Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- 19 - Lats & Upper BackDocument29 pages19 - Lats & Upper Backbreinfout fotos100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- 2016 Sadik Olympia Prep Combined PDFDocument47 pages2016 Sadik Olympia Prep Combined PDFAlexis V Xialongyu100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hypertrophy Execution Mastery - Module 1 Workouts - Chest BackDocument24 pagesHypertrophy Execution Mastery - Module 1 Workouts - Chest BackHarshit Singh100% (1)
- The McKenzie Method Powerpoint - 2008Document57 pagesThe McKenzie Method Powerpoint - 2008aslooclt100% (2)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Radiography of Forearm and Upper ArmDocument35 pagesRadiography of Forearm and Upper ArmsaurabhmhshwrPas encore d'évaluation
- Physiotherapy Care Protocol For Low Back PainDocument29 pagesPhysiotherapy Care Protocol For Low Back Painaliaarif75% (4)
- ANATOMYDocument9 pagesANATOMYAndrassy Twinkle AlineaPas encore d'évaluation
- Yoga PosesDocument25 pagesYoga PosesHoratiu Petrescu100% (1)
- Iron Cross: ProgramDocument16 pagesIron Cross: ProgramFlorian DutroncPas encore d'évaluation
- MCQ On AnatomyphysDocument59 pagesMCQ On AnatomyphysKiran Kalyanam0% (1)
- Partial Foot AmputationDocument38 pagesPartial Foot AmputationVandana SinghPas encore d'évaluation
- Tensegrity in Cadaveric StudyDocument5 pagesTensegrity in Cadaveric StudyJohn SharkeyPas encore d'évaluation
- Connective TissueDocument202 pagesConnective TissuePeter ThompsonPas encore d'évaluation
- Sanchez Sotelo2007Document10 pagesSanchez Sotelo2007Lucas LozaPas encore d'évaluation
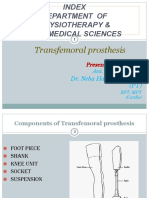
- TRANSFEMORAL - PPT 1Document64 pagesTRANSFEMORAL - PPT 1Farheen KhanPas encore d'évaluation
- Volkmann Ischaemia ContractureDocument4 pagesVolkmann Ischaemia ContractureAdre RefdianPas encore d'évaluation
- Normative Values For Isometric Muscle Force by Handheld DynamometerDocument14 pagesNormative Values For Isometric Muscle Force by Handheld DynamometerWasemBhatPas encore d'évaluation
- JOINS Keperawatan B 4Document5 pagesJOINS Keperawatan B 4Laila nurhafizahPas encore d'évaluation
- Compa Horse and Human - NervesDocument12 pagesCompa Horse and Human - NervesJames SumagaysayPas encore d'évaluation
- Dr. Yossi Maryanti, M.biomed, Sp. S - Neck and Back PainDocument50 pagesDr. Yossi Maryanti, M.biomed, Sp. S - Neck and Back PainFreade AkbarPas encore d'évaluation
- Flexibility in Spanish Elite Inline Hockey Players: Profile, Sex, Tightness and AsymmetryDocument14 pagesFlexibility in Spanish Elite Inline Hockey Players: Profile, Sex, Tightness and AsymmetryDaniela DaňováPas encore d'évaluation
- Journal of AMCDocument6 pagesJournal of AMCMarko SimonceliPas encore d'évaluation
- 5 Axillary and Epitrochlear Lymph Node Dissection For MelanomaDocument11 pages5 Axillary and Epitrochlear Lymph Node Dissection For MelanomajuanrangonePas encore d'évaluation
- Dry Needling Case Studies 1-5Document13 pagesDry Needling Case Studies 1-5munesh shrivastvaPas encore d'évaluation
- Return To Sport and Reinjury Rates in Elite Female Athletes After Anterior Cruciate Ligament RuptureDocument8 pagesReturn To Sport and Reinjury Rates in Elite Female Athletes After Anterior Cruciate Ligament RuptureFederico BristotPas encore d'évaluation
- Uts AnatomiDocument18 pagesUts AnatomiSuratmi UnnesPas encore d'évaluation
- Epidemiology of Lumbar Disc HerniationDocument4 pagesEpidemiology of Lumbar Disc HerniationPankaj VatsaPas encore d'évaluation
- PE L1 Common InjuriesDocument16 pagesPE L1 Common InjuriesAnjel Rhada Mae EstoestaPas encore d'évaluation
- Effect of Mcconnell Taping On Pain, Rom & Grip Strength in Patients With Triangular Fibrocartilage Complex InjuryDocument9 pagesEffect of Mcconnell Taping On Pain, Rom & Grip Strength in Patients With Triangular Fibrocartilage Complex InjuryDr. Krishna N. SharmaPas encore d'évaluation
- Sports and Performing Arts Medicine 2 LoDocument7 pagesSports and Performing Arts Medicine 2 LowladjaPas encore d'évaluation