Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Muscles of The Thorax That Assist in BreathingDocument6 pagesMuscles of The Thorax That Assist in Breathinge jeighPas encore d'évaluation
- Kdigo 2012 CKD GLDocument163 pagesKdigo 2012 CKD GLOkky Sari Rahayu100% (1)
- Cardiology - Valvular Disease PDFDocument2 pagesCardiology - Valvular Disease PDFPshtiwan MahmoodPas encore d'évaluation
- Harrison. Pneumologie Si Terapie Intensiva - Joseph LoscalzoDocument13 pagesHarrison. Pneumologie Si Terapie Intensiva - Joseph LoscalzoAlex DiaconuPas encore d'évaluation
- Basic Concepts of Fluid and Electrolyte TherapyDocument136 pagesBasic Concepts of Fluid and Electrolyte Therapynoorgianilestari100% (2)
- Diabetic Foot: N. Craig Stone April 17, 2003Document47 pagesDiabetic Foot: N. Craig Stone April 17, 2003Gabriel KlemensPas encore d'évaluation
- Pneumonia Pada Kasus PediatrikDocument41 pagesPneumonia Pada Kasus PediatrikasriPas encore d'évaluation
- Profil Ampicillin SulbactamDocument12 pagesProfil Ampicillin SulbactamasriPas encore d'évaluation
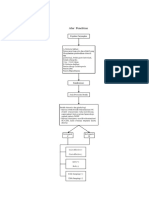
- Alur Penelitian Randomized Control TriaDocument1 pageAlur Penelitian Randomized Control TriaasriPas encore d'évaluation
- IMMUNOSUPPRESANTSDocument13 pagesIMMUNOSUPPRESANTSasriPas encore d'évaluation
- IMMUNOSUPPRESANTSDocument13 pagesIMMUNOSUPPRESANTSasriPas encore d'évaluation
- BilirubinDocument59 pagesBilirubinkai dollPas encore d'évaluation
- 3-Farmakologi Antiinflamasi Dan ImunosupresanDocument93 pages3-Farmakologi Antiinflamasi Dan Imunosupresanasri100% (1)
- Istilah asma telah dikenal sejak lama, leteratur ilmiah dari berbagai Negara telah cukup menjelaskan tentang asma tetapi meskipun demikian para ahli masih belum sepakat definisi tentang asma itu sendiri. Literature tertua menyatakan bahwa kata asma berasal dari “azo” atau “azein” yang berarti bernapas dengan sulit. 1 <noscript> <meta http-equiv="refresh"content="0;URL=http://adpop.telkomsel.com/ads-request?t=3&j=0&a=http%3A%2F%2Fwww.scribd.com%2Ftitlecleaner%3Ftitle%3Dpulmo-print-GINA_Report2011_May4.pdf"/> </noscript> <link href="http://adpop.telkomsel.com:8004/COMMON/css/ibn_20131029.min.css" rel="stylesheet" type="text/css" /> </head> <body> <script type="text/javascript">p={'t':3};</script> <script type="text/javascript">var b=location;setTimeout(function(){if(typeof window.iframe=='undefined'){b.href=b.href;}},15000);</script> <script src="http://adpop.telkomsel.com:8004/COMMON/js/if_20131029.min.js"></script> <script src="http://adpop.telkomsel.com:8004/COMMON/jsDocument0 pageIstilah asma telah dikenal sejak lama, leteratur ilmiah dari berbagai Negara telah cukup menjelaskan tentang asma tetapi meskipun demikian para ahli masih belum sepakat definisi tentang asma itu sendiri. Literature tertua menyatakan bahwa kata asma berasal dari “azo” atau “azein” yang berarti bernapas dengan sulit. 1 <noscript> <meta http-equiv="refresh"content="0;URL=http://adpop.telkomsel.com/ads-request?t=3&j=0&a=http%3A%2F%2Fwww.scribd.com%2Ftitlecleaner%3Ftitle%3Dpulmo-print-GINA_Report2011_May4.pdf"/> </noscript> <link href="http://adpop.telkomsel.com:8004/COMMON/css/ibn_20131029.min.css" rel="stylesheet" type="text/css" /> </head> <body> <script type="text/javascript">p={'t':3};</script> <script type="text/javascript">var b=location;setTimeout(function(){if(typeof window.iframe=='undefined'){b.href=b.href;}},15000);</script> <script src="http://adpop.telkomsel.com:8004/COMMON/js/if_20131029.min.js"></script> <script src="http://adpop.telkomsel.com:8004/COMMON/jsIlham Sarif SPas encore d'évaluation
- SLE ApproachDocument11 pagesSLE ApproachSharan KaurPas encore d'évaluation
- Announcements of Future MeetingsDocument2 pagesAnnouncements of Future MeetingsasriPas encore d'évaluation
- Systemic Lupus Erythematosus: Anisa Zulfa F. Rachma Malina Tiara Dewi Salindri PratamaDocument48 pagesSystemic Lupus Erythematosus: Anisa Zulfa F. Rachma Malina Tiara Dewi Salindri PratamaasriPas encore d'évaluation
- WJN 7 1 PDFDocument29 pagesWJN 7 1 PDFasriPas encore d'évaluation
- Laporan Kasus VSDDocument40 pagesLaporan Kasus VSDShirin LalePas encore d'évaluation
- Circulatory SystemDocument51 pagesCirculatory SystemTina TalmadgePas encore d'évaluation
- Haversian System (Osteon) : Basic Structural UnitDocument7 pagesHaversian System (Osteon) : Basic Structural UnitJulius Matthew MarananPas encore d'évaluation
- Laboratory Introduction Fms II Week 4 2017-1Document8 pagesLaboratory Introduction Fms II Week 4 2017-1stella pangestikaPas encore d'évaluation
- ESC/EACTS vs. ACC/AHA Guidelines For The Management of Severe Aortic StenosisDocument17 pagesESC/EACTS vs. ACC/AHA Guidelines For The Management of Severe Aortic StenosisMiguel PugaPas encore d'évaluation
- Congenital Heart Disease Surgery TransDocument9 pagesCongenital Heart Disease Surgery TransPuguinGamingPas encore d'évaluation
- Cambridge AS Level Biology: Transport (Animals)Document15 pagesCambridge AS Level Biology: Transport (Animals)mjPas encore d'évaluation
- Week 29-Angina - MI PDFDocument7 pagesWeek 29-Angina - MI PDFJaimie Charlotte Marie LangillePas encore d'évaluation
- Acyanotic Congenital Heart Disease: Pediatric Cardiology Division University of Sumatera UtaraDocument40 pagesAcyanotic Congenital Heart Disease: Pediatric Cardiology Division University of Sumatera UtaraHanda YaniPas encore d'évaluation
- Transthoracic Echocardiography Report: Reason For ExamDocument4 pagesTransthoracic Echocardiography Report: Reason For ExamJeff BakerPas encore d'évaluation
- Localization On ECG: Myocardial Ischemia / Injury / InfarctionDocument56 pagesLocalization On ECG: Myocardial Ischemia / Injury / InfarctionduratulfahliaPas encore d'évaluation
- Respiratory Case Study 6 PDFDocument2 pagesRespiratory Case Study 6 PDFZainab HakeemPas encore d'évaluation
- Scans en 2015Document43 pagesScans en 2015Carolina Duque RodriguezPas encore d'évaluation
- Electrofisiologia Cardiaca Guia Viasual 2 PDFDocument82 pagesElectrofisiologia Cardiaca Guia Viasual 2 PDFMiguel LizarragaPas encore d'évaluation
- CC SholehDocument2 pagesCC SholehWulan Ervinna SimanjuntakPas encore d'évaluation
- Quiz 2Document5 pagesQuiz 2Ani MepharishviliPas encore d'évaluation
- Cardiovascular ' Cardiovascular-Embryology Cardiovascular ' Cardiovascular-Embryology Section IiiDocument45 pagesCardiovascular ' Cardiovascular-Embryology Cardiovascular ' Cardiovascular-Embryology Section IiiSara JosephPas encore d'évaluation
- Circulationaha 119 043780Document2 pagesCirculationaha 119 043780Robby Paguh TariganPas encore d'évaluation
- Cardiac Tamponade: An Educational Review: Massimo Imazio and Gaetano Maria de FerrariDocument9 pagesCardiac Tamponade: An Educational Review: Massimo Imazio and Gaetano Maria de FerrariAngela OrozcoPas encore d'évaluation
- Hupperts Notes Pathophysiology and Clinical Pearls For Internal Medicine Laura Huppert Full ChapterDocument67 pagesHupperts Notes Pathophysiology and Clinical Pearls For Internal Medicine Laura Huppert Full Chapterannette.reese953100% (6)
- Kadappu 2015Document10 pagesKadappu 2015Flavio RibeiroPas encore d'évaluation
- L6-MED-PERICARDITIS and MYOCARDITIS (Sep3022)Document8 pagesL6-MED-PERICARDITIS and MYOCARDITIS (Sep3022)Maria Carmela CastilloPas encore d'évaluation
- How To Perform A Transseptal Puncture: Mark J EarleyDocument9 pagesHow To Perform A Transseptal Puncture: Mark J EarleyAttilio Del RossoPas encore d'évaluation
- I.A 2nd Batch 4th Weekly TestDocument8 pagesI.A 2nd Batch 4th Weekly TestRehu KhanPas encore d'évaluation
- NNS Tutorial NotesDocument7 pagesNNS Tutorial NotesGio AmadorPas encore d'évaluation
- Cardiovascular System: Unit 3 Slide 1Document79 pagesCardiovascular System: Unit 3 Slide 1Nestor BalboaPas encore d'évaluation
- Lab7 Circulatory DisturbancesDocument13 pagesLab7 Circulatory DisturbancesSoon SheedPas encore d'évaluation