Vous aimerez peut-être aussi
- An Easy Guide To Head To Toe Assessment Vrtis 12 2008 Website PDFDocument6 pagesAn Easy Guide To Head To Toe Assessment Vrtis 12 2008 Website PDFBSN 2014Pas encore d'évaluation
- Screening Head To Toe Physical ExaminationDocument16 pagesScreening Head To Toe Physical ExaminationJay Mar Mendoza BabatePas encore d'évaluation
- Potential Complications Signs and SymptomsDocument2 pagesPotential Complications Signs and SymptomsJessica GomezPas encore d'évaluation
- C 13Document11 pagesC 13Jo100% (1)
- ACTIVE LEARNING TEMPLATE: System DisorderDocument1 pageACTIVE LEARNING TEMPLATE: System DisorderDeo FactuarPas encore d'évaluation
- Pre-op Evaluation SummaryDocument1 pagePre-op Evaluation Summarysabbo morsPas encore d'évaluation
- SBAR Communication Tool and Progress NoteDocument2 pagesSBAR Communication Tool and Progress Notejrj1111100% (1)
- PEDIATRIC ASSESSMENT OVERVIEWDocument2 pagesPEDIATRIC ASSESSMENT OVERVIEWAghnia Nafila100% (1)
- Intake and Output FORMDocument2 pagesIntake and Output FORMEduardPas encore d'évaluation
- CPRDocument1 pageCPRjanet roosevelt100% (1)
- 65-Year-Old Woman With Cough and FatigueDocument7 pages65-Year-Old Woman With Cough and Fatigue최인선100% (1)
- EAR First AidDocument4 pagesEAR First Aidr_lakshmi2722Pas encore d'évaluation
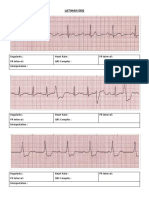
- Latihan Ekg KD A III 2016Document15 pagesLatihan Ekg KD A III 2016Syamsul PutraPas encore d'évaluation
- Mesenteric Ischemia in Dilated CardiomyopathyDocument30 pagesMesenteric Ischemia in Dilated CardiomyopathyJo AnnePas encore d'évaluation
- 1538 Exam 4 Cell Reg & GriefDocument35 pages1538 Exam 4 Cell Reg & GriefJade EdanoPas encore d'évaluation
- Preparation Worksheets For NUR 345 Heart Failure SimDocument14 pagesPreparation Worksheets For NUR 345 Heart Failure SimclarimerPas encore d'évaluation
- Body FluidsDocument6 pagesBody FluidsMemory MahwendaPas encore d'évaluation
- Fall Risk Assessment FormDocument3 pagesFall Risk Assessment FormMichael Silva100% (1)
- Charting Examples For Physical AssessmentDocument16 pagesCharting Examples For Physical Assessmentim3in1Pas encore d'évaluation
- Disorders of The Circulatory System Table-AnswersDocument2 pagesDisorders of The Circulatory System Table-Answersapi-281108263Pas encore d'évaluation
- Physical ExaminationDocument117 pagesPhysical Examinationsasmita nayakPas encore d'évaluation
- Pharmacology Main DrugsDocument14 pagesPharmacology Main DrugsSabir KhanPas encore d'évaluation
- West Visayas State University: Nursing ProcessDocument4 pagesWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- Nursing Clinical Prep SheetDocument1 pageNursing Clinical Prep SheetPatty Pasarilla PassehlPas encore d'évaluation
- AH2 Hesi ReviewDocument46 pagesAH2 Hesi ReviewJamie Antonini Grant100% (1)
- Brain 13Document1 pageBrain 13Nurse BettyPas encore d'évaluation
- Patient Assessment Marking SheetDocument2 pagesPatient Assessment Marking SheetJim Courtney100% (4)
- Abbreviations ListDocument6 pagesAbbreviations ListolivedaisychainPas encore d'évaluation
- Pathophysiology of AF in CHFDocument5 pagesPathophysiology of AF in CHFBimaIndraPas encore d'évaluation
- Concept Map Diagnosis and InterventionsDocument3 pagesConcept Map Diagnosis and Interventionsmenickel3Pas encore d'évaluation
- H&P OutlineDocument5 pagesH&P Outlineginadaislu100% (1)
- Assessheet 122Document2 pagesAssessheet 122Christine GoodpasterPas encore d'évaluation
- Gordons Case Pres 1Document5 pagesGordons Case Pres 1JM Asentista0% (1)
- Neonatal Assessmnt Tool PDFDocument2 pagesNeonatal Assessmnt Tool PDFYestin Reece Corpus ArcegaPas encore d'évaluation
- NCM 106 - Case Analysis - Nursing Care Plan of Heart FailureDocument2 pagesNCM 106 - Case Analysis - Nursing Care Plan of Heart FailureMarisol Jane JomayaPas encore d'évaluation
- Pediatric DKA: Section I: Scenario DemographicsDocument7 pagesPediatric DKA: Section I: Scenario DemographicsSugi DenyPas encore d'évaluation
- Head To Toe Physical Assessment: College of NursingDocument4 pagesHead To Toe Physical Assessment: College of NursingMaicah ShanePas encore d'évaluation
- Exam 3 Study Guide: Pain and Peripheral Vascular DiseaseDocument5 pagesExam 3 Study Guide: Pain and Peripheral Vascular DiseaseFarzanaAziziPas encore d'évaluation
- Condition Drug Class: Cardiovascular MedicationsDocument5 pagesCondition Drug Class: Cardiovascular MedicationsCasey Fioravante100% (1)
- Rapid Assessment SheetDocument5 pagesRapid Assessment SheetElise HowardPas encore d'évaluation
- Maste Med SheetDocument78 pagesMaste Med SheetBarbie Wiggers100% (1)
- Gastro MnemonicsDocument8 pagesGastro MnemonicsRufina SoomroPas encore d'évaluation
- Normal Adult Lab Values Blood GasesDocument1 pageNormal Adult Lab Values Blood Gasesmenickel3Pas encore d'évaluation
- Blank Physical Assessment SheetDocument2 pagesBlank Physical Assessment SheetRenee Hickman RobinsonPas encore d'évaluation
- Normal UA Results Chart With Nursing Considerations For AbnormalsDocument1 pageNormal UA Results Chart With Nursing Considerations For AbnormalsLinsey Bowen100% (1)
- Clinical Medication WorksheetDocument1 pageClinical Medication WorksheetSrkocher100% (1)
- CardiopathophysiologyDocument63 pagesCardiopathophysiologyapplesncorePas encore d'évaluation
- PATIENT 1 Nursing Assessment FormDocument5 pagesPATIENT 1 Nursing Assessment FormndembolovePas encore d'évaluation
- Basic EKG InterpretationDocument48 pagesBasic EKG InterpretationAimee Ann Pauco MacaraegPas encore d'évaluation
- Study Guide #10 With HEENT ChecklistDocument4 pagesStudy Guide #10 With HEENT ChecklistPrince DuPas encore d'évaluation
- Nursing QuestionnairesDocument3 pagesNursing QuestionnairesDianne Marbella AlvaradoPas encore d'évaluation
- Summary of Normal Laboratory ValuesDocument7 pagesSummary of Normal Laboratory ValuesIvan Matthew SuperioPas encore d'évaluation
- Cardiac Meds To MemorizeDocument4 pagesCardiac Meds To MemorizekellyaePas encore d'évaluation
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- Assignment 1111Document2 pagesAssignment 1111z707yPas encore d'évaluation
- Newborn Findings Respiratory: NAME: - DATE: - Nursery AssessmentDocument7 pagesNewborn Findings Respiratory: NAME: - DATE: - Nursery AssessmentAllana Louisse AbellanosaPas encore d'évaluation
- Newborn Physical AssessmentDocument7 pagesNewborn Physical AssessmentBinal JoshiPas encore d'évaluation
- OBSTETRIC ASSESSMENT TOOLDocument5 pagesOBSTETRIC ASSESSMENT TOOLDud AccPas encore d'évaluation
- Blue MondayDocument3 pagesBlue MondayElena APas encore d'évaluation
- Urinary SystemDocument9 pagesUrinary SystemCUESCANO, CRISTEL G. BSMT 2-APas encore d'évaluation
- Surgical ObturatorDocument4 pagesSurgical ObturatordentalteethPas encore d'évaluation
- نموذج انقاذ حياة الجديدDocument2 pagesنموذج انقاذ حياة الجديدraad_alghamdi_1Pas encore d'évaluation
- Complete Report OAPR-77102 Praveen 29aug2019Document13 pagesComplete Report OAPR-77102 Praveen 29aug2019Praveen MNPas encore d'évaluation
- Krok 2 Medicine (EN)_ Attempt review 4Document52 pagesKrok 2 Medicine (EN)_ Attempt review 4IS ZDPas encore d'évaluation
- Paediatric Formulation Books Inventory List 2013-10-10Document15 pagesPaediatric Formulation Books Inventory List 2013-10-10LUIS MIGUEL CASTILLA MORANPas encore d'évaluation
- Podcast 1 ScriptDocument2 pagesPodcast 1 Scriptapi-384802416Pas encore d'évaluation
- Effect of Bhramari Pranayama and Yoga NidraDocument3 pagesEffect of Bhramari Pranayama and Yoga Nidrajuan_emilioPas encore d'évaluation
- Family Clinic Inc Colleges Manila Nursing ProgramDocument21 pagesFamily Clinic Inc Colleges Manila Nursing Programkian5Pas encore d'évaluation
- CARNOsiNe EXTRA Product ReviewDocument40 pagesCARNOsiNe EXTRA Product Reviewdranita@yahoo.comPas encore d'évaluation
- Pathophysiology of OsteoporosisDocument6 pagesPathophysiology of OsteoporosisZenithaMeidaPas encore d'évaluation
- Immunodiagnostic TechniquesDocument37 pagesImmunodiagnostic TechniquesRima Carolina Bahsas ZakyPas encore d'évaluation
- Henrich To Fall Risk ModelDocument2 pagesHenrich To Fall Risk ModelDiyah RahmawatiPas encore d'évaluation
- Management of HypospadiasDocument34 pagesManagement of HypospadiasAdebisiPas encore d'évaluation
- Pharmacotherapy A Pathophysiolaogic Approach 8 TH Edition 2538 2560Document23 pagesPharmacotherapy A Pathophysiolaogic Approach 8 TH Edition 2538 2560kikiPas encore d'évaluation
- Laboratorios Valores EndocrinoDocument88 pagesLaboratorios Valores EndocrinoS OPas encore d'évaluation
- Q A 1Document48 pagesQ A 1ChannelGPas encore d'évaluation
- KadDocument28 pagesKadhardiff12Pas encore d'évaluation
- 02 Phallosan Manual GB 222x137 LowresDocument8 pages02 Phallosan Manual GB 222x137 LowresJenifer ConelyPas encore d'évaluation
- Small Animal Cytologic DiagnosisDocument920 pagesSmall Animal Cytologic DiagnosisLaura SchulzPas encore d'évaluation
- MRCOG Part 2 September 2017 Recalls FinalDocument13 pagesMRCOG Part 2 September 2017 Recalls FinalSaeed HasanPas encore d'évaluation
- Molecular Biology: Test Name Result Flag Units Ref. ValDocument1 pageMolecular Biology: Test Name Result Flag Units Ref. ValArabPas encore d'évaluation
- Acute Abdomen During Pregnancy 2014 PDFDocument584 pagesAcute Abdomen During Pregnancy 2014 PDFlula gestiana taufan100% (1)
- Ob2 Sas 40Document7 pagesOb2 Sas 40????Pas encore d'évaluation
- ABCDE ManagementDocument26 pagesABCDE ManagementHilmy Haydar El-FauzyPas encore d'évaluation
- Department of Community and Family Medicine AIIMS, RishikeshDocument16 pagesDepartment of Community and Family Medicine AIIMS, RishikeshAbhinav KumarPas encore d'évaluation
- PATHFit Lesson 1 - Physical Fitness ComponentsDocument48 pagesPATHFit Lesson 1 - Physical Fitness ComponentsKenneth Bowers100% (3)
- NPHCEDocument13 pagesNPHCEzain3kmdPas encore d'évaluation
- Sleep DisorderDocument43 pagesSleep DisorderSyed Waqas NaqviPas encore d'évaluation