Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Tenth House in AstrologyDocument6 pagesThe Tenth House in AstrologytratakPas encore d'évaluation
- Renault Gearbox and Final Drive OilsDocument10 pagesRenault Gearbox and Final Drive OilsPhat0% (1)
- Daniel Madison - BreachDocument8 pagesDaniel Madison - Breachmrbookman3Pas encore d'évaluation
- Cast Your HoroscopeDocument27 pagesCast Your HoroscopeSunil ShastriPas encore d'évaluation
- L 7 Thermal Death Time DataDocument21 pagesL 7 Thermal Death Time DataVaibhav GuptaPas encore d'évaluation
- Seismic Isolation For Buildings Catalog 2013 by Bridgestone Corp - Multi Rubber BearingDocument44 pagesSeismic Isolation For Buildings Catalog 2013 by Bridgestone Corp - Multi Rubber BearingitetejacPas encore d'évaluation
- Ok TC FlotationDocument4 pagesOk TC FlotationWilliam SalcedoPas encore d'évaluation
- System Substation Commissioning TestsDocument8 pagesSystem Substation Commissioning TestsCvijayakumar100% (1)
- BFD-180-570 DN65 GBDocument25 pagesBFD-180-570 DN65 GBalexander100% (3)
- SitasiDocument1 pageSitasiorriPas encore d'évaluation
- Family Planning Training Resource PackageDocument16 pagesFamily Planning Training Resource PackageorriPas encore d'évaluation
- Family Planning Training Resource PackageDocument16 pagesFamily Planning Training Resource PackageorriPas encore d'évaluation
- Family Planning Training Resource PackageDocument16 pagesFamily Planning Training Resource PackageorriPas encore d'évaluation
- Ariel-Kehamilan Remaja Yang Berakhibat KriminalitasDocument6 pagesAriel-Kehamilan Remaja Yang Berakhibat KriminalitasorriPas encore d'évaluation
- 5 WHO Medical Eligibility CriteriaDocument9 pages5 WHO Medical Eligibility CriteriaorriPas encore d'évaluation
- Acut Kidney InjuryDocument12 pagesAcut Kidney InjuryorriPas encore d'évaluation
- Hellp Syndrome DicDocument10 pagesHellp Syndrome Dicanne_kristiantiPas encore d'évaluation
- Infertility and Uterine F 2016 Best Practice Research Clinical ObstetricsDocument8 pagesInfertility and Uterine F 2016 Best Practice Research Clinical ObstetricsorriPas encore d'évaluation
- Difference Betwen Lyomioma and SarcomaDocument23 pagesDifference Betwen Lyomioma and SarcomaorriPas encore d'évaluation
- Malignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalDocument8 pagesMalignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalorriPas encore d'évaluation
- Smooth Muscle Tumor of UterusDocument12 pagesSmooth Muscle Tumor of UterusorriPas encore d'évaluation
- The Treatment of Post Hysterectomy Vaginal Vault ProlapseDocument17 pagesThe Treatment of Post Hysterectomy Vaginal Vault ProlapseorriPas encore d'évaluation
- Bookshelf NBK22183Document236 pagesBookshelf NBK22183orriPas encore d'évaluation
- Design and Modelling of Internal Permanent Magnet Motor (#764846) - 1189475Document25 pagesDesign and Modelling of Internal Permanent Magnet Motor (#764846) - 1189475Tejas PanchalPas encore d'évaluation
- Evolution of MISDocument4 pagesEvolution of MISHarshitha PadmashaliPas encore d'évaluation
- 017 - Chapter 3 - L13Document6 pages017 - Chapter 3 - L13nanduslns07Pas encore d'évaluation
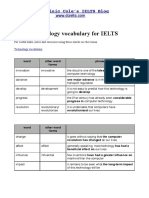
- Technology VocabularyDocument3 pagesTechnology VocabularyChixo GalaxyPas encore d'évaluation
- Trane 5 Ton HP Cond submittat4TWB3060-SUB-106 - 05.05 - 11012009Document2 pagesTrane 5 Ton HP Cond submittat4TWB3060-SUB-106 - 05.05 - 11012009nobleairPas encore d'évaluation
- Penerapan Metode Sonikasi Terhadap Adsorpsi FeIIIDocument6 pagesPenerapan Metode Sonikasi Terhadap Adsorpsi FeIIIappsPas encore d'évaluation
- What Is New in API 610 11th EdDocument6 pagesWhat Is New in API 610 11th EdAnonymous 1XHScfCIPas encore d'évaluation
- 1965 Elio R. Freni - Electrolytic Lead Refining in SardiniaDocument9 pages1965 Elio R. Freni - Electrolytic Lead Refining in SardiniaGeorgettaPas encore d'évaluation
- Reading Week 13Document6 pagesReading Week 13Quy PhanPas encore d'évaluation
- Blender To Google EarthDocument41 pagesBlender To Google Earthrichx7Pas encore d'évaluation
- Laura Gentile Letter On Hampden County CourthouseDocument6 pagesLaura Gentile Letter On Hampden County CourthouseMassLivePas encore d'évaluation
- MH2732-Robotics Lab ManualDocument50 pagesMH2732-Robotics Lab Manualramzi ayadiPas encore d'évaluation
- The Anaphylactic ShockDocument8 pagesThe Anaphylactic ShockRooby JeanpierrePas encore d'évaluation
- EN 301.908-2 Ver 3.2.1Document37 pagesEN 301.908-2 Ver 3.2.1DHDIDIDPas encore d'évaluation
- Research Paper On TurbojetDocument6 pagesResearch Paper On Turbojetqptwukrif100% (1)
- Atg SPRL 01 PDFDocument25 pagesAtg SPRL 01 PDFMuhammad Faiez AfzaalPas encore d'évaluation
- Nigeria Certificate in Education Science ProgrammeDocument215 pagesNigeria Certificate in Education Science Programmemuhammadbinali77_465Pas encore d'évaluation
- Turnitin Originality ReportDocument20 pagesTurnitin Originality ReportNaomi Deirdre ReyesPas encore d'évaluation
- BJT Common Emitter Characteristics: Experiment 6Document5 pagesBJT Common Emitter Characteristics: Experiment 6beesahPas encore d'évaluation
- Neo Neurophone Patrick FlanaganDocument2 pagesNeo Neurophone Patrick FlanaganalexanderjfernandesPas encore d'évaluation
- Polymer Structures: Issues To Address..Document34 pagesPolymer Structures: Issues To Address..Eugene Embalzado Jr.Pas encore d'évaluation