Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Sexual Abuse Shield Rule ReportDocument26 pagesSexual Abuse Shield Rule ReportCarlo ColumnaPas encore d'évaluation
- DOMESTIC ADOPTION-governed by DAA and Family Code Procedure Governed by Rule On Adoption (Aug 22, 2002)Document2 pagesDOMESTIC ADOPTION-governed by DAA and Family Code Procedure Governed by Rule On Adoption (Aug 22, 2002)WazzupPas encore d'évaluation
- Digest Abad Vs ViazonDocument2 pagesDigest Abad Vs ViazonIamIvy Donna PondocPas encore d'évaluation
- Guerrero, Et Al. v. General Motors Corporation, Et Al. - Document No. 6Document2 pagesGuerrero, Et Al. v. General Motors Corporation, Et Al. - Document No. 6Justia.comPas encore d'évaluation
- Oblicon 1106 - 1134Document14 pagesOblicon 1106 - 1134Hannah HazelPas encore d'évaluation
- Article - The Adoption of Children in Judaism and in Israel A Conceptual and Practical Review, 2Document26 pagesArticle - The Adoption of Children in Judaism and in Israel A Conceptual and Practical Review, 2אליעזר קופערPas encore d'évaluation
- MTA - Application FormDocument2 pagesMTA - Application Formedgar requilmePas encore d'évaluation
- UAE LawDocument37 pagesUAE LawCristina ŞtefanPas encore d'évaluation
- Office Order No. 223 - 14 Subject: Revised Documentary Requirements For Social Insurance Benefits and Other Related Claims and TransactionsDocument9 pagesOffice Order No. 223 - 14 Subject: Revised Documentary Requirements For Social Insurance Benefits and Other Related Claims and TransactionsLIERAPas encore d'évaluation
- Separation Agreement: FactsDocument13 pagesSeparation Agreement: FactsLien PatrickPas encore d'évaluation
- Estate Planning QuestionnaireDocument14 pagesEstate Planning QuestionnaireTim KiehlPas encore d'évaluation
- Law of AdoptionDocument8 pagesLaw of AdoptionNasma AbidiPas encore d'évaluation
- Brondial Notes - Special ProceedingDocument34 pagesBrondial Notes - Special ProceedingAedler Jo-lean Atutubo100% (3)
- Emergency Petition To Remove Girl (6) From Sexually Abusive Father, Maine April 16 2013Document16 pagesEmergency Petition To Remove Girl (6) From Sexually Abusive Father, Maine April 16 2013Expect Us100% (1)
- Guardian HandbookDocument32 pagesGuardian Handbookellieboo39Pas encore d'évaluation
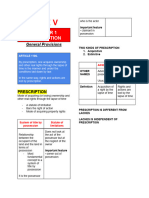
- AE 07 - Module 1 - Lesson 1 and 2 - Intro To Law, Prescription PDFDocument109 pagesAE 07 - Module 1 - Lesson 1 and 2 - Intro To Law, Prescription PDF유니스Pas encore d'évaluation
- Application FOR Pre-Need Plans: 08 JULY 2020Document2 pagesApplication FOR Pre-Need Plans: 08 JULY 2020Gerry Avila NaguitPas encore d'évaluation
- Crim SOC31Document6 pagesCrim SOC31Jen PaezPas encore d'évaluation
- Lakeview WaiverDocument1 pageLakeview WaiverPrice FerrellPas encore d'évaluation
- In Re Petition For Adoption of Michelle P. Lim G.R. Nos. 168992-93 May 21, 2009Document12 pagesIn Re Petition For Adoption of Michelle P. Lim G.R. Nos. 168992-93 May 21, 2009Blessa Raynes AzañaPas encore d'évaluation
- The Children's Code Bill, 2022 FinalDocument178 pagesThe Children's Code Bill, 2022 FinalKaka MwenyaPas encore d'évaluation
- Family Court Rules PDFDocument10 pagesFamily Court Rules PDFJOHNPas encore d'évaluation
- Chapter 2 Capacity To Buy and SellDocument4 pagesChapter 2 Capacity To Buy and SellApple Ke-ePas encore d'évaluation
- Babita Ngo ReportDocument18 pagesBabita Ngo Reportpsd_vidPas encore d'évaluation
- 2008 (4) ALL MR 882.htmlDocument5 pages2008 (4) ALL MR 882.htmlJ VenkatramanPas encore d'évaluation
- Specpro ReportDocument31 pagesSpecpro ReportLyleTheresePas encore d'évaluation
- California Survival School Release and Waiver Agreement 2018 PDFDocument2 pagesCalifornia Survival School Release and Waiver Agreement 2018 PDFAnonymous zhNqC0KmmPas encore d'évaluation
- 12.21 C. Sanctions For False Allegations - California Child Custody Litigation and Practice - CEBDocument28 pages12.21 C. Sanctions For False Allegations - California Child Custody Litigation and Practice - CEBRicardo Gomez0% (1)
- Adoption, AIR 1961 MP 173, Brejendra Narayan Ganguly and ... Vs Chinta Haran Sarkar and Anr. On 10 October, 1960Document5 pagesAdoption, AIR 1961 MP 173, Brejendra Narayan Ganguly and ... Vs Chinta Haran Sarkar and Anr. On 10 October, 1960Skk IrisPas encore d'évaluation
- Topic 9 Guardianship and Custody (Islamic Law)Document27 pagesTopic 9 Guardianship and Custody (Islamic Law)faezaahPas encore d'évaluation