Académique Documents
Professionnel Documents
Culture Documents
HTA en Obesidad
Transféré par
Miriam ObregonCopyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
HTA en Obesidad
Transféré par
Miriam ObregonDroits d'auteur :
Formats disponibles
REVISIONES
Mecanismos de hipertensión en obesidad
Mechanisms of hypertension in obesity
C.M. López de Fez, M.T. Gaztelu, T. Rubio, A. Castaño
ABSTRACT
RESUMEN Obesity is a chronic disease, considered to be an
La obesidad es una enfermedad crónica, conside- important risk factor in the development of coronary
rada un factor de riesgo importante en el desarrollo de disease, hypertension, renal insufficiency and failure.
enfermedad coronaria, hipertensión, insuficiencia y Obesity contributes to hypertension by mecha-
fallo renal. nisms such as: insulinic resistance and hyperinsuli-
La obesidad contribuye a la hipertensión por naemia, increase of adrenergic activity and of concen-
mecanismos tales como: resistencia insulínica e hipe- trations of aldosterone, retention of sodium and water
rinsulinemia, aumento de la actividad adrenérgica y de and increase of cardiac wear, alteration of the endothe-
las concentraciones de aldosterona, retención de lial function, through molecules such as leptin and
sodio y agua e incremento del gasto cardíaco, altera- adiponectin and genetic factors. Many paths of
ción de la función endotelial, a través de moléculas research remain open.
como leptina y adiponectina y factores genéticos. Que- The angiotensin-converting-enzyme inhibitors
dan aún abiertas muchas vías de investigación. (ACEI) and/or the angiotensin II receptor antagonists
Los IECA y/o los ARA II son fármacos de primera (ARA II) are first choice medicines because of their
elección por su efecto beneficioso sobre la resistencia beneficial effect on insulinic resistance and sympathet-
insulínica y actividad simpática. ic activity.
Palabras clave. Hipertensión. Obesidad. Hiperin- Key words. Hypertension. Obesity. Hyperinsuli-
sulinemia. Sistema renina-angiotensina-aldosterona. naemia. Renin-angiotensin-aldosterone system. Leptin.
Leptina. Adiponectina. Adiponectin.
An. Sist. Sanit. Navar. 2004; 27 (2): 211-219.
Servicio de Medicina Interna. Hospital García Correspondencia:
Orcoyen. Estella (Navarra). Carmen Marina López de Fez
Aceptado para su publicación el 24 de marzo de Travesía de Acella 5, esc. izda, 3 A
2004. 31008 Pamplona
e-mail: trubiove@cfnavarra.es
An. Sist. Sanit. Navar. 2004, Vol. 27, Nº 2, mayo-agosto 211
C. M.. López de Fez et al
INTRODUCCIÓN DISTRIBUCIÓN DE LA GRASA
La obesidad es una enfermedad cróni-
CORPORAL
ca cuya prevalencia va en aumento por lo La obesidad localizada preferentemen-
que su prevención es un reto importante te en el hemicuerpo superior se asocia a
en salud pública. Se define como un exce- un aumento de morbi-mortalidad cardio-
so de peso corporal a expensas de acúmu- vascular y mayor incidencia de enfermeda-
lo de tejido adiposo1. Desde el punto de des tales como diabetes mellitus (DM),
vista antropométrico, la fórmula más HTA, dislipemia, patología de la vesícula
empleada es el índice de masa corporal biliar y neoplasias3-5.
(IMC), cociente entre el peso en kilogra-
Algunos investigadores encuentran
mos y la talla en metros al cuadrado. Un
que la prevalencia de HTA en obesidad es
valor superior a 30, es indicativo de obesi-
mayor de la que cabría esperar por el
dad. En la actualidad se considera el índice
incremento de IMC per se. Otros, sin
cintura cadera (ICC), más fiable que el IMC
embargo, describen cambios en la presión
para el cálculo del riesgo cardiovascular.
arterial similares según incremento de
Cuando es mayor de 1 en varones ó 0,88 en
IMC, grado de obesidad superior y niveles
mujeres, indica un aumento de este riesgo.
de insulina en ayunas6.
En el estudio Framingham, el 70% de los
casos de hipertensión (HTA) en el hombre
y 61% en mujeres, son atribuibles a exceso RESISTENCIA A LA
de adiposidad, con aumento promedio de INSULINA/HIPERINSULINEMA
presión sistólica de 4,5 mmHg por cada 5
kg de aumento de peso2. Los niveles de insulina sérica en
pacientes obesos, hipertensos o no, son
La relación de la HTA con factores mayores frente a individuos sanos y se
ambientales y sociales, así como mecanis- asocia a cambios en el metabolismo de las
mos endocrinos, genéticos y metabólicos grasas7. La obesidad en el hemicuerpo
es manifiesta3. Éstos son: distribución de la superior se relaciona con concentraciones
grasa corporal, resistencia a la insulina e de insulina altas en ayunas y tras la admi-
hiperinsulinemia, activación simpática, nistración de glucosa, y con aumento en la
efectos renales debido al aumento de las incidencia de DM tipo 2. Ello se debe a la
concentraciones de aldosterona por acumulación de células abdominales lipolí-
mayor actividad del sistema renina-angio- ticas hiperactivas que liberan cantidades
tensina-aldosterona (RAAS), retención de de ácidos grasos libres hacia la vena porta,
sodio, expansión volumétrica con aumen- incrementando la síntesis de triglicéridos
to de resistencia vascular periférica debi- e inhibiendo la captación de insulina, con
do a alteraciones en la vasodilatación, con- aparición de resistencia a la insulina e
centraciones de leptina y adiponectina, hiperinsulinemia7. Son varios los niveles
factores hemodinámicos y predisposición de actuación sobre la presión arterial7-19
genética. (Tabla 1). Entre otros se incluyen:
Tabla 1. Mecanismos propuestos por los que la resistencia insulínica y/o la hiperinulinemia inducen
aumento de la PA*.
Mecanismo Efecto
Aumento de la reabsorción renal de Na y agua. Mayor sensibilidad de la PA a la ingesta dietética de
sal.
Aumento de las respuestas presoras y de aldosterona Alteración del transporte de membrana de
a la angiotensina II. electrolitos.
Mayor acumulación intracelular de calcio. Estimulación de los factores crecimiento (m.
esquelético).
Estimulación de la actividad nerviosa simpática. Menor síntesis de PG vasodilatadoras.
Alteración en vasodilatación. Secreción de endotelina.
*La resistencia a la insulina puede ser responsable, al menos en parte, de la alteración en la excreción de (Na) que se observa en las per-
sonas obesas: aumenta el sodio intracelular y produce hipovolemia, actuando a nivel de dos bombas, la ATPasa Na-K, y el antiporter Na-H+.
212 An. Sist. Sanit. Navar. 2004, Vol. 27, Nº 2, mayo-agosto
MECANISMOS DE HIPERTENSIÓN EN OBESIDAD
Efecto estimulador del simpático. La (HVI) y contribuye a la génesis de arrit-
inyección de dosis progresivamente mayo- mias ventriculares y, con ello, muerte súbi-
res de insulina provoca un incremento ta.
dosis-dependiente de los niveles de nore- La acción vasoconstrictora del SNS en
pinefrina (NE) circulante con aumento de vasos de músculo esquelético reduce la
la frecuencia cardiaca y la presión arterial. absorción de glucosa por el músculo, favo-
Otra hipótesis recaería sobre una situa- reciendo la resistencia insulínica e hiperin-
ción de resistencia insulínica localizada sulinemia3,20,21.
básicamente a nivel del músculo estriado,
que condicionaría, hipertrofia vascular vía La HTA surge de las interacciones de, al
receptor a y un aumento de la conversión menos, cuatro mecanismos, siendo el más
de fibras musculares hacia tipo 2b, las cua- obvio, la activación del SNS22 (Fig. 2). Sin
les muestran un mayor nivel de resistencia embargo, la hiperactividad simpática no
insulínica, perpetuándose así el daño sólo obedece a la hiperinsulinemia induci-
sobre las resistencias periféricas (Fig. 1). da por obesidad, sino también a un efecto
directo de la mayor ingesta calórica. En
Efecto retenedor de NA a nivel renal. pacientes obesos normotensos, el tono
Disminuye la excreción de Na. simpático renal está aumentado al doble
Alteraciones sobre metabolismo lipí- pero los niveles de NE corresponden al
dico. Aumento de VLDL, colesterol total y 50% del normal. Por otro lado, en pacien-
triglicéridos con disminución de HDL. tes obesos e hipertensos existe un aumen-
to de NE en riñón, con niveles en corazón
Efecto en el transportador catiónico doble respecto a los de un paciente obeso
de membrana. Estimulación de la bomba normotenso y 25% mayor a los de un
Na+/H+, disminución de la actividad Na/K voluntario sano. La actividad simpática
ATPasa y del intercambiador Na+/Ca2+ con muscular en individuos obesos es mayor
aumento de Ca2+ intracelular. sean o no hipertensos22,23, de lo que se
Efectos en pared vascular. Incrementa deduce que es condición necesaria pero
resistencias periféricas. no suficiente. La clave está en la capacidad
adaptativa del SNS a nivel cardíaco. Por
otro lado, la insulina en individuos con
SISTEMA NERVIOSO SIMPÁTICO normopeso induce vasodilatación en el
El aumento de la actividad simpática es músculo esquelético, sin embargo, en obe-
un mecanismo de inicio y mantenimiento sos hay escasa respuesta del flujo sanguí-
de la presión arterial. De hecho, la activi- neo a la insulina, debido en parte, a una
dad del sistema nervioso simpático (SNS) mayor sensibilidad presora a la noradrena-
produce hipertrofia ventricular izquierda lina17.
OBESIDAD
Resistencia insulínica Hiperactividad simpática
Retención de Na
Aumento del gasto cardiaco
HIPERTENSIÓN
Figura 1. Esquema sencillo de mecanismo de aparición de HTA en obesidad.
An. Sist. Sanit. Navar. 2004, Vol. 27, Nº 2, mayo-agosto 213
C. M.. López de Fez et al
Obesidad, diabetes Disfunción diastólica
Hipertensión HVI ICC Muerte
Dislipemia, tabaco Disfunción sistólica
Figura 2. Mecanismos productores de HTA.
RAAS: incremento de las concentra- dora a los estimulantes del NO, pudiendo
ciones séricas de aldosterona deberse a una reducción en su síntesis26-28,
El RAAS es un determinante el tono del sin estar relacionado en exclusiva a una
glomérulo renal eferente y de la reabsor- menor disponibilidad de sustrato29, debido
ción tubular de Na, participando de efec- a una mayor descomposición del NO por
tos vasoconstrictores y de la homeostasis superóxido30 o por la inhibición por sus-
del volumen líquido extracelular. La obesi- tancias ciclooxigenasa dependientes31.
dad se asocia a un aumento de los niveles
de aldosterona y alteración de la relación SENSIBILIDAD AL SODIO Y
angiotensina II- aldosterona, con mayor VOLUMEN PLASMÁTICO1,2
actividad del RAAS3, aumentando la canti-
Los mecanismos a través de los cuales
dad corporal de Na y agua, y por tanto
se origina la retención de Na podrían estar
favoreciendo el aumento de la PA en obe-
en relación con los efectos combinados de
sos. Las concentraciones de renina dismi-
la resistencia insulínica con mayor o
nuyen progresivamente con la obesidad, e
menor grado de hiperinsulinismo8 y con la
inversamente, las concentraciones de
hiperactividad simpática. El aumento de
aldosterona en obesos son mayores que en
calcio intracelular en las células muscula-
no obesos.
res lisas por disminución de la ATPasa Na-
Estudios realizados con el fin de inves- K, puede dar lugar a HTA, al inducir incre-
tigar la relación entre variantes genéticas mento del tono muscular y la resistencia
de la enzima convertidora de angiotensina periférica. Algunos investigadores señalan
con la PA y con la estructura y función del que existe una excreción de Na normal o
ventrículo izquierdo (VI) en jóvenes obe- ligeramente elevada en individuos obesos
sos, objetivaron que los pacientes homoci- relacionándola con la HTA asociada a la
gotos para el alelo D presentan un riesgo obesidad32.
mayor de desarrollar HTA, alteración
estructural y disfunción VI; por lo que
LEPTINA
deben ser considerados como candidatos
de padecer enfermedad cardiovascular24. Es una hormona de 167 aminoácidos
secretada por los adipocitos33. Se introdu-
ce en los fluidos cerebroespinales por
EFECTOS DE HIPERTENSIÓN Y
endocitosis, uniéndose al receptor especí-
OBESIDAD EN LA FUNCIÓN DEL fico hipotálamico (Ob-R), activando neuro-
ENDOTELIO péptidos, provocando pérdida de apetito,
La obesidad y la HTA se asocian a dis- disminuyendo el tejido graso y el peso del
función endotelial. El óxido nítrico (NO) es individuo3,33-35. El nivel de leptina en indivi-
el vasodilatador endógeno más potente. duos normales se encuentra entre 5-15
Interviene en la regulación del tono vascu- µg/ml, siendo mayor en obesos.
lar, inhibición de la agregación y adhesión El gen Ob-R controla la expresión de
plaquetar e inhibe la proliferación de célu- varias alternativas. El Ob-Rb es el receptor
las musculares25. mayor, con un dominio transmembrana y
Estudios llevados a cabo en pacientes otro intracelular con radical carboxilo. Los
hipertensos, han mostrado que presenta Ob-Ra, Ob-Rc y Ob-Rd son receptores pre-
una alteración de la respuesta vasodilata- maturos con un corto tallo intracelular que
214 An. Sist. Sanit. Navar. 2004, Vol. 27, Nº 2, mayo-agosto
MECANISMOS DE HIPERTENSIÓN EN OBESIDAD
facilitan el paso de leptina al cerebro. El nuyendo la expresión de moléculas de
Ob-Re es un receptor proteico que carece adhesión (VCAM-1, ICAM-1, E-selectina,
de dominio transmembrana y se comporta etc.). Sus niveles son menores en pacien-
como receptor soluble que se une e inacti- tes obesos que en no obesos, en hombres
va la leptina circulante. que en mujeres y mayores en pacientes
con enfermedad coronaria y DM tipo 2. La
La leptina actúa a diferentes niveles en reducción de peso en pacientes obesos se
el sistema cardiovascular y renal, aumen- sigue de un aumento de la concentración
tando la descarga simpática, insulino-resis- de adiponectina. Existe una relación inver-
tencia y la excreción de sodio y agua2,3,19. sa entre niveles de esta proteína y la ten-
Son contradictorios los resultados obteni- sión arterial y también en términos de fil-
dos de la relación que puede existir entre trado glomerular. El mecanismo por el cual
leptina-obesidad y leptina-insulinemia. En se produce descenso de adiponectina es
estudios con animales experimentales desconocido. Una explicación podría ser el
obesos se observan concentraciones bajas aumento de la actividad del SNS. Existe
de leptina y de sus receptores. En huma- también relación inversa con niveles de tri-
nos, el déficit de leptina sería, con más glicéridos y con la aparición DM tipo 2. En
probabilidad, secundario a una alteración la resistencia insulínica y en la patogénesis
en su receptor33,36. Además, tiene un efecto de la arteriosclerosis se evidencia un des-
estimulador en la secreción de gonadotro- censo de sus niveles38-42.
pinas e insulina, y tanto la hiperinsuline-
mia como los glucocorticoides poseen, a
su vez, un efecto estimulador de la secre- FACTORES HEMODINÁMICOS
ción de leptina. Para conocer el papel de la En los individuos obesos, el gasto car-
leptina en los mecanismos que nos ocu- díaco, la volemia central y total y el volu-
pan, algunos estudios centran la relación men sistólico son mayores que en no obe-
entre presión arterial, IMC, actividad de sos41. El gasto cardíaco es proporcional al
SNS, resistencia insulínica y leptina. Se incremento de la masa corporal y puede
objetiva una interacción diferente depen- ser razón principal de aumento de PA32. Por
diendo del sexo: la leptina y la resistencia otro lado, en los pacientes obesos, nos
insulínica producen un aumento de la TA encontramos con un estado protrombóti-
por aumento de actividad del SNS en muje- co, secundario al estasis venoso y dismi-
res, pero no así en hombres37. Sin embargo, nución de la actividad física entre otros,
otros han propuesto que no existe tal rela- que contribuye al aumento de la PA.
ción. Para complicar más esta relación, la
administración de leptina produce dos FACTORES GENÉTICOS
efectos distintos: a largo plazo puede
incrementar la actividad simpática con Esta consideración se deriva del hecho
efectos vasopresores, mientras que la de que la obesidad central-superior se
administración directa en las arterias rena- debe en parte a una predisposición genéti-
les puede inducir natriuresis con retención ca, y que en gemelos adultos existe una
de Na y por tanto, efecto antivasopresor3. concordancia en cuanto a HTA, DM y obe-
Son necesarios más estudios para eviden- sidad. Sin embargo, no siempre se eviden-
ciar el papel que desempeña la leptina en cia HTA en la obesidad, por lo que deben
la HTA. existir estos factores genéticos33,43-45. Ante-
cedentes familiares de HTA y obesidad son
factores de riesgo de HTA.
ADIPONECTINA
El TGF-b, codificado genéticamente, es
Actualmente, crece la evidencia de que una citoquina multifuncional que regula el
el tejido adiposo per se es un órgano endo- crecimiento, la diferenciación y la produc-
crino que secreta sustancias biológica- ción de matriz celular43. Se segrega por
mente activas. La adiponectina es una pro- monocitos, células endoteliales y muscula-
teína de reciente descubrimiento secreta- res de la pared del vaso. Se asocia a otras
da por este tejido. Inhibe en la forma ini- patologías como cáncer, aterosclerosis y
cial las lesiones arterioscleróticas, dismi- enfermedades fibróticas. En pacientes
An. Sist. Sanit. Navar. 2004, Vol. 27, Nº 2, mayo-agosto 215
C. M.. López de Fez et al
hipertensos, se ha demostrado un aumen- Daño renal
to de dicha proteína. Más aún, los niveles Los riñones del obeso están cubiertos
de esta proteína son mayores en pacientes por una capa de grasa que penetra en el
hipertensos con aumento de IMC, frente a hilio renal rodeando la médula3, originando
IMC normal. Pueden influir en la expresión un aumento del depósito de células inters-
de TGF-β los polimorfismos en DNA TGF-b1 ticiales y de la matriz extracelular entre los
y la actividad de angiotensina-II siendo un túbulos, que induce un aumento de la pre-
mediador del daño producido por esta en sión hidrostática intersticial y de la reab-
la HTA. Algunos científicos incluyen que sorción tubular de Na. Las consecuencias
existe asociación con las consecuencias a son un aumento de flujo renal, filtrado glo-
largo plazo de HTA, como son la HVI, el merular (FG) y albuminuria, con posibili-
remodelado vascular y la enfermedad dad de daño renal.
renal. Existe relación entre leptina y TGF-
b1, ya que se ha demostrado que la leptina
estimula la expresión por células del glo- TRATAMIENTO DEL OBESO
mérulo renal de TGF-β1 y los receptores HIPERTENSO
tipo II en el mesangio. Es fácil asumir, que una corrección del
sobrepeso, será beneficioso en la reduc-
Sistema cardiovascular ción de cifras de tensión arterial. Para ello
existen medidas no farmacológicas y far-
Varios estudios relacionan la obesidad
macológicas.
con insulino y leptino resistencia, que
supone una inhibición de la actividad del
péptido natriurético, retención de Na, Medidas no farmacológicas
expansión de volumen cardio-pulmonar y Son medidas no farmacológicas: dieta
del gasto cardíaco. Se producen cambios baja en grasa, pobre en sal, moderada en
en el metabolismo de cationes con la con- hidratos de carbono y rica en fibra; ejerci-
siguiente adaptación del corazón mediante cio aeróbico y disminución de ingesta de
HVI concéntrica-excéntrica46 (Fig. 3). alcohol, entre otras.
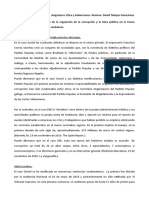
Aumento de la Liberación de
Obesidad+Andrógenos Grasa abdominal ácidos grasos libres
DIABETES
MELLITUS RP a insulina Aumento de la Menor extracción
TIPO 2 secreción insulínica hepática
pancreática de insulina
HIPERINSULINEMIA
Hiperactividad Retención Hipertrofia
Nerviosa de sodio vascular
Simpática
Vasodilatación atenuada HIPERTENSIÓN
Figura 3. Hipertensión y fallo cardiaco.
216 An. Sist. Sanit. Navar. 2004, Vol. 27, Nº 2, mayo-agosto
MECANISMOS DE HIPERTENSIÓN EN OBESIDAD
Medidas farmacológicas ca y concentraciones de aldosterona,
Desde la introducción de los inhibido- retención de sodio y de agua. Existe un
res de la enzima de conversión de la angio- incremento del gasto cardiaco, con res-
tensina (IECA)47 en el tratamiento antihi- puesta de hipertrofia excéntrica-concéntri-
pertensivo se pudo observar un efecto ca, por parte del ventrículo, que predispo-
potenciado en la terapéutica hipogluce- nen a fallo cardiaco. La afectación renal
miante. Además, los IECA tienen un efecto puede desarrollar glomeruloesclerosis y
bloqueante de la actividad simpática, y fallo renal.
por supuesto, de la generación de angio- La pérdida ponderal se asocia con una
tensina II, con la consiguiente vasodilata- caída de presión arterial, tanto en normo-
ción que condiciona, sobre todo a nivel de tensos como en hipertensos. En los obesos
músculo estriado, efectos positivos sobre hipertensos, la presión empieza a descen-
la utilización de la glucosa. Los antagonis- der antes de obtener el peso ideal.
tas de receptores de angiotensina II, han Los IECA y/o los ARA II son fármacos de
demostrado igualmente ser fármacos efi- primera elección por su efecto beneficioso
caces en el control de la HTA en estos sobre la resistencia insulínica y actividad
pacientes, al inhibir el eje RAAS a diferen- simpática.
tes niveles. De hecho, estudios recientes,
aconsejan su uso combinado.
BIBLIOGRAFÍA
Otros fármacos utilizados en el trata- 1. Organización Mundial de la Salud (WHO
miento de la HTA del paciente obeso, son Report, 1998).
los diuréticos, betabloqueantes, alfablo- 2. ZHANG R, REISIN E. Obesity-hypertension: the
queantes y calcioantagonistas. Los diuréti- effects on cardiovascular and renal system.
cos, especialmente tiazidas, son fármacos Am J Hypertens 2000; 13: 1308-1314.
principalmente prescritos para el control 3. KANNEL WD, ANDERSON K, WILSON PWF. Secular
de los edemas y clínica asociada de insufi- blood pressure trends in normotensive per-
ciencia cardiaca. Los betabloqueantes, dis- sons: the Framingham study. Am Heart J
minuyen la frecuencia cardiaca y el gasto 1993; 125: 1154-1158.
miocárdico, por lo que son fármacos que 4. MARTINS D, TAREEN N, PAN D, NORRIS K. The
pueden utilizarse en enfermos selecciona- relationship between body mass index and
dos. Sin embargo, dados sus efectos cola- pulse pressure in older adults with isolated
terales y la existencia de otras patologías systolic hypertension. Am J Hypertens 2002;
asociadas (EPOC, diabetes…) en estos 15: 538-543.
pacientes, su uso queda en segundo plano. 5. POULIOT MC, DÉPRES J-P, LEMIEUX S, MOORJANI S,
Los alfabloqueantes son utilizados en TREMBLAY A, NADEAU A et al. Wiast circunfer-
pacientes varones con problemas prostáti- ence and abdominal sagital diameter: best
cos. Los calcioantagonistas son útiles en simple anthropometric indexes of abdomi-
pacientes de edad avanzada. Todos estos nal visceral adipose tissue accumulation and
fármacos, en la práctica habitual, son utili- related cardiovascular risk in men and
women. Am J Cardiol 1994; 73: 46-468.
zados en combinación.
6. SCHMIDT MI, WATSON RL, DUNCAN BB, METCLAF P,
BRANCATI FL, SHARRETT AR et al. Clustering of
CONCLUSIONES dyslipemia, hyperuricemia, diabetes, and
Se han expuesto los posibles mecanis- hyertension and its association with fasting
mos de HTA en obesidad conocidos en la insulin and central overall obesity in a gen-
actualidad, dejando puertas abiertas a eral population. Metabolism 1996: 45: 699-
706.
nuevas investigaciones. Se asume de
manera general que la obesidad juega un 7. VERA O, VELASCO M, CARBALLO J, FLORES E,
importante papel en la patogénesis de la ESPINOZA M, DE LA PARTE M et al. Insulinemia:
relationship with obesity and high blood
HTA. pressure. Am J Hypertens 2002; 15: A187.
Los mecanismos fisiopatológicos rela- 8. LANSBERG L. Diet, obesity and hypertension:
cionados con la HTA inducida por la obesi- A hypothesis involving insulin, the sympa-
dad son: resistencia insulínica, hiperinsuli- thetic nervous system, and adaptative ther-
nemia, aumento de la actividad adrenérgi- mogenesis. Q J Med 1986; 61: 1081-1090.
An. Sist. Sanit. Navar. 2004, Vol. 27, Nº 2, mayo-agosto 217
C. M.. López de Fez et al
9. GUPTA AK, CLARK RV, KIRCHNER KA. Effects of 22. GRASSI G, SERAVALLE G, CATTANEO BM, BOLLA GB,
insulin on renal sodium excretion. Hyperten- LANFRANCHI A, COLOMBO M et al. Sympathetic
sion 1992; 19 (Suppl 1): 178-182. activation in obese normotensive subjects.
Hypertension 1995; 25: 560-563.
10. SHARMA AM, SCHORR U, DISTLER A. Insulin resis-
tance in young salt-sensitive normotensive 23. AGAPITOV A, CORREIA M, SURKEY C, BRENZ T,
subjects. Hypertension 1993; 25: 384-390. HAYNES W. Sympathetic control of vascular
tone in obese humans. Am J Hypertens 2001;
11. ROCCHINI AP, MOOREHEAD C, DEREMER S, GOOD- 14 (Suppl 1): A23.
FRIEND TL BALL DL. Hyperinsulinemia and the
aldosterona and pressor responses to 24. DI CHIARA T, DURO G, PARRINELLO G, PATERNA S,
angiotensina II. Hypertension 1990; 15: 861- DI FIORE R, SEAGLIONE R et al. Angiotensin con-
866. verting enzyme gene polymorphisme and
central obesity: relationship with blood
12. BARBAGALLO M, GUPTA RK, RESNICK L. Indepen- pressure and left ventricular structure and
dent effects of hiperinsulinemia and hyper- function. Am J Hypertens 2001; 14 (Suppl 1):
glycemia on intracellular sodium in normal A163.
human red cell. Am J Hypertens 1993, 6: 264-
267. 25. FHIGASHI Y, SASAKI S, NAKGAWA K, MATSUURA H,
CHAYAMA K, OSHIMA T. Effect of obesity on
13. PONTREMOLI R, ZAVARONI I, MAZZA S, BATTEZZATI endothelium-dependent, nitric oxide-mediat-
M, MASSARINO F, TIXIANELLO A et al. Changes in ed vasodilation in normotensive individuals
blood pressure, plasma trygliceride and and patients with essential hypertension.
aldosterone concentration, and red cell Am J Hypertens 2001; 14: 1038-1045.
cation concentration in patients with
26. REES DD, PALMER RMJ, MONCDA S. Role of
hiperinsulinemia. Am J Hypertens 1991; 4;
endothelium-derived nitric oxide in the regu-
159-163.
lation of blood pressure. Proct Natl Acad Sci
14. AVIV A. The role of Ca2+, protein kinase and USA 1989; 86: 3375-3378.
the Na+H+ antiporter in the development of 27. CALVER A, COLLIER J, GREEN D, VALLANCE P. Effect
hypertension and insulin resitance. J Am Soc of acute plasma volume expansion on
Nephol 193; 3: 1049-1063. peripheral arteriolar tone in healthy sub-
15. BORNFELDT KE, ARNQUIST HJ, CAPRON L. In vivo jects. Clin Sci 192; 85: 541-547.
proliferation of rat vascular smooth muscle 28. KELM M, PREIK M, HAFNER DJ, STRAUER BE. Evi-
in relation to diabetes mellitus insulin-like dence for multifactorial process involved in
growthfactor I and insulin. Diabetologia the impaired flow responses of nitric oxide
1992; 35: 104-108. in the hypertensive patients with endothelial
16. LEMBO G, NAPOLI R, CAPALDO B, RENDINA V, IAC- dysfunction. Hypertension 1996; 27: 346-353.
CARINO V, VOLPE M et al. Abnormal sympathet- 29. PANZA JA, CASINO PR, BADAN DM, QUYYUMI AA.
ic overactivity aevoked by insulin in the Effect of increased availability of endotheli-
skeletal of patients with essential hyperten- um derived nitric oxide precursor on
sion. J Clin Invest 1992; 29: 111-114. endothelium-dependent vascular relaxation
in normal subjects and in patients with
17. AXEROL L. Insulin, prostaglandins, and the
essential hypertension. Circulation 1993; 87:
patoghenesis of hyertension. Diabetes 1991;
1475-1481.
40: 1223-1227.
30. TSCHUDI MR, MESAROS S, LUSCHER TF, MALINSKI T.
18. BARON AD, BRECHTEL-HOOK G, JOHNSON A, Direct in situ mesasurement of nitric oxid in
FINEBERG N, HENRY DP, STEINBERG HO. Interac- mesenteric resistance arteries. Increased
tions between insulin and norepinephrine on decomposition by superoxide in hyperten-
blood pressure and insulin sensitiviy. J Clin sion. Hypertension 1996; 27: 32-35.
Invest 1994: 93: 2453-2462.
31. TADDEI S, VIRDIS A, GHIADONI L, MAGAGNA A, SAL-
19. HU RM, LEVIN ER, PEDRAM A, FRANK HJL. Insulin VETTI A. Cyclooxygenase inhibition restores
stimulates production and secretion of nitric oxide activity in essential hyperten-
endothelium from bovine endothelial cells. sion. Hypertension 1997; 29: 274-279.
Diabetes 1993; 42: 351-358.
32. HALL J, BRANDS M, DIXON W, SMITH MJ. Obesity-
20. ESLER M. The sympathetic system and induced hypertension: renal function and
hipertensión. Am J Hypertens 2000; 13: S99- system hemodynamic. Hypertension 1993,
105. 22: 292-299.
21. ESLER M. Sympatheic nervus system and 33. RÖNNEMAA M, KARONEN S-L, RISSANEN A, KOSKEN-
insulin resistance: from obesity to diabetes. VUO M, KOIVISTO VA. Relation between plasma
Am J hypertens 2001; 14: A264. leptin levels and measures of body fat in
218 An. Sist. Sanit. Navar. 2004, Vol. 27, Nº 2, mayo-agosto
MECANISMOS DE HIPERTENSIÓN EN OBESIDAD
identical twins discordant for obesity. Am 41. OREN S, GROSSMAN E, FROHLICH ED. Arterial and
Intern Med 1995; 126: 26-31. venous compliance in obese and nonobese
34. KAZUSHI T, ICHIRO N. Leptin and membrane flu- subjects. Am J Cardiol 1996; 77: 665-667.
idity of erythrocytes in essential hyperten- 42. HATTORI Y, SUZUKI M, HATTORI S, KASAI K. Globu-
sion: an electron paramagnetic resonance lar adiponectin upregulates nitric oxide pro-
investigation. Am J Hypertens 2004; 17: 375- duction in vascular endothelia. Diabet 2003;
379. 46: 1543-1549.
35. XUEQUIN J, NOBORU F, JINZI S, HIROTO T, YIMU L,
43. CARMELLI D, CARDON L, FABSITZ R. Clustering of
KATSUO K et al. Effects of leptin on endothelial
hypertension, diabetes, and obesity in adult
function with Ob-Rb gene transfer in Zucker
male twins: same genes or same environ-
fatty. Atherosclerosis 2003; 169: 225-233.
ments. Am J Hum Genet 1994; 55: 566-573.
36. PANKOV IUA. Are all animal and human organs
and tissues endocrine in nature and are 44. PORRECA E, DI FEBBO C, VITACOLONNA E, BAC-
secreting peptide hormones into blood? CANTE G, DI CASTELNUOVO A, ANGELINI A et al.
Vopr Med Khim 1996; 42: 179-184. Transforming growth factor-B1 levels in
hypertensive patients: Association with
37. YAMAKADO M, ISHIZAKA Y, TAKAHASHI E. Clinical body mass index and leptin. Am J Hypertens
study on the role of leptin and insulin resis- 2002; 15: 759-765.
tanse in the pathogenesis of obesity related
hypertension. Am J Hypertens 2001; 14: 45. RICQUIER D. Genetic and molecular aspects of
A222. obesity: recent data. Pathol Biol 1999; 47:
1080-1084.
38. ADAMCZAC M, WICET A, FUNASHSASHI T, CHUDEK J,
KOKOT F, MATSUZAWA Y. Decreased plasma 46. TASIC I, LOVIC B, ILIC S, DJORRDEJEVIC D, LOVIC D,
adiponectin in patients with essential hyper- MILADINOVIC TN. Relationship between obesi-
tension. Am J Hypertens 2003; 16: 72-75. ty decrease and regresion of hypertensive
39. SOWERA JR. Obesity as a cardiovascular risk left ventricular hypertrophy. Am J Hypertens
factor. Am J Med 2003; 115 (Suppl 8): 37S-41S. 2002; 15 (Suppl 1): A198.
40. MURAKAMI H, URA N, FURUHASHI M, HIGASHIURA K, 47. AMADOR N, GUIZAR JM, MALACARA JM, PÉREZ-
MIURA T, SHIMAMOTO K. Role of adiponectin in LUQUE E, PANIAGUA R. Sympathetic activity and
insulin-resistant hypertension and response to ACE inhibitor (enalapril) in nor-
artherosclerosis. Hypertens Res 2003, 26: motensive obese and non-obese subjects.
705-710. Arch M Research 2004; 35: 54-58.
An. Sist. Sanit. Navar. 2004, Vol. 27, Nº 2, mayo-agosto 219
Vous aimerez peut-être aussi
- Doctrina Queja+36-2013 PDFDocument3 pagesDoctrina Queja+36-2013 PDFMARIO SANCHEZ MIRANDA100% (1)
- Atento 2018Document118 pagesAtento 2018Alex QuintePas encore d'évaluation
- Ley de GaussDocument4 pagesLey de GaussViictor Manuelle MiierPas encore d'évaluation
- Estructura MisaDocument3 pagesEstructura MisaJM CuevasPas encore d'évaluation
- PHP Con MysqlDocument21 pagesPHP Con MysqlAndrés MarroquínPas encore d'évaluation
- ¿Cómo Se Extrae El Oro?Document5 pages¿Cómo Se Extrae El Oro?Katya Marcela Herrera MuñozPas encore d'évaluation
- Mezclas Racemicas (Expo) )Document11 pagesMezclas Racemicas (Expo) )CRISYAISAL50% (2)
- Curso - ELECTIVADocument3 pagesCurso - ELECTIVAMilton Alejandro CRUZ SANCHEZPas encore d'évaluation
- Concepto e Importancia de La GeotecniaDocument2 pagesConcepto e Importancia de La Geotecniaintelligent solutions100% (1)
- Trinidad de DiosDocument2 pagesTrinidad de DiosEbed A. Mamani ChPas encore d'évaluation
- Germanica Nueva MedicinaDocument11 pagesGermanica Nueva Medicinafelipe4alfaro4salas100% (1)
- Tejido Oseo HistologiaDocument18 pagesTejido Oseo HistologiaRodolfo Diaz100% (3)
- Acuiculturatilapiaruralperiurbana PDFDocument73 pagesAcuiculturatilapiaruralperiurbana PDFドイツ語 ブラウリオPas encore d'évaluation
- Estudio Monografico - ApaDocument9 pagesEstudio Monografico - ApaJaime Valdiviezo MarceloPas encore d'évaluation
- En Busca Del AmorDocument2 pagesEn Busca Del AmorCarlos Herbas CoaquiraPas encore d'évaluation
- Planificación de Entrenamiento para Francisca ContrerasDocument3 pagesPlanificación de Entrenamiento para Francisca ContrerasFrancisca Contreras MuñozPas encore d'évaluation
- Proyecto Sobre Educación y Nuevas TecnologíasDocument6 pagesProyecto Sobre Educación y Nuevas TecnologíasSergio NuñezPas encore d'évaluation
- Soldadura Por ArcoDocument6 pagesSoldadura Por ArcoLuis GuerreroPas encore d'évaluation
- Justificacion Tecnica - Pintura en Muros....Document13 pagesJustificacion Tecnica - Pintura en Muros....Javier Enrique Diaz ChacinPas encore d'évaluation
- Claudia Mugica Zuñiga - A1u9 - DaDocument5 pagesClaudia Mugica Zuñiga - A1u9 - DaClaudia I. Mugica ZuñigaPas encore d'évaluation
- Visual Basic para ExcelDocument4 pagesVisual Basic para ExcelFernando Farfan SalazarPas encore d'évaluation
- DJ SolicitanteDocument2 pagesDJ SolicitanteRoyMinenAlanyaAshtoPas encore d'évaluation
- Factores de ProducciónDocument6 pagesFactores de Producciónjuancojc100% (1)
- Analisis ERE GURTELDocument3 pagesAnalisis ERE GURTELdavidtobPas encore d'évaluation
- Pollito Chicken - Ana Lydia VegaDocument3 pagesPollito Chicken - Ana Lydia VegaWENDY HERNANDEZ SANCHEZPas encore d'évaluation
- Ensayo Educacion No FormalDocument3 pagesEnsayo Educacion No Formaljovipre50% (2)
- ANGUSTIADocument14 pagesANGUSTIAMARIA GUTIERREZPas encore d'évaluation
- Memorial de Divorcio Ordinario (Gustavo)Document6 pagesMemorial de Divorcio Ordinario (Gustavo)gustavoochaetaPas encore d'évaluation
- PlaneaciónDocument1 pagePlaneaciónCA LRPas encore d'évaluation
- Solución Costos PredeterminadosDocument6 pagesSolución Costos PredeterminadosShaday MacedoPas encore d'évaluation