Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Physical AssessmentDocument19 pagesPhysical AssessmentMamerto Q. Flores IIIPas encore d'évaluation
- Physiotherapy Exercises Following Transfemoral (Above Knee) AmputationDocument5 pagesPhysiotherapy Exercises Following Transfemoral (Above Knee) AmputationLuqmanul HakimPas encore d'évaluation
- 1920 1924Document16 pages1920 1924api-246211793Pas encore d'évaluation
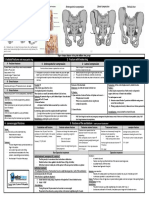
- Fracturte of Pelvis PDFDocument2 pagesFracturte of Pelvis PDFYogi drPas encore d'évaluation
- Distal Radius Fracture Outcomes and RehabilitationDocument4 pagesDistal Radius Fracture Outcomes and Rehabilitationerfan khanPas encore d'évaluation
- Notes On Extra-Contractual ObligationsDocument2 pagesNotes On Extra-Contractual ObligationslchieSPas encore d'évaluation
- Stargate For Savage Worlds v0 6Document16 pagesStargate For Savage Worlds v0 6treat123Pas encore d'évaluation
- Torts Midterms Reviewer Final PDFDocument9 pagesTorts Midterms Reviewer Final PDFDarla GreyPas encore d'évaluation
- IG Bio Case StudyDocument2 pagesIG Bio Case StudyMikaela SunPas encore d'évaluation
- Blyton Enid Now For A Story 1948Document193 pagesBlyton Enid Now For A Story 1948athinapolos100% (1)
- Austin Journal of Musculoskeletal DisordersDocument4 pagesAustin Journal of Musculoskeletal DisordersAustin Publishing GroupPas encore d'évaluation
- HUBS1105 Glenohumeral Joint and Muscles of The Shoulder Region Lectures CombinedDocument7 pagesHUBS1105 Glenohumeral Joint and Muscles of The Shoulder Region Lectures CombinedChloe HeuchanPas encore d'évaluation
- Congenital Muscular TorticollisDocument5 pagesCongenital Muscular TorticollisKevin Paul ZuñigaPas encore d'évaluation
- 8B - Spondylolysis, SpondylolisthesisDocument14 pages8B - Spondylolysis, SpondylolisthesismorlaszloPas encore d'évaluation
- AO Trauma Course - Basic Principles of Fracture Management Syllabus For FacultyDocument27 pagesAO Trauma Course - Basic Principles of Fracture Management Syllabus For FacultyPablo GerardoPas encore d'évaluation
- Radiologic Positioning PrinciplesDocument20 pagesRadiologic Positioning PrinciplesEugene De PanoPas encore d'évaluation
- Brachial Plexus InjuryDocument10 pagesBrachial Plexus InjurySanditya FadliPas encore d'évaluation
- TLE-AFA-AgriCrop Grade9 Q1 LAS3Document6 pagesTLE-AFA-AgriCrop Grade9 Q1 LAS3Van ImperialPas encore d'évaluation
- 001 What Is Thai Massage (FreeCourseWeb - Com)Document6 pages001 What Is Thai Massage (FreeCourseWeb - Com)Victor FernandesPas encore d'évaluation
- Quotation: Furathama Ehee Training CentreDocument5 pagesQuotation: Furathama Ehee Training Centrehassan2020Pas encore d'évaluation
- Cats and Dogs Compare and Contrast EssayDocument8 pagesCats and Dogs Compare and Contrast Essayjvscmacaf100% (2)
- Aim and Principle of First AidDocument11 pagesAim and Principle of First AidAanchal BansalPas encore d'évaluation
- Hirac SampleDocument12 pagesHirac Sampleyelsa otreblaPas encore d'évaluation
- English Lesson Plan The Dog Named Duke By: William D. EllisDocument16 pagesEnglish Lesson Plan The Dog Named Duke By: William D. EllisGurdeepPas encore d'évaluation
- Research Paper-2Document15 pagesResearch Paper-2api-641155139Pas encore d'évaluation
- Electrically Heated Cappings Separator: Apiacta 1, 1976Document4 pagesElectrically Heated Cappings Separator: Apiacta 1, 1976elpancaseroPas encore d'évaluation
- Jamie TakenDocument77 pagesJamie TakenCine DadaPas encore d'évaluation
- Surgical Sutures-10Document25 pagesSurgical Sutures-10badar_aqPas encore d'évaluation
- Pathophysiology: A Clinical Approach (2nd Ed.) - Braun Anderson (Chapter 3)Document8 pagesPathophysiology: A Clinical Approach (2nd Ed.) - Braun Anderson (Chapter 3)Mcat NotensionPas encore d'évaluation
- Medical For Athletes 2 1Document2 pagesMedical For Athletes 2 1james hardenPas encore d'évaluation