malocclusion and oral muscles dysfunction: a model
1999;60:13-23. of approach. Eur J Paediatr Dent 2012;13:321-3.
7. Proffit W. Ortodonzia moderna. Second edition. Mi- 28. Kaya D, Taner TU. Management of an Adult with
lan: Elsevier Masson; 2001.
IG E Spaced Dentition, Class III Malocclusion and Open-
8. Dahan J. Tongue Disorders and jaw deformities. No- bite Tendency. Eur J Dent 2011;5:121-9.
sological aspects and therapeutic concepts. Mondo 29. Kulkarni GV, Lau D. A single appliance for the cor-
Ortod 1989;14:777-89.
R M
rection of digit-sucking, tongue-thrust, and posterior
9. Gallusi G. Compendio di odontostomatologia Pediat- cross bite. Pediatr Dent 2010;32:61-3.
rica. Padua: Piccin; 1985. 30. Meibodi SE, Meybodi SA, Meybodi EM. The effect of
10. Garattini G, Crozzoli P, Grasso G. Eziopatogenesi e mandibular tongue cribs on dentoskeletal changes in
trattamento precoce delle malocclusioni correlate al patients with Class II Division 1 malocclusions. World
perdurare della deglutizione atipica. Mondo ortodon- J Orthod 2010;11:23-6.
P A
tico 1991;2:149-56. 31. Celli D, Gasperoni E, Deli R. Long-term outcome
11. Rix RF. Deglutition and the teeth. Dent Rec in a patient with a dentoskeletal open-bite maloc-
1946;66:103-8. clusion treated without extraction. World J Orthod
O V
12. Werlich EP. The prevalence of variant swallowing 2007;8:344-56.
patterns in a group of Seattle school children. Mas- 32. Fukumitsu K, Ohno F, Ohno T. Lip sucking and lip
ter’s thesis, University of Washington; 1962. biting in the primary dentition: two cases treated
C ER
13. Rogers JH. Swallowing patterns of a normal-popula- with a morphological approach combined with lip
tion sample compared to those of patients from an exercises and habituation. Int J Orofacial Myology
Y
orthodontic practice. Am J Orthod 1961;17:674-9. 2003;29:42-57.
14. Marvin LH. Tongue thrust: a point of view. J Speech 33. Dahan JS, Lelong O. Effects of bite raising and occlu-
Hear Disord 1976;41:172-84. sal awareness on tongue thrust in untreated children.
15. Jalaly T, Ahrari F, Amini F. Effect of tongue thrust Am J Orthod Dentofacial Orthop 2003;124:165-72.
IN
swallowing on position of anterior teeth, J Dent Res 34. Cayley AS, Tindall AP, Sampson WJ, Butcher AR.
Dent Clin Dent Prospects 2009;3:73-7. Electropalatographic and cephalometric assessment
16. Shetty SR, Munshi AK. Oral habits in children--a of myofunctional therapy in open-bite subjects. Aust
prevalence study. J Indian Soc Pedod Prev Dent Orthod J 2000;16:23-33.
1998;16:61-6. 35. Alexander CD. Open bite, dental alveolar protrusion,
M
17. Störmer K, Pancherz H. Electromyography of the class I malocclusion: A successful treatment result.
perioral and masticatory muscles in orthodontic Am J Orthod Dentofacial Orthop 1999;116:494-
patients with atypical swallowing. J Orofac Orthop 500.
1999;60:13-23. 36. Ralli G, Ruoppolo G, Mora R, Guastini L. Deleterious
18. Tosello DO, Vitti M, Berzin F. EMG activity of the sucking habits and atypical swallowing in children
orbicularis oris and mentalis muscles in children with with otitis media with effusion. Int J Pediatr Otorhi-
or other proprietary information of the Publisher.
malocclusion, incompetent lips andatypical swallow- nolaryngol 2011;75:1260-4.
ing--part I. J Oral Rehabil 1998;25:838-46. 37. Cozza P, Di Girolamo S, Ballanti F, Panfilio F. Or-
19. Farronato G, Giannini L, Galbiati G, Stabilini SA, thodontist-otorhinolaryngologist: an interdisciplinary
Maspero C. Orthodontic-surgical treatment: neu- approach to solve otitis media. Eur J Paediatr Dent
romuscular evaluation in open and deep skeletal bite 2007;8:83-8.
patients. Prog Orthod 2013;14:41. 38. Weber P, Corrêa EC, Bolzan Gde P, Ferreira Fdos S,
20. Farronato G, Giannini L, Galbiati G, Grillo E, Maspe- Soares JC, da Silva AM. Chewing and swallowing in
ro C. Occlus-o-Guide® versus Andresen activator young women with temporomandibular disorder. Co-
appliance: neuromuscular evaluation. Prog Orthod das 2013;25:375-80.
2013;14:4. 39. Castelo PM, Gavião MB, Pereira LJ, Bonjardim LR.
21. Farronato G, Giannini L, Galbiati G, Sesso G, Maspe- Relationship between oral parafunctional/nutritive
ro C. Orthodontic-surgical treatment: neuromuscular sucking habits and temporomandibular joint dys-
222 MINERVA STOMATOLOGICA June 2014
not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
ATYPICAL SWALLOWING MASPERO
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
function in primary dentition. Int J Paediatr Dent 51. Piyapattamin T, Soma K, Hisano M. Temporary
2005;15:29-36. tongue thrust: failure during orthodontic treatment.
40. Emmerich A, Fonseca L, Elias AM, de Medeiros UV. Aust Orthod J 2002;18:39-46.
The relationship between oral habits, oronasopha- 52. Hotokezaka H, Matsuo T, Nakagawa M, Mizuno A,
ryngeal alterations, and malocclusion in preschool Kobayashi K. Severe dental open bite malocclusion
children in Vitória, Espírito Santo, Brazil. Cad Saude with tongue reduction after orthodontic treatment.
Publica 2004;20:689-97. Angle Orthod 2001;71:228-36.
41. Williamson EH, Hall JT, Zwemer JD. Swallowing pat- 53. Pedrazzi ME. Treating the open bite. J Gen Orthod
terns in human subjects with and without temporo- 1997;8:5-16.
mandibular dysfunction. Am J Orthod Dentofacial 54. De Souza DR, Semechini TA, Kröll LB, Berzin F. Oral
Orthop 1990;98:507-11. myofunctional and electromyographic evaluation of
42. Machado Júnior AJ, Crespo AN. Postural evaluation the anterior suprahyoid muscles and tongue thrust
in children with atypical swallowing: radiographic in patients with Class II/1 malocclusion submitted to
study. J Soc Bras Fonoaudiol 2012;24:125-9. first premolar extraction. J Appl Oral Sci 2007;15:24-8.
43. Fraser C. Tongue thrust and its influence in orthodon- 55. Kharbanda OP, Sidhu SS, Sundaram K, Shukla DK.
tics. Int J Orthod Milwaukee 2006;17:9-18. Oral habits in school going children of Delhi: a
® A
44. Peng CL, Jost-Brinkmann PG, Yoshida N, Chou HH, prevalence study. J Indian Soc Pedod Prev Dent
Lin CT. Comparison of tongue functions between 2003;21:120-4.
mature and tongue-thrust swallowing--an ultra- 56. Machado AJ Jr, Crespo AN. Cephalometric evaluation
sound investigation. Am J Orthod Dentofacial Orthop
T C
of the airway space and hyoid bone in children with
2004;125:562-70. normal and atypical deglutition: correlation study.
45. Kikyo T, Saito M, Ishikawa M. A study comparing Sao Paulo Med J 2012;130:236-41.
ultrasound images of tongue movements between 57. Machado AJ Jr, Crespo AN. Influence of mandibular
H DI
open bite children and normal children in the early morphology on the hyoid bone in atypical degluti-
mixed dentition period. J Med Dent Sci 1999;46:127- tion: a correlational study. Int J Orofacial Myology
37. 2011;37:39-46.
46. Fuhrmann R, Diedrich P. B-mode ultrasound scan- 58. Machado AJ Jr., Crespo AN. Cephalometric evaluation
ning of the tongue during swallowing. Dentomaxil-
IG E of the oropharyngeal space in children with atypical
lofac Radiol 1994;23:211-5. deglutition. Braz J Otorhinolaryngol 2012;78:120-5.
47. Fuhrmann R, Diedrich P. Video-supported dynamic 59. D’Alatri L, Picciotti PM, Marchese MR, Fiorita A. Alter-
B-mode sonography of tongue function during swal-
R M
native treatment for otitis media with effusion: eus-
lowing. Fortschr Kieferorthop 1993;54:17-26. tachian tube rehabilitation. Acta Otorhinolaryngol Ital
48. Kawamura M, Nojima K, Nishii Y, Yamaguchi H. A 2012;32:26-30.
cineradiographic study of deglutitive tongue move- 60. Condò R, Costacurta M, Perugia C, Docimo R. Atypi-
ment in patients with anterior open bite. Bull Tokyo cal deglutition: diagnosis and interceptive treatment.
Dent Coll 2003;44:133-9.
P A
A clinical study. Eur J Paediatr Dent 2012;13:209-14.
49. Monaco A, Cattaneo R, Spadaro A, Marchetti E, Bar-
one A. Prevalence of atypical swallowing: a kinesio-
graphic study. Eur J Paediatr Dent 2006;7:187-91. Conflicts of interest.—The authors certify that there is no
O V
50. Chawla HS, Suri S, Utreja A. Is tongue thrust that de- conflict of interest with any financial organization regarding
velops during orthodontic treatment an unrecognized the material discussed in the manuscript.
potential road block? J Indian Soc Pedod Prev Dent Received on October 2, 2013.
C ER
2006;24:80-3. Accepted for publication on July 14, 2014.
Y
Deglutizione atipica: revisione della letteratura
IN
L a deglutizione è un complesso atto fisiologico
che permette la progressione ed il trasporto del
bolo alimentare, della saliva e dei liquidi dalla cavità
ta è posta a contatto con la superficie palatina dei
denti anteriori o fra le arcate anziché sul palato, il
dorso è incurvato verso il basso e la base contatta la
M
orale allo stomaco. Questa funzione essenziale per zona più posteriore del palato e la parete anteriore
la vita implica un articolato meccanismo neuromus- della faringe. Tale condizione comporta una ridotta
colare indotto da impulsi nervosi trasmessi da recet- contrazione dei muscoli elevatori della mandibola,
tori sensitivi della lingua e delle labbra 1-4. mentre la muscolatura periorale mostra una signi-
Il modello di deglutizione infantile prevede fi- ficativa attività, assente in condizioni fisiologiche 8.
or other proprietary information of the Publisher.
siologicamente l’interposizione della lingua tra le Esistono diverse forme di deglutizione atipica.
basi ossee, mentre nel modello adulto la punta Dal punto di vista eziologico se ne distinguono
della lingua va a posizionarsi a livello della papilla due forme: la forma primaria e la forma secondaria.
retroincisiva. La transizione tra le due fasi avviene La deglutizione atipica primaria ha origine psico-
gradualmente in un periodo di 12-15 mesi, conte- logica, da iperaccudimento parentale, ed è spesso
stualmente all’eruzione degli elementi dentari 1,8. Il associata ad un generale atteggiamento infantile,
mancato passaggio al modello adulto, quindi il pro- a disturbi di sonno, appetito, digestione e umore
trarsi di una deglutizione simile a quella infantile, (atteggiamento di difesa a situazioni stressanti ester-
è una condizione patologica chiamata deglutizione ne). La deglutizione atipica secondaria, invece, è
atipica. In questa alterata postura linguale, la pun- conseguente a concomitanti fattori fisici, tra i quali:
Vol. 63 - No. 6 MINERVA STOMATOLOGICA 223
not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
MASPERO ATYPICAL SWALLOWING
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
— abitudini viziate come il succhiamento del di rivederne gli attuali orientamenti scientifici, per
pollice, l’onicofagia, il bruxismo, l’uso prolungato arrivare a rispondere a due quesiti fondamentali:
del succhiotto; 1) che tipo di rapporto causale esiste fra de-
— allattamento artificiale protratto e svezzamen- glutizione atipica e malocclusione;
to ritardato; 2) che tipo di terapia impostare per la sua
— frenulo corto; risoluzione.
— fattori genetici quali la morfologia del palato e
delle vie aeree e le disformosi ereditarie;
— adenoidi e tonsille ipertrofiche con tendenza Materiali e metodi
alla respirazione orale;
— riniti allergiche; Inserendo le parole chiave “atypical swallowing”
— anomalie posturali di cranio, mandibola e lin- e “tongue thrust”nella banca dati Medline di Pub-
gua. med [www.ncbi.nim.nih.gov/pubmed], é stata con-
La deglutizione atipica, inoltre, può essere dif- dotta una revisione sistematica della letteratura ri-
® A
ferenziata in semplice o complessa, a seconda del guardo il tema della deglutizione atipica.
tipo di spinta della lingua e del grado di contrazio- Tra le fonti individuate, si sono esclusi gli scritti
ne dei muscoli mimici (labiali, facciali e mentonie- precendenti agli anni ’90, in quanto l’oggetto del-
T C
ro) e dei muscoli elevatori della mandibola. la revisione vuole essere attuale; inoltre, non sono
Il mancato passaggio dalla deglutizione infanti- stati presi in considerazione gli articoli inerenti ma-
H DI
le a quella adulta è una problematica con inciden- lattie a carico del sistema nervoso centrale, poiché i
za elevatissima nella popolazione. Secondo Proffit trattati non contenevano spunti di pertinenza odon-
(2001), è stato riscontrato che solo l’ 85-90% degli toiatrica.
adulti presenta una deglutizione corretta 7. Questa Alcune utili considerazioni generali sono state
IG E
abitudine viziata è assai frequentemente associata
alla presenza di malocclusioni.
In particolare:
tratte da libri di testo inerenti all’argomento.
R M
— problematiche scheletriche quali open bite, Risultati
ante inclinazione del piano mascellare e post incli-
nazione del piano mandibolare; Con la metodica indicata sono stati selezionati
— problematiche dentarie quali diastemi, protru- 82 articoli, dal 1990 al 2014. Fra questi, non tutti
P A
sione degli incisivi superiori, aumento dell’overjet e affrontavano la questione del rapporto causale fra
riduzione dell’overbite 8-10. deglutizione atipica e malocclusione. Nella maggior
Rix (1946) studiò un campione di 93 bambini di parte dei trattati, il fatto che la deglutizione atipica
O V
età compresa fra 7 e 12 anni: 61 avevano una de- sia causa di anomalie morfologiche veniva conside-
glutizione atipica e, di loro, il 36% aveva una mal rato un assioma, derivante da evidenze scientifiche
C ER
occlusione 11. degli anni passati.
Werlich (1962) visitò 640 bambini delle scuole Degli autori che tutt’ora scelgono di indagare su
Y
elementari e delle medie, e trovò che il 30,4% ave- questa tematica, circa l’86% afferma che la degluti-
vano una deglutizione atipica. Di questi, il 50,7% zione atipica sia fattore di rischio di:
presentavano una seconda classe - prima divisione — alterazioni di posizionamento dentale (open-
IN
e il 98,5% avevano un open bite. Inoltre, nei bambi- bite anteriore,cross-bite posteriore eproinclinazione
ni di età maggiore, trovò una relazione significativa degli incisivi) 15,16;
tra deglutizione atipica e crossbite posteriore 12. — alterazione della funzionalità dei muscoli mi-
Rogers (1961) confrontò un gruppo di pazienti mici e masticatori (iperattività dei primi e ipotono
pediatrici ortodontici con un campione di bambi- dei secondi) 17-21.
M
ni della scuola pubblica, alcuni dei quali avevano Non sono invece stati trovati articoli in grado di
problemi ortodontici, e notò che l’incidenza di de- dimostrarne l’influenza sulla crescita delle ossa ma-
glutizione atipica era elevata in entrambi i gruppi scellari 22.
(56,9% negli scolari e 62,8% nei pazienti ortodonti- Un minor numero di studi (il 14% circa) afferma
ci). Questa era particolarmente elevata tra i soggetti che non è la deglutizione atipica a portare ad un
or other proprietary information of the Publisher.
con morso profondo (79,7% e 62,8% rispettivamen- alterato sviluppo morfofunzionale dell’apparato sto-
te), ma lo era ancor di più tra quelli con open bite matognatico. Viceversa, sarebbe l’alterazione della
(98,2% e 92,8%) 13,14. postura linguale ad essere il risultato di un difetto
L’eziopatogenesi complessa, l’elevata incidenza fisico, per cui si tratterebbe di un meccanismo di
nella popolazione e la correlazione con problemati- compensazione volto a superare un’anomalia strut-
che di tipo dento-scheletrico, rendono il tema della turale preesistente 23,24.
deglutizione atipica argomento di forte interesse in Il 35% degli articoli selezionati riguardava il tipo
ambito ortodontico, miologico e logopedico, ed è di terapia da impostare di fronte a un paziente or-
tutt’ora oggetto di innumerevoli discussioni. todontico con deglutizione atipica. La totalità di essi
La presente revisione della letteratura si propone afferma che l’ortodonzia, come unico trattamento,
224 MINERVA STOMATOLOGICA June 2014
not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
ATYPICAL SWALLOWING MASPERO
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
non è sufficiente per la risoluzione del problema. un’eventuale discrepanza fra la posizione occlusale
Sarebbe quindi necessario un approccio multidisci- abituale della mandibola e quella assunta durante
plinare, ortodontico e miofunzionale, per garantire la deglutizione 49; infine, l’elettromiografia della mu-
un risultato ottimale e stabile nel tempo 25-35. scolatura periorale e dei muscoli masticatori indivi-
Data la forte associazione statistica fra degluti- dua un’alterazione della loro attività (iperattività dei
zione atipica, respirazione orale e, di conseguenza, muscoli labiali e mentoniero, ipotono del muscolo
otite media acuta, molte delle ricerche individuate massetere) 17-21.
erano di pertinenza mista, odontoiatrica e otorino- Il fatto significativo sta però nell’individuare se
laringoiatrica (circa il 13%) 36,37. la “tongue thrust”, che sia durante la deglutizione o
La deglutizione atipica è inoltre argomento di durante la posizione di riposo, sia causa o conse-
studio in campo gnatologico e posturologico (11% guenza dello sviluppo di una malocclusione, e a tal
degli articoli selezionati). Da un lato, la percentuale proposito si sono trovate differenti opinioni.
di soggetti con disfunzioni a carico dell’ATM pre- La maggior parte della letteratura analizzata so-
sentanti anche deglutizione atipica è elevata 38-41; stiene l’ipotesi che la “tongue thrust” possa portare a
® A
dall’altro, esiste una relazione statistica significativa delle disgnazie. Tutti gli studi analizzati, però, dimo-
fra alterata postura linguale e alterata postura cra- strano la loro tesi finale sulla base di dati puramente
niale 42. La relazione causale fra queste problemati- statistici. Nessuno è in grado di descrivere la serie di
T C
che non è però affrontata. momenti biologici che porterebbero, partendo dalla
presenza di “tongue thrust”, al consolidamento di
H DI
un difetto strutturale. Secondo gli autori, il rapporto
Discussione causale tra disfunzione e dismorfosi sarebbe quindi
di tipo biunivoco.
La prima difficoltà riscontrata nel condurre la Inoltre, sono stati individuati alcuni case report
IG E
revisione della letteratura è stata constatare che il
termine “deglutizione atipica” viene utilizzato, dalla
maggior parte degli autori, con un significato più
che dimostrerebbero come la deglutizione atipica
possa complicare, se non impedire, il buon decorso
di una terapia ortodontica in atto. Nei casi suddetti,
R M
ampio rispetto alla definizione inizialmente enun- solo dopo aver rimosso l’abitudine viziata, sottopo-
ciata. In generale, verrebbe considerata abitudine nendo il paziente a una riabilitazione miofunzio-
viziata non solo il movimento linguale che avviene nale, si sarebbe riusciti a finalizzare la terapia orto-
durante l’atto deglutitorio, ma anche un’alterazione dontica 50-52.
P A
della posizione di riposo della lingua stessa 43. Sa- In uno studio di Pedrazzi (1997) riguardante la
rebbe dunque più appropriato parlare di “spinta lin- terapia dell’open-bite, si afferma che le prime cau-
guale” o “tongue thrust”, piuttosto che di “disordini se di un open-bite dentario sarebbero la “tongue
O V
della deglutizione” o “atypical swallowing” in sen- thrust” e l’ipotonia del massetere. Durante la terapia
so stretto. La sola pressione esercitata dalla lingua ortodontica, nelle fasi in cui il rapporto interarcata
C ER
durante la deglutizione si attua nel giro di poche non è ottimale e non è possibile assumere la posi-
frazioni di secondo e non sarebbe sufficiente a spie- zione di massima intercuspidazione, da un lato si
Y
gare la correlazione che essa ha con problematiche riduce il tono muscolare masseterino, dall’altro s’in-
dello sviluppo del complesso dento-scheletrico 7. staura una deglutizione di adattamento con interpo-
Questo dato potrebbe avere conseguenze sul sizione della lingua fra le arcate dentarie. Entrambi
IN
momento della diagnosi: se si dovesse analizzare i fattori potrebbero risultare in open-bite molto dif-
solo l’atto della deglutizione, sarebbe più probabile ficili da risolvere. Secondo l’autore, sarebbe quindi
rilevarne un’alterazione semplicemente con l’esa- di primaria importanza l’inserimento del paziente
me obiettivo. Per l’analisi della posizione di riposo ortodontico in un programma di riabilitazione mio
invece, ciò risulterebbe più complesso e potrebbe funzionale 53.
M
essere necessario ricorrere a metodi diagnostici di A sostegno di questa tesi si collocano gli autori
tipo strumentale. che discutono sul tipo di terapia da impostare per
Alcuni studi fra quelli selezionati durante la re- pazienti ortodontici con “tongue thrust”, afferman-
visione della letteratura avevano lo scopo di valu- do che una terapia multidisciplinare è necessaria
tare l’affidabilità di alcune indagini strumentali per per un risultato ottimale e stabile nel tempo 25-35.
or other proprietary information of the Publisher.
l’osservazione della posizione linguale nei suoi vari Pazienti ortodontici che risolvono esclusivamente la
momenti funzionali. La sonografia (real time B-mo- malocclusione e non l’abitudine viziata vanno in-
de sonography, M-mode ultrasounds) sembrerebbe contro a recidive 54.
essere una procedura efficace e non invasiva per La deglutizione atipica è l’abitudine viziata fra
visualizzare i movimenti della lingua nei piani dello le più frequenti nella popolazione pediatrica, ma
spazio 44-47; la cineradiografia, effettuata ponendo spesso non si manifesta da sola: forte è la sua asso-
un marcatore di piombo sul dorso linguale, sarebbe ciazione con il succhiamento protratto del pollice e
anch’essa una metodica efficace 48, ma è invasiva la respirazione orale 22, 23, 55.
in quanto prevede l’utilizzo di radiazioni ionizzanti; Tramite tracciati cefalometrici eseguiti da Macha-
la kinesiografia computerizzata consente di rilevare do et al. (2011), si è potuto notare come individui
Vol. 63 - No. 6 MINERVA STOMATOLOGICA 225
not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
MASPERO ATYPICAL SWALLOWING
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
con “tongue thrust” abbiano una posizione diversa plici aspetti: l’eziologia, il trattamento e l’associazio-
dell’osso ioide (distanza maggiore osso ioide – pia- ne con disfunzioni e dismorfosi più o meno localiz-
no mandibolare) e uno spazio aereo faringeo ridotto zate nel distretto facciale.
rispetto a individui con una deglutizione fisiologica. Il rapporto tra presenza di abitudini viziate e in-
Questo potrebbe influenzare il tipo di respirazione, sorgenza di alterazioni a carico dell’apparato stoma-
che a sua volta aumenterebbe il rischio di sviluppa- tognatico può essere definito biunivoco. Così come
re infezioni del complesso acustico 56-58. la deglutizione atipica e il persistere di abitudini
D’Alatri et al. (2012), con il suo studio condot- viziate infantili può ripercuotersi sul corretto svilup-
to su 35 bambini con otite media acuta, degluti- po dento-scheletrico, allo stesso modo alterazioni
zione atipica e respirazione orale, afferma che la anatomiche dell’apparato stomatognatico possono
riabilitazione miofunzionale delle tube di Eustachio, determinare un quadro di deglutizione atipica con
accompagnata da una rimozione delle abitudini vi- conseguenti alterazioni neuromuscolari.
ziate, può essere considerata una terapia utile per Nel caso l’abitudine viziata sia contemporanea a
il trattamento di soggetti con predisposizione alle una disgnazia, è necessario un approccio terapeu-
® A
infezioni dell’orecchio medio 59. tico multidisciplinare che risolva entrambe le pro-
Interessante è stato rilevare come molti sostenga- blematiche in quanto, il permanere della “tongue
no che soggetti con deglutizione atipica abbiano sia thrust”, potrebbe ostacolare o impedire la riuscita
T C
problemi all’ATM, che una diversa postura rispetto della terapia ortodontica e causare recidive nel lun-
a chi non ha quest’abitudine viziata 38-41. Sempre go termine.
H DI
Machado et al. (2012) ha condotto un’indagine su Con una diagnosi precoce si può migliorare la
radiografie latero laterali. Dai tracciati cefalometrici prognosi sensibilmente. Infatti, da terapie iniziate
risulta alterata l’inclinazione della base cranica ri- in dentizione decidua o mista primaria si ottengono
spetto al corpo e al dente dell’epistrofeo 42. migliori risultati in termini di qualità e stabilità nel
IG E
Che la deglutizione sia una conseguenza o una
causa in questo senso, non è chiaro. Sta di fatto
che la diagnosi di deglutizione atipica dovrebbe far
tempo.
La diagnosi di “tongue thrust” è meno semplice
di quella di un’anomala attività linguale durante la
R M
scattare il quesito diagnostico di altre disfunzioni: deglutizione. Nel caso in cui dall’esame obiettivo
repiratorie, articolari e posturali. non sia possibile identificare la situazione, si può
La totalità degli articoli trattanti il tipo di tera- contare su alcune indagini strumentali, quali l’elet-
pia da impostare, qualora ci si trovi di fronte a un tromiografia, la kinesiografia e la sonorografia.
P A
soggetto con deglutizione atipica, affermano che la Poiché si è visto che la presenza di “tongue
terapia ortodontica come unico trattamento non è thrust” non implica necessariamente la presenza di
sufficiente per la risoluzione del problema, ma è ne- una mal occlusione 7, non risultano necessarie inda-
O V
cessario un approccio multidisciplinare, ortodontico gini strumentali di screening per i tutti i soggetti in
e miofunzionale, per garantire un risultato ottimale età pediatrica, nonostante l’elevata incidenza della
C ER
e stabile nel tempo. deglutizione atipica nella popolazione.
Un altro dato importante è che molti ritengono Viceversa, nel caso di pazienti aventi particolari
Y
che sia necessario intervenire al più presto per ri- malocclusioni (soprattutto open bite anteriore, cross
muovere l’abitudine viziata. In particolare secondo bite posteriore, proinclinazione degli incisivi), è in-
Condò et al. (2012), una terapia svolta durante den- dicato verificare che non vi sia un’influenza nega-
IN
tizione decidua o mista primaria avrebbe risultati tiva da parte della lingua.Se ciò fosse vero, non si
significativamente migliori rispetto a terapie iniziate potrebbe procedere con la terapia ortodontica in-
più tardivamente 60. dipendentemente da una riabilitazione miofunzio-
E’opportuno considerare che molti degli studi nale.
L’impostazione del piano terapeutico più op-
M
analizzati partono dal presupposto che la “tongue
thrust” sia causa di malocclusione, assumendolo portuno per la sua attuazione deve necessariamen-
come assioma da ricerche del passato. te essere effettuato alla luce di quelle che sono le
Come già menzionato in precedenza, la deglu- caratteristiche del singolo soggetto: la presenza di
tizione atipica può influenzare problematiche oto- eventuali abitudini viziate, la postura della testa e
rinolaringoiatriche, come l’otite media acuta, ed è del corpo, il grado di collaborazione del paziente.
or other proprietary information of the Publisher.
spesso associata a disfunzioni dell’ATM. In ogni Eventuali abitudini viziate devono essere sempre in-
caso si tratta di una disfunzione dell’apparato sto- tercettate precocemente.
matognatico che va corretta. Se il soggetto in esame è ancora in dentizione
decidua o mista primaria, quindi ancora in piena
fase di crescita, vale la pena tentare un approccio
Conclusioni rieducativo prima ancora di quello ortodontico.
Vi sono infatti case report dimostranti che la sola
La deglutizione atipica è una problematica com- sospensione delle abitudini viziate possa portare
plessa, il cui studio è fonte d’interesse da decenni e all’autocorrezione del difetto morfologico. Se inve-
tutt’ora rimane oggetto di discussione sotto molte- ce il soggetto ha una maturità dento-sheletrica più
226 MINERVA STOMATOLOGICA June 2014
not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo,
means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is
ATYPICAL SWALLOWING MASPERO
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies
(either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other
avanzata, occorrerà senz’altro intervenire con l’orto- Risultati. Il rapporto causale fra le due proble-
donzia, mantenendo pur sempre l’associazione con matiche sembra essere biunivoco: alcuni autori
la riabilitazione miofunzionale. sostengono che l’abitudine viziata si instauri come
meccanismo di compensazione di una malocclu-
sione preesistente (soprattutto in caso di open-
Riassunto bite); altri scritti documentano come essa tenda
ad esacerbare quadri di malocclusione; è inoltre
Obiettivo. La deglutizione atipica è una proble- dimostrato che una spinta linguale non fisiologica
matica di natura miofunzionale caratterizzata da possa influenzare negativamente l’andamento di
un’alterata postura linguale durante l’atto deglutito- una terapia ortodontica in corso. Di conseguen-
rio. L’ elevata prevalenza nella popolazione, l’ezio- za, l’approccio terapeutico migliore risulta essere
logia multifattoriale e la frequente associazione con quello mutidisciplinare: accanto all’ortodonzia,
la presenza di malocclusioni hanno fatto sì che di- necessaria per correggere la malocclusione, è es-
venisse argomento di forte interesse e di dibattito in senziale impostare un iter di riabilitazione mio-
® A
ambito scientifico. funzionale per correggere l’abitudine viziata, ga-
La presente revisione della letteratura si propone rantendo così dei risultati stabili a lungo termine.
di illustrare gli attuali orientamenti sul tema della E’ inoltre documentata una differenza significativa
T C
deglutizione atipica, cercando in particolare di ri- fra i risultati ottenuti da un trattamento iniziato
spondere a due quesiti: 1) che tipo di correlazione precocemente (dentizione decidua o mista prima-
H DI
esiste fra deglutizione atipica e malocclusione; 2) ria) oppure successivamente.
che tipo di terapia impostare per la sua risoluzione. Conclusioni. Il rapporto di biunivocità causale
Metodi. La revisione è stata condotta sulla banca tra deglutizione atipica e malocclusione suggerisce
dati Medline [www.ncbi.nim.nih.gov/pubmed] inse- un approccio terapeutico multidisciplinare, orto-
IG E
rendo le parole chiave “atypical swallowing” e “ton-
gue thrust”. Sono stati esaminati tutti i documenti
dal 1990 in poi, escludendo quelli inerenti a quadri
dontico e miofunzionale, per la risoluzione contem-
poranea delle due problematiche. La diagnosi pre-
coce e l’intervento tempestivo influenzano in modo
R M
sindromici del sistema motorio centrale. significativamente positivo l’esito della terapia.
P A
O V
C ER
Y
IN
M
or other proprietary information of the Publisher.
Vol. 63 - No. 6 MINERVA STOMATOLOGICA 227
Vous aimerez peut-être aussi
- Minerva Stomatol 217Document6 pagesMinerva Stomatol 217Dino MainoPas encore d'évaluation
- Impacted Maxillary Canine On The PositioDocument9 pagesImpacted Maxillary Canine On The PositioFranz Willman Chiguala MixanPas encore d'évaluation
- Jurnal 2Document10 pagesJurnal 2Dudeperfect666Pas encore d'évaluation
- Va Medica: Consensus Report Italiano Sul Trattamento Con Tossina Botulinica Per Uso EsteticoDocument13 pagesVa Medica: Consensus Report Italiano Sul Trattamento Con Tossina Botulinica Per Uso EsteticoEmiliano Prandelli100% (1)
- Clark y Goon 2015Document18 pagesClark y Goon 2015abraham landaetaPas encore d'évaluation
- Action Observation and Mirror Neuron Network: A Tool For Motor Stroke RehabilitationDocument7 pagesAction Observation and Mirror Neuron Network: A Tool For Motor Stroke RehabilitationElias VillalonPas encore d'évaluation
- R34Y2019N01A0039Document7 pagesR34Y2019N01A0039Jessica EsparzaPas encore d'évaluation
- Clean Intermittent Cath 2011Document10 pagesClean Intermittent Cath 2011Angger SatriaPas encore d'évaluation
- Va Medica: Treatment Efficacy of Language and Calculation Disorders and Speech Apraxia: A Review of The LiteratureDocument21 pagesVa Medica: Treatment Efficacy of Language and Calculation Disorders and Speech Apraxia: A Review of The LiteraturemohamerrPas encore d'évaluation
- Mars3 Tech 600-12000 20200805Document6 pagesMars3 Tech 600-12000 20200805Daniel Lack PendásPas encore d'évaluation
- Mars III RangeDocument4 pagesMars III RangeRenardPas encore d'évaluation
- Va Medica: Prevention and Conservative Management of Acute Kidney InjuryDocument14 pagesVa Medica: Prevention and Conservative Management of Acute Kidney InjuryRobertPas encore d'évaluation
- R33Y2014N04A0383Document11 pagesR33Y2014N04A0383Yadareli DothéPas encore d'évaluation
- 2014, Fisioterapia Na EscolioseDocument11 pages2014, Fisioterapia Na EscolioseLuana ScuveroPas encore d'évaluation
- The Success of Indirect Restorations in Posterior Teeth: A Systematic Review of The LiteratureDocument11 pagesThe Success of Indirect Restorations in Posterior Teeth: A Systematic Review of The LiteratureIvy MedPas encore d'évaluation
- EJPRM2012Document11 pagesEJPRM2012Grown LindaPas encore d'évaluation
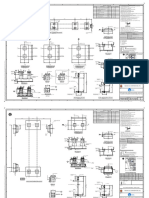
- Structural Notes: Seaoil Filling StationDocument1 pageStructural Notes: Seaoil Filling StationCasmir TayagPas encore d'évaluation
- EX350i Service Manual 2Document167 pagesEX350i Service Manual 2joaofavioPas encore d'évaluation
- Service Diagram ICONS 9845160072Document3 pagesService Diagram ICONS 9845160072kovács SándorPas encore d'évaluation
- 2271-711-JSD-1530-01 - C Telecoms Philosophy PDFDocument67 pages2271-711-JSD-1530-01 - C Telecoms Philosophy PDFSay Hong Jeffrey Tan0% (1)
- Pages From Two - Stage - Booster PDFDocument16 pagesPages From Two - Stage - Booster PDFVRV.RELATORIO.AVARIA RELATORIO.AVARIA100% (1)
- Mars3 Tech 600-12000 20190905Document6 pagesMars3 Tech 600-12000 20190905Miguel Catarino HuertaPas encore d'évaluation
- 6300L Carrier ROB CDocument120 pages6300L Carrier ROB Cvmg guindastesPas encore d'évaluation
- 114 - Method Statement For Bored Cast in Situ Pile - R2 PDFDocument42 pages114 - Method Statement For Bored Cast in Situ Pile - R2 PDFDadi YashwantPas encore d'évaluation
- Ad 2.5-33-O Standard Departure Chart Instrument (Sid) Rwy 30 Merva 1f, Gitla 1f, Suvas 1f, Salam 4f, Tomal 4fDocument2 pagesAd 2.5-33-O Standard Departure Chart Instrument (Sid) Rwy 30 Merva 1f, Gitla 1f, Suvas 1f, Salam 4f, Tomal 4fRoyal ArtzPas encore d'évaluation
- General Design Specification: 076971C 0000 JSD 1700 01 B 1/59Document59 pagesGeneral Design Specification: 076971C 0000 JSD 1700 01 B 1/59aegean227Pas encore d'évaluation
- Discovery Day Poster FinalDocument1 pageDiscovery Day Poster Finalapi-352110215Pas encore d'évaluation
- GRP Scheme of Switchgear Generator, GT and UT 35620061800R00Document136 pagesGRP Scheme of Switchgear Generator, GT and UT 35620061800R00Rukma Goud Shakkari100% (1)
- Dig 525 (061017)Document19 pagesDig 525 (061017)Bernard MendisPas encore d'évaluation
- Rotodynamic PumpsDocument2 pagesRotodynamic PumpsDavid AguilarPas encore d'évaluation
- SCP Rem As Built 190317 RevptsbDocument194 pagesSCP Rem As Built 190317 RevptsbHeri yantoPas encore d'évaluation
- Reference Drawing Bill of Material For This Drawing General Notes Topographic Symbols Pipeline Symbols Soil SymbolsDocument26 pagesReference Drawing Bill of Material For This Drawing General Notes Topographic Symbols Pipeline Symbols Soil SymbolssubudhiprasannaPas encore d'évaluation
- Brochure SP Option Plus UK HDDocument2 pagesBrochure SP Option Plus UK HDkentPas encore d'évaluation
- 9829300122-01 GA90+-160 Service DiagramDocument33 pages9829300122-01 GA90+-160 Service DiagramFloydMG TecnominPas encore d'évaluation
- Efficacy of Modified Constraint-Induced Movement Therapy in Acute StrokeDocument9 pagesEfficacy of Modified Constraint-Induced Movement Therapy in Acute Strokesolythaxx.96Pas encore d'évaluation
- Maxillary All-On-Four''Document5 pagesMaxillary All-On-Four''Qiiqa JuarezPas encore d'évaluation
- Defence OdisaDocument3 pagesDefence OdisaMangal RajakPas encore d'évaluation
- Tetric EvoFlow Bulk FillDocument48 pagesTetric EvoFlow Bulk FillJuanTabarésPas encore d'évaluation
- Balance Training Improves Static StabilityDocument13 pagesBalance Training Improves Static StabilityDANAE AYALAPas encore d'évaluation
- SystemsDocument1 pageSystemsumPas encore d'évaluation
- Y - C - AUDIO - HEAD AMP SCHEMATIC DIAGRAM - FTP Directory ListingDocument12 pagesY - C - AUDIO - HEAD AMP SCHEMATIC DIAGRAM - FTP Directory ListingWalter MartínezPas encore d'évaluation
- ZR-ZT 132-160 VSD Electrical Diagram EN Antwerp 9823547533 Ed02Document29 pagesZR-ZT 132-160 VSD Electrical Diagram EN Antwerp 9823547533 Ed02pachara sarntiyakulPas encore d'évaluation
- React 2 BattDocument2 pagesReact 2 BattpotoculPas encore d'évaluation
- Atlas Copco Wiring A38Document2 pagesAtlas Copco Wiring A38Mochamad fandi Dharmawan100% (1)
- Toptal PortfolioDocument40 pagesToptal PortfolioĐorđe IvanovićPas encore d'évaluation
- Bim Aft Ar 059Document1 pageBim Aft Ar 059vern pamPas encore d'évaluation
- Procedure For Positive Material Identification at Vendor'S WorksDocument7 pagesProcedure For Positive Material Identification at Vendor'S WorksAjay BaggaPas encore d'évaluation
- Extn 34001175ZD - CaDocument10 pagesExtn 34001175ZD - Cadeltatech.thaiPas encore d'évaluation
- 030 RFI ELLIPSE Beam Admin Auditorium ACT Response 20231113Document4 pages030 RFI ELLIPSE Beam Admin Auditorium ACT Response 20231113Muriyanto MuriPas encore d'évaluation
- KEC RWSS GAN KHA SLU GA 014 Layout1Document1 pageKEC RWSS GAN KHA SLU GA 014 Layout1IkramPas encore d'évaluation
- Standby Sru & Additional Tanks: Indian Oil Corporation LTDDocument5 pagesStandby Sru & Additional Tanks: Indian Oil Corporation LTDkhandelwalaPas encore d'évaluation
- Article: Early Rehabilitation Treatment in Newborns With CMTDocument7 pagesArticle: Early Rehabilitation Treatment in Newborns With CMTAngélicaPas encore d'évaluation
- IONIX ModelDocument6 pagesIONIX ModelTrường Bửu TrầnPas encore d'évaluation
- Effects of Mini Trampoline Exercise On MDocument5 pagesEffects of Mini Trampoline Exercise On MGuilhermeConradPas encore d'évaluation
- E Poster - Idiopathic Spontaneous PneumothoraxDocument1 pageE Poster - Idiopathic Spontaneous PneumothoraxMuyiwa AremuPas encore d'évaluation
- Jackson Street GateDocument1 pageJackson Street GatePaolo MadambaPas encore d'évaluation
- Dang A Rang A Dang Do!Document5 pagesDang A Rang A Dang Do!tancaden7877Pas encore d'évaluation
- Ven Espíritu DivinoDocument2 pagesVen Espíritu DivinoricardogranaracadenaPas encore d'évaluation
- MZ.D Lote 12 - UBICACIONDocument1 pageMZ.D Lote 12 - UBICACIONJuan ZegarraPas encore d'évaluation
- Roberts, Stephen, BeightonDocument10 pagesRoberts, Stephen, BeightonJulio AbarzuaPas encore d'évaluation
- Roberts, Stephen, BeightonDocument10 pagesRoberts, Stephen, BeightonJulio AbarzuaPas encore d'évaluation
- 2Document13 pages2Elena PruniciPas encore d'évaluation
- Roberts, Stephen, BeightonDocument10 pagesRoberts, Stephen, BeightonJulio AbarzuaPas encore d'évaluation
- Caring For Infants and Their Families: CraniosynostosisDocument13 pagesCaring For Infants and Their Families: CraniosynostosisJulio AbarzuaPas encore d'évaluation
- Treatment Timing and Multidisciplinary Approach in Apert SyndromeDocument6 pagesTreatment Timing and Multidisciplinary Approach in Apert SyndromeJulio AbarzuaPas encore d'évaluation
- t3 Som 2014 2Document14 pagest3 Som 2014 2Julio AbarzuaPas encore d'évaluation
- Embriologia Humana y Biologia Del Desarrollo CarlsonDocument14 pagesEmbriologia Humana y Biologia Del Desarrollo CarlsonJulio AbarzuaPas encore d'évaluation
- Caring For Infants and Their Families: CraniosynostosisDocument13 pagesCaring For Infants and Their Families: CraniosynostosisJulio AbarzuaPas encore d'évaluation
- Skull Base Embryology: A Multidisciplinary ReviewDocument10 pagesSkull Base Embryology: A Multidisciplinary ReviewJulio AbarzuaPas encore d'évaluation
- t2 Cendekiawan 2010 PDFDocument9 pagest2 Cendekiawan 2010 PDFJulio AbarzuaPas encore d'évaluation
- Sajnani, 2015Document7 pagesSajnani, 2015Julio AbarzuaPas encore d'évaluation
- t3 Som 2014 1Document8 pagest3 Som 2014 1Julio AbarzuaPas encore d'évaluation
- 11Document9 pages11Din PcPas encore d'évaluation
- Frazier-Bowers Et Al, 2016Document11 pagesFrazier-Bowers Et Al, 2016Julio AbarzuaPas encore d'évaluation
- Topical Review: Sleep Bruxism, Headaches, and Sleep-Disordered Breathing in Children and AdolescentsDocument10 pagesTopical Review: Sleep Bruxism, Headaches, and Sleep-Disordered Breathing in Children and AdolescentsJulio AbarzuaPas encore d'évaluation
- Sajnani, 2015Document8 pagesSajnani, 2015Julio AbarzuaPas encore d'évaluation
- Sajnani, 2015Document8 pagesSajnani, 2015Julio AbarzuaPas encore d'évaluation
- Sajnani, 2015Document7 pagesSajnani, 2015Julio AbarzuaPas encore d'évaluation
- Björk Facial Growth in Man, Studied With The Aid of Metallic ImplantsDocument6 pagesBjörk Facial Growth in Man, Studied With The Aid of Metallic ImplantsNataly ComettaPas encore d'évaluation
- The Gerson TherapyDocument43 pagesThe Gerson Therapyboboacer100% (1)
- Andersson El Al%2ssssssc 2012Document8 pagesAndersson El Al%2ssssssc 2012Julio AbarzuaPas encore d'évaluation
- A Taste of Honey by Kai Ashante WilsonDocument97 pagesA Taste of Honey by Kai Ashante WilsonHyperion - ant.100% (1)
- Goblin Punch GLOG Alchemy and OozesDocument16 pagesGoblin Punch GLOG Alchemy and OozesAndré Angellis75% (4)
- Red Velvet - Psycho Lyrics PDFDocument6 pagesRed Velvet - Psycho Lyrics PDFErika MarasiganPas encore d'évaluation
- Nobody KnowsDocument3 pagesNobody KnowsIbanElTrolazoLalalaPas encore d'évaluation
- Business Partnership ProposalDocument2 pagesBusiness Partnership ProposalRico EduresePas encore d'évaluation
- Chitra Bharati Film Festival 2022: Rules & RegulationsDocument5 pagesChitra Bharati Film Festival 2022: Rules & RegulationsNavin ShashiPas encore d'évaluation
- Gastronomic ADocument194 pagesGastronomic Acecinestpasunpipe100% (1)
- Assignment in Business Communication: Brand 1: CleartripDocument3 pagesAssignment in Business Communication: Brand 1: CleartripPradeeba ChinnaduraiPas encore d'évaluation
- Edugain Rational NumbersDocument2 pagesEdugain Rational NumbersananditaPas encore d'évaluation
- BENZ, Walter (2012) - Classical Geometries in Modern ContextsDocument18 pagesBENZ, Walter (2012) - Classical Geometries in Modern ContextsanettlePas encore d'évaluation
- Week 8 - 1 and 8 - 2 Intellectual Property LawDocument49 pagesWeek 8 - 1 and 8 - 2 Intellectual Property LawBrowPas encore d'évaluation
- Behind Blue EyesDocument2 pagesBehind Blue EyesVictor Matos de OliveiraPas encore d'évaluation
- ZUNECA PHARMACEUTICAL v. NATRAPHARMDocument41 pagesZUNECA PHARMACEUTICAL v. NATRAPHARMFaustina del RosarioPas encore d'évaluation
- Pi Opadry CA Coat Param v2Document2 pagesPi Opadry CA Coat Param v2drantistPas encore d'évaluation
- Joyin v. Lin - Complaint Following Amazon DelistingDocument7 pagesJoyin v. Lin - Complaint Following Amazon DelistingSarah Burstein100% (1)
- Surmandal ManualDocument6 pagesSurmandal ManualAnonymous mJy4lhPas encore d'évaluation
- Ascap Copyright Lesson PlanshortDocument5 pagesAscap Copyright Lesson Planshortapi-259153530Pas encore d'évaluation
- Website Terms and Conditions - For Applicants - Band Baja Bide - 15112011Document4 pagesWebsite Terms and Conditions - For Applicants - Band Baja Bide - 15112011Priyanka GargPas encore d'évaluation
- 103HSLDocument4 pages103HSLRajesh BondgilwarPas encore d'évaluation
- Reinforced Concrete Mechanics Design SolDocument315 pagesReinforced Concrete Mechanics Design Solariani710Pas encore d'évaluation
- Dawson Group v. Miller - ACPA Complaint PDFDocument11 pagesDawson Group v. Miller - ACPA Complaint PDFMark JaffePas encore d'évaluation
- Financial Accounting Canadian 2nd Edition Waybright Solutions ManualDocument36 pagesFinancial Accounting Canadian 2nd Edition Waybright Solutions Manualkrossenflorrie355Pas encore d'évaluation
- Specifying Rock To Fill Gabions, Revet Mattresses, and Gabion MattressesDocument2 pagesSpecifying Rock To Fill Gabions, Revet Mattresses, and Gabion Mattressesgrats_singcoPas encore d'évaluation
- FrugalTO MagazineDocument28 pagesFrugalTO Magazinefrugalto100% (2)
- Loctite Ea 3478 - Carga MetalicaDocument3 pagesLoctite Ea 3478 - Carga Metalicafrancisca ferrerPas encore d'évaluation
- Volume 43, Issue 23, June 6, 2014Document112 pagesVolume 43, Issue 23, June 6, 2014BladePas encore d'évaluation
- Nikola Vs TeslaDocument29 pagesNikola Vs TeslaFred LamertPas encore d'évaluation
- Greyhound SystemDocument5 pagesGreyhound Systemhorace_hrc100% (1)
- Intra Moot-Plaintiff 1Document21 pagesIntra Moot-Plaintiff 1samidha hegdePas encore d'évaluation