Vous aimerez peut-être aussi
- Electrical BurnsDocument27 pagesElectrical BurnsGautam KalraPas encore d'évaluation
- Sleep Disorders Classification and TreatmentDocument5 pagesSleep Disorders Classification and TreatmentIsabel CastilloPas encore d'évaluation
- Solution Manual For Human Anatomy Physiology Cat Version 4th Edition Terry Martin Cynthia Prentice CraverDocument6 pagesSolution Manual For Human Anatomy Physiology Cat Version 4th Edition Terry Martin Cynthia Prentice CraverKelly Adams96% (27)
- Management of Chronic Conditions in The Foot and Lower Leg, 1e. (2015)Document268 pagesManagement of Chronic Conditions in The Foot and Lower Leg, 1e. (2015)Mitul Patel100% (2)
- General Surgery MCQDocument190 pagesGeneral Surgery MCQلمسة مصمم100% (1)
- Sleep Disorders GuideDocument30 pagesSleep Disorders GuideAmit TamboliPas encore d'évaluation
- NCLEX Question C AnswersDocument14 pagesNCLEX Question C AnswersDavis WhitePas encore d'évaluation
- Local Anesthesia Part-1Document33 pagesLocal Anesthesia Part-1Abdul RazakPas encore d'évaluation
- Managing Adult Insomnia ConfidentlyDocument8 pagesManaging Adult Insomnia ConfidentlyJuliana RodriguezPas encore d'évaluation
- Administering O2 TherapyDocument22 pagesAdministering O2 TherapyWilbert Andrew FlojemonPas encore d'évaluation
- Everything You Need to Know About Sleep DisordersDocument19 pagesEverything You Need to Know About Sleep DisordersOlive CantosPas encore d'évaluation
- CCNDocument39 pagesCCNMann TSha100% (1)
- Insomnia: non pharmacological approachD'EverandInsomnia: non pharmacological approachPas encore d'évaluation
- Intradialytic ComplicationsDocument61 pagesIntradialytic ComplicationsKatherine NavarroPas encore d'évaluation
- Mai - InsomniaDocument8 pagesMai - InsomniaHendra PulunganPas encore d'évaluation
- Dsm-Iv DSM-5: Table 3.36 DSM-IV To DSM-5 Insomnia Disorder ComparisonDocument2 pagesDsm-Iv DSM-5: Table 3.36 DSM-IV To DSM-5 Insomnia Disorder ComparisonRashella Jessica JoePas encore d'évaluation
- Jcom Mar00 InsomniaDocument9 pagesJcom Mar00 InsomniafarhantunichiaPas encore d'évaluation
- Sleep Disturbances: Rene E - CormierDocument6 pagesSleep Disturbances: Rene E - CormierAdam GenturPas encore d'évaluation
- By: Reashnaa A/P Loganathan Yunisa Meutia Putri Zahra Fitrianti Preseptor: R.M. Haryadi Karyono, DR., SPKJDocument51 pagesBy: Reashnaa A/P Loganathan Yunisa Meutia Putri Zahra Fitrianti Preseptor: R.M. Haryadi Karyono, DR., SPKJmeutiaputripuyPas encore d'évaluation
- Go To:: 4th Edition (DSM) - IV, Which Is Published by The American Psychiatric Association (Document25 pagesGo To:: 4th Edition (DSM) - IV, Which Is Published by The American Psychiatric Association (rebalez gamingPas encore d'évaluation
- A Study On Quality and Quantity of Sleep Disturbances Associated With Their Quality of Life in Psychiatric PatientsDocument6 pagesA Study On Quality and Quantity of Sleep Disturbances Associated With Their Quality of Life in Psychiatric PatientsIjsrnet EditorialPas encore d'évaluation
- World Psychiatry - 2019 - KrystalDocument16 pagesWorld Psychiatry - 2019 - Krystalvalentino officialPas encore d'évaluation
- Insomnio CronicoDocument17 pagesInsomnio CronicoDra Carolina Escalante Neurologa de AdultosPas encore d'évaluation
- The Assessment and Management of Insomnia An UpdateDocument16 pagesThe Assessment and Management of Insomnia An UpdateWita AnggraeniPas encore d'évaluation
- Nursing Care Plan For InsomiaDocument4 pagesNursing Care Plan For InsomiaLord Pozak MillerPas encore d'évaluation
- Sleep-Wake DisordersDocument4 pagesSleep-Wake DisordersJohn PagangpangPas encore d'évaluation
- Insomnia and HypersomnolenceDocument9 pagesInsomnia and HypersomnolenceLABADAN, JOHANNA ALAINE S. 3-2Pas encore d'évaluation
- Aaft 14 I 1 P 33Document3 pagesAaft 14 I 1 P 33Zihan viranandaPas encore d'évaluation
- Sleep-Wake DisordersDocument14 pagesSleep-Wake Disordersnathanielge19Pas encore d'évaluation
- Sleep DisordersDocument49 pagesSleep DisordersShivam SoniPas encore d'évaluation
- Insomniaprevalenceconseque PDFDocument6 pagesInsomniaprevalenceconseque PDFYumna Satyani LasiyoPas encore d'évaluation
- Global Perspective Q&a Template 2021Document4 pagesGlobal Perspective Q&a Template 2021陈梓阳Pas encore d'évaluation
- Sleep DisordersDocument5 pagesSleep DisorderssookoojessicaPas encore d'évaluation
- Sleep Deprivation HTPDocument5 pagesSleep Deprivation HTPNikka PelayoPas encore d'évaluation
- Lecture+6+States+of+Consciousness PostingDocument62 pagesLecture+6+States+of+Consciousness PostingyuihkgPas encore d'évaluation
- Excessive daytime sleepiness diagnosisDocument54 pagesExcessive daytime sleepiness diagnosisKousar IshaqPas encore d'évaluation
- Infectious DemoDocument42 pagesInfectious DemoLaura TapiaPas encore d'évaluation
- Sleep & Dreams - CombinedDocument47 pagesSleep & Dreams - CombinedqwerasdfPas encore d'évaluation
- PDF Data AnalysisDocument5 pagesPDF Data AnalysisAshley FernandezPas encore d'évaluation
- Insomnia: Case Studies in Family Practice: Kamil Mohd Ariff Zailinawati Abu Hassan Author Information PMC DisclaimerDocument12 pagesInsomnia: Case Studies in Family Practice: Kamil Mohd Ariff Zailinawati Abu Hassan Author Information PMC DisclaimerAbhishek AgrawalPas encore d'évaluation
- Insomnia: A Presentation byDocument19 pagesInsomnia: A Presentation byHerlina HasibuanPas encore d'évaluation
- Clasificarea Tulburarilor de Somn 2Document12 pagesClasificarea Tulburarilor de Somn 2Anna DiaconuPas encore d'évaluation
- Sleep-Wake DisordersDocument61 pagesSleep-Wake Disorderskume senbetaPas encore d'évaluation
- NCP 1Document1 pageNCP 1Rommelie CaballeroPas encore d'évaluation
- SAS - Session 11 - PSY079 - Intro To PsychologyDocument8 pagesSAS - Session 11 - PSY079 - Intro To PsychologyLordelee Mae N PamaylaonPas encore d'évaluation
- LAPMAN - 6130020049 Maulidatul Jinani FDocument22 pagesLAPMAN - 6130020049 Maulidatul Jinani FFirda JinanPas encore d'évaluation
- Pato Insomnia PDFDocument14 pagesPato Insomnia PDFdilaPas encore d'évaluation
- InsomniaDocument13 pagesInsomniadr.cidgutPas encore d'évaluation
- Clinical Guide to Sleep DisordersDocument23 pagesClinical Guide to Sleep DisordersBEA RADAPas encore d'évaluation
- Sleep DisordersDocument45 pagesSleep DisordersOse IbhadodePas encore d'évaluation
- Jama Krystal 2021 PG 210031 1640024194.48206Document1 pageJama Krystal 2021 PG 210031 1640024194.48206SibaraniPas encore d'évaluation
- Jolanta Orzeł-Gryglewska: Yl) PL ÊwhwlyzDocument20 pagesJolanta Orzeł-Gryglewska: Yl) PL Êwhwlyzzrombie7Pas encore d'évaluation
- Consequences of Sleep Deprivation: Jolanta Orzeł-GryglewskaDocument20 pagesConsequences of Sleep Deprivation: Jolanta Orzeł-GryglewskaLulu LuwiiPas encore d'évaluation
- Sleep and Anxiety DisordersDocument11 pagesSleep and Anxiety DisordersRebeca EspinosaPas encore d'évaluation
- Psychologic and Psychiatric Assessment: © 2021 Elsevier Inc. All Rights ReservedDocument6 pagesPsychologic and Psychiatric Assessment: © 2021 Elsevier Inc. All Rights ReservedDiane MxPas encore d'évaluation
- Understanding Sleep Disorders and Their ClassificationDocument6 pagesUnderstanding Sleep Disorders and Their ClassificationAh BoonPas encore d'évaluation
- Lesson 5: ESP and States of ConsciousnessDocument4 pagesLesson 5: ESP and States of ConsciousnessAriadna ApolonioPas encore d'évaluation
- Concepts - 1997 - Management of InsomniaDocument6 pagesConcepts - 1997 - Management of InsomniaFranciscoPas encore d'évaluation
- Sleep Disorders: Review Neurology Series Editor, William J. Mullally, MDDocument8 pagesSleep Disorders: Review Neurology Series Editor, William J. Mullally, MDniPas encore d'évaluation
- To Study The Mystery of Sleep, Sleep Disorder or Insomnia and Its Effect On Physical and Mental HealthDocument3 pagesTo Study The Mystery of Sleep, Sleep Disorder or Insomnia and Its Effect On Physical and Mental HealthInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Sleep Disorders: Its Causes and TreatmentsDocument20 pagesSleep Disorders: Its Causes and TreatmentsBasari OdalPas encore d'évaluation
- Management of Sleep Disorders in ElderlyDocument20 pagesManagement of Sleep Disorders in ElderlyRiyaSinghPas encore d'évaluation
- อ.จักรกฤษณ์ - sleep deprivation กค 2564 handouts updateDocument18 pagesอ.จักรกฤษณ์ - sleep deprivation กค 2564 handouts updateGayvalin St.Pas encore d'évaluation
- Sleep Disorders: InsomniaDocument6 pagesSleep Disorders: InsomniaNazrul Naeem AsmawiPas encore d'évaluation
- Sleep DisordersDocument65 pagesSleep DisordersZeleke temechewPas encore d'évaluation
- How To Manage Sleep DisordersDocument19 pagesHow To Manage Sleep DisordersTwinkle SalongaPas encore d'évaluation
- NCP For Older Adults With Sleep DisturbanceDocument17 pagesNCP For Older Adults With Sleep DisturbanceAlienda Puspita PutriPas encore d'évaluation
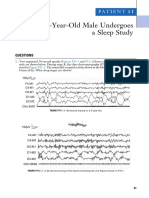
- A 3-Year-Old Male Undergoes A Sleep Study: Patient 1 1Document3 pagesA 3-Year-Old Male Undergoes A Sleep Study: Patient 1 1Mitul PatelPas encore d'évaluation
- A Child With Repeated Movements During Sleep: Patient28Document3 pagesA Child With Repeated Movements During Sleep: Patient28Mitul PatelPas encore d'évaluation
- TidalDocument23 pagesTidalMitul PatelPas encore d'évaluation
- WTP LyricsDocument15 pagesWTP LyricsMitul PatelPas encore d'évaluation
- Obstructive Sleep Apnea: Treatment Overview and Medical TreatmentsDocument7 pagesObstructive Sleep Apnea: Treatment Overview and Medical TreatmentsMitul PatelPas encore d'évaluation
- WTP LyricsDocument15 pagesWTP LyricsMitul PatelPas encore d'évaluation
- A Child With Mouth Movements During Sleep and A Teenager With Jerks in The Morning After AwakeningDocument3 pagesA Child With Mouth Movements During Sleep and A Teenager With Jerks in The Morning After AwakeningMitul PatelPas encore d'évaluation
- Foo DRDocument1 pageFoo DRMitul PatelPas encore d'évaluation
- Miss CamaraderieDocument2 pagesMiss CamaraderieMitul PatelPas encore d'évaluation
- CoverDocument1 pageCoverMitul PatelPas encore d'évaluation
- (Op-Ed) Azealia Banks and The Double Standard of Mental IllnessDocument3 pages(Op-Ed) Azealia Banks and The Double Standard of Mental IllnessMitul PatelPas encore d'évaluation
- Excusez-Moi, Est-Ce Que Vous Savez Où Est Un Bon Restaurant Parisienne?Document1 pageExcusez-Moi, Est-Ce Que Vous Savez Où Est Un Bon Restaurant Parisienne?Mitul PatelPas encore d'évaluation
- 2 PageDocument1 page2 PageMitul PatelPas encore d'évaluation
- CCNC Depression Toolkit (Dragged)Document1 pageCCNC Depression Toolkit (Dragged)Mitul PatelPas encore d'évaluation
- Prior Authorization Conditions For Approval of Humira® (Adalimumab)Document4 pagesPrior Authorization Conditions For Approval of Humira® (Adalimumab)Mitul PatelPas encore d'évaluation
- (Op-Ed) Azealia Banks and The Double Standard of Mental IllnessDocument3 pages(Op-Ed) Azealia Banks and The Double Standard of Mental IllnessMitul PatelPas encore d'évaluation
- Parting Gift NotesDocument4 pagesParting Gift NotesMitul PatelPas encore d'évaluation
- Netter ProceduresDocument2 pagesNetter ProceduresMitul PatelPas encore d'évaluation
- Cardioversion For Atrial Fibrillation - ClinicalKeyDocument27 pagesCardioversion For Atrial Fibrillation - ClinicalKeyAnthony Martin Corrales ParedesPas encore d'évaluation
- Endocrine System: Cell Secretion Types Types of HormonesDocument6 pagesEndocrine System: Cell Secretion Types Types of HormonesKrissia BaasisPas encore d'évaluation
- The Organization of the Human BodyDocument6 pagesThe Organization of the Human Bodysithum sanjanaPas encore d'évaluation
- Atrium FlutterDocument11 pagesAtrium FlutterSiti Maryam NatadisastraPas encore d'évaluation
- Chapter 19 Citric Acide CycleDocument37 pagesChapter 19 Citric Acide CycleWaad MajidPas encore d'évaluation
- Cues/Needs Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective Data: IndependentDocument2 pagesCues/Needs Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective Data: IndependentArabelle GOPas encore d'évaluation
- Multiparameter Patient Monitors-1Document12 pagesMultiparameter Patient Monitors-1robert robPas encore d'évaluation
- Heart and blood vessels explained in detailDocument15 pagesHeart and blood vessels explained in detailIDKPas encore d'évaluation
- HypernatremiaDocument2 pagesHypernatremiaAliyah PundagPas encore d'évaluation
- Endocrine and Metabolic Physiology BCQDocument4 pagesEndocrine and Metabolic Physiology BCQBlackstarPas encore d'évaluation
- Care for Clients with Cognitive and Perceptual DisordersDocument93 pagesCare for Clients with Cognitive and Perceptual DisordersWoot RootPas encore d'évaluation
- Research Article: Effects of Forest Bathing On Cardiovascular and Metabolic Parameters in Middle-Aged MalesDocument8 pagesResearch Article: Effects of Forest Bathing On Cardiovascular and Metabolic Parameters in Middle-Aged MalesMikael MoazanPas encore d'évaluation
- Bio 5 Questions ActDocument3 pagesBio 5 Questions ActAndy GacuyaPas encore d'évaluation
- Body Fluids and Circulation NotesDocument8 pagesBody Fluids and Circulation Notessatyam6449Pas encore d'évaluation
- Cardiogenic Shock and IcuDocument9 pagesCardiogenic Shock and IcuDayu MandhaPas encore d'évaluation
- HTN Keith RN Mike Kelly Case Study AnswersDocument13 pagesHTN Keith RN Mike Kelly Case Study AnswersabbiePas encore d'évaluation
- Optimal Management of Hypotension During Cesarean Delivery Under Spinal AnesthesiaDocument22 pagesOptimal Management of Hypotension During Cesarean Delivery Under Spinal AnesthesiaJosé Alberto LozanoPas encore d'évaluation
- Summative Test 1 ScienceDocument2 pagesSummative Test 1 ScienceIris Klench A. BaldovisoPas encore d'évaluation
- Final Draft - Sleep EssayDocument11 pagesFinal Draft - Sleep Essayapi-609533757Pas encore d'évaluation
- Asam BasaDocument22 pagesAsam BasaHariningtyas Dian RPas encore d'évaluation
- World Tree Herbals®-TCM Heart Deficient-Empty PatternsDocument4 pagesWorld Tree Herbals®-TCM Heart Deficient-Empty PatternsfulvioschiavoPas encore d'évaluation
- Module 6, Mid.101 Systematic ChangesDocument11 pagesModule 6, Mid.101 Systematic ChangesNicole DeusPas encore d'évaluation
- SC123 Human Physiology - McGuireDocument5 pagesSC123 Human Physiology - McGuireAbhinav ThakurPas encore d'évaluation