Académique Documents
Professionnel Documents
Culture Documents
2018 PHYS REV Ingestão Alimentar e Comportamento Alimentar Depois de Cirurgia Bariátrica
Transféré par
LeonardoCampanelliCopyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
2018 PHYS REV Ingestão Alimentar e Comportamento Alimentar Depois de Cirurgia Bariátrica
Transféré par
LeonardoCampanelliDroits d'auteur :
Formats disponibles
Physiol Rev 98: 1113–1141, 2018
Published May 2, 2018; doi:10.1152/physrev.00021.2017
FOOD INTAKE AND EATING BEHAVIOR AFTER
BARIATRIC SURGERY
Werd Al-Najim, Neil G. Docherty, and X Carel W. le Roux
Diabetes Complications Research Centre, Conway Institute, School of Medicine and Medical Sciences, University
College Dublin, Dublin, Ireland; Department of Gastrosurgical Research and Education, Institute of Clinical
Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; and Investigative Science,
Imperial College London, London, United Kingdom
Al-Najim W, Docherty NG, le Roux CW. Food Intake and Eating Behavior After
L
Bariatric Surgery. Physiol Rev 98: 1113–1141, 2018. Published May 2, 2018;
doi:10.1152/physrev.00021.2017.—Obesity is an escalating global chronic disease.
Bariatric surgery is a very efficacious treatment for obesity and its comorbidities.
Alterations to gastrointestinal anatomy during bariatric surgery result in neurological
and physiological changes affecting hypothalamic signaling, gut hormones, bile acids, and gut
microbiota, which coalesce to exert a profound influence on eating behavior. A thorough under-
standing of the mechanisms underlying eating behavior is essential in the management of patients
after bariatric surgery. Studies investigating candidate mechanisms have expanded dramatically in
the last decade. Herein we review the proposed mechanisms governing changes in eating behavior,
food intake, and body weight after bariatric surgery. Additive or synergistic effects of both condi-
tioned and unconditioned factors likely account for the complete picture of changes in eating
behavior. Considered application of strategies designed to support the underlying principles gov-
erning changes in eating behavior holds promise as a means of optimizing responses to surgery
and long-term outcomes.
I. IMPORTANT TERMS 1113 beginning with hunger and proceeding through satiation
II. INTRODUCTION 1113 and satiety, before returning to hunger (85). The conse-
III. OBESITY AND BARIATRIC SURGERY 1113 quences of when this loop becomes pathological are either
IV. BIOPSYCHOLOGY OF HUNGER,... 1116 overweight or underweight. Obesity and its associated com-
V. EATING BEHAVIOR AFTER... 1117 plications are increasing unabated, but bariatric surgery is
VI. MECHANISMS OF CHANGED... 1121 an effective treatment (50, 194, 254).
VII. CONCLUSION AND PERSPECTIVES 1132
Over the past decade, our knowledge of eating behavior has
increased dramatically, in particular the molecular and an-
I. IMPORTANT TERMS atomical basis of satiety. Important advances in the charac-
terization of the processes involved in eating behavior and
Hunger is the motivational impulse to seek and consume the changes that occur following bariatric surgery have oc-
food, geared towards initiating an eating episode. curred. More complete understanding of the changes in
eating behavior after surgery may help in the design of
Satiation is the process that brings an eating episode to an strategies to optimize the outcomes of bariatric surgery and
end. It commences when the gut senses fullness or when the moreover aid discovery of nonsurgical interventions for
person is satisfied with the amount consumed. weight loss and weight loss maintenance.
Satiety is the state in which the hunger drive, and conse-
quently eating episode, is inhibited. III. OBESITY AND BARIATRIC SURGERY
Obesity has been declared a chronic disease by a number of
II. INTRODUCTION global health organizations including the World Health Or-
ganization (WHO), Food and Drug Administration (FDA),
Hunger and satiation are the predominant signals involved the National Institutes of Health (NIH), the American Med-
in the initiation or termination of a meal. Psychological ical Association (AMA), and the Canadian Medical Associ-
experiences, peripheral physiological signals, and central ation (CMA) (6, 60). Worldwide the rates of obesity have
neural processes interact before, during, and after food in- reached epidemic proportions bringing with it a burden of
take to form a biopsychological closed loop conceptually associated comorbidities and negative impact on quality of
0031-9333/18 Copyright © 2018 the American Physiological Society 1113
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
life. Obesity likely represents a common phenotypic presen- larly gastric bypass and sleeve gastrectomy to more ac-
tation of several complex disorders involving maladaptive curately capture the breadth of physiological changes
changes in eating behavior, appetite regulation, and energy induced. Moreover, advocates of this alternative termi-
metabolism. Therefore, prevention and management of nology also point to the shift in emphasis it provides
obesity requires a multifaceted approach to achieve realistic towards viewing the health benefits associated with
goals. weight loss rather than simply weight loss itself as being
the key outcome (250).
Lifestyle changes together with diet and exercise are usually
considered as the first lines of prophylaxis and therapy in The Roux-en-Y gastric bypass (RYGB) is the procedure
weight management treatments and are the mainstay of most commonly and consistently performed over the last
associated public health messages. This is not dissimilar to three decades due to its effectiveness in weight loss and
lifestyle changes being the cornerstone of the public health weight loss maintenance (35). Nevertheless, RYGB is a
message in relation to the prevention and management of
technically demanding procedure and is associated with
hypertension, dyslipidemia, or diabetes. Frustratingly how-
major rearrangement of the normal gastrointestinal anat-
ever, lifestyle approaches for obesity are of limited efficacy
omy. In this procedure, the stomach is transected to gener-
in managing and treating severe overweight and its comor-
ate a small gastric pouch 15⫺30 ml in volume, and a lower
bidities. This is disappointing to clinicians and patients as
larger gastric remnant excluded from contact with food.
many fail to maintain weight loss in the long term. Only
around 15% of obese and overweight people who attempt The gastric pouch is then anastomosed to the distal limb of
to lose excess weight by diet therapy can manage to sustain a jejunotomy performed at the mid-jejunum thus forming
10% weight loss over a period of 1 yr (160). Dietary-in- the alimentary or Roux limb. In the absence of gastric res-
duced weight loss tends to be largely unsustainable with ervoir function or sphincter control, this rearrangement al-
weight rebound within 1 yr. In the majority of cases, all lows essentially instantaneous transfer of ingested food to
weight lost is regained within 3–5 yr (321). the small intestinal lumen. Gastric, pancreatic, and biliary
secretions flow undiluted in the biliopancreatic limb proxi-
In contrast to dietary approaches, bariatric surgery is a mal to the jejunal transection and are permitted to mix with
highly successful intervention for the treatment of obesity chyme in a common channel formed by side-to-side anas-
and diabetes and is becoming increasingly popular due to its tomosis of the biliopancreatic limb 100 –150 cm distal to
ability to foster substantial and sustainable weight loss with the gastro-jejunal anastomosis (218).
attendant improvements in health, functioning, and quality
of life (194, 211, 252, 254, 277). The Gastric Band (BAND) was previously more widely per-
formed but has declined in popularity in the last 5 yr (35).
This procedure involves the insertion of an adjustable hol-
A. Surgical Modalities low plastic and silicone ring around the stomach just below
the gastric cardia, creating a small pouch and a narrow
Bariatric surgery is an option for those obese patients for passage to the remaining part of the stomach. This proce-
whom lifestyle- and medication-based approaches have dure was originally thought to physically restrict meal size
proven ineffective. Bariatric surgery procedures have evolved and delay emptying of food from the pouch, thus producing
over the years starting from radical small bowel operations early and prolonged satiety (20). However, much of the
such as the jejunal-ileal bypass in the 1950s, to the gastric
effect of the procedure is now thought to be provoked by
bypass in the late 1960s (4, 120, 183), gastric banding in the
pressure applied on the Intraganglionic Laminar Endings
1990s (162), and the more recently popularized vertical sleeve
(IGLES) which relay afferent signals resulting in reductions
gastrectomy (5). Refinements to lessen the extent of recon-
in hunger (286). The gastric BAND causes a delayed bolus
figuration alongside the routine use of laparoscopic ap-
proaches have made the procedures safer, more efficient, transit into the infraband stomach but does not change
and characterized by a less severe side-effect profile (106). overall gastric emptying half-time, a key observation in re-
Under certain circumstances, more radical procedures like lation to the differential effect of BAND versus RYGB on
the Biliopancreatic Diversion/Duodenal Switch (BPD/DS) satiety, a topic developed in detail later in this manuscript
may still be used on occasion for cases of severe obesity with (41). Vertical Sleeve Gastrectomy (VSG) has become in-
significant complications, though the procedure is less pop- creasingly popular due to its relative simplicity and good
ular due to the high burden of postoperative nutritional clinical outcomes (46). VSG involves the excision of 70 –
deficiencies and related complications (10). 80% of the stomach to make a small stomach that creates a
high-pressure chamber that easily generates pressures suffi-
The different bariatric procedures currently vary with re- cient to overcome pyloric sphincter tone and thus results in
gard to their relative metabolic benefits, as well as surgical rapid gastric emptying.
risks. In some quarters, the term metabolic surgery is now
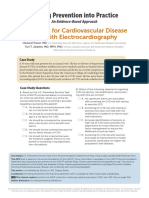
preferred to describe certain types of surgeries particu- FIGURE 1 shows the different bariatrics procedures.
1114 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
FIGURE 1. Anatomy of different bariatric procedures. Figures from left to right show RYGB, BAND, VSG, and
BPD/DS.
B. Positive and Negative Repercussions of to several possible organic diseases of the gastrointestinal
Surgical Weight Loss tract (119). Hypoglycemia occurs in 64 – 82% of patients
during the first 5 years of bariatric surgery (254). Several
Bariatric surgery produces 15–30% weight loss (1, 53, 139, hypotheses for its pathogenesis exist including improved B
145, 150, 214, 225, 226, 254, 275, 287), maintained for at cells mass and function, reduced level of ghrelin, improved
least 20 yr after procedures such as the RYGB. Moreover, insulin sensitivity, and failure of counterregulation (2).
glycemic control improves in 90% of patients after RYGB These complex side effects make it challenging for the treat-
(277). Short- and medium-term studies show that VSG is ing clinician and more importantly for the suffering patient
almost as effective as the RYGB with respect to short- to as they often persist in the long term and can thus cause
medium-term improvements in body weight loss and glyce- reduced quality of life.
mic control (1, 139, 145, 150, 225, 226, 254, 287). Bariat-
ric surgery also leads to improvement or remission of other Nutritional deficiencies occur in 30 –70% of patients after
obesity-related comorbidities such as hypertension, ob- bariatric surgery (123). Protein, iron, folate, calcium, and
structive sleep apnea, musculoskeletal pain, and overall vitamins B1, B12, and D are the most affected macro- and
quality of life (194, 211, 252, 254). micronutrients (14). Nutrient deficiency when severe can
lead to symptoms of edema, hypoalbuminemia, anemia,
Bariatric surgery does come with some unwanted conse- and hair loss (protein) as well as peripheral neuropathy
quences, making the decision to opt for this treatment a (folate, B12), Wernicke encephalopathy and beriberi (B1),
matter of the risks versus benefits on the balance for any metabolic bone disease (vitamin D, calcium), and anemia
particular individual. Around 4% of patients that undergo (iron) (14). Therefore, the quality of food consumed and
bariatric surgery have surgical complications within 30 nutritional monitoring are a critical part of the postsurgical
days of the operation, with the most common being bleed- management of patients. Lifelong multivitamin supplemen-
ing, perforation, or leakage (276). Later surgical complica- tation is also essential (232).
tions can also occur in 15–20% of patients; these include
small bowel obstruction, anastomotic stenosis, or marginal C. Set-Point Theory
ulceration (108). Both early and late surgical complications
can be diagnosed and treated with a surgical or endoscopic Despite the effectiveness of bariatric surgery as a means of
intervention. substantially reducing body weight over a relatively short
period of time, further weight loss to achieve the “ideal”
Medical complications can also occur after bariatric sur- body weight for aesthetic reasons often proves challenging.
gery and are sometimes more nuanced in terms of diagnosis The new stable body weight profile achieved by 12–18 mo
and treatment due to the complex and on occasion occult after bariatric surgery often appears to be “defended” with
nature of the etiology. Abdominal pain (particularly unex- the same vigor, as was the elevated body weight was before
plained abdominal pain) and hypoglycemic episodes in pa- bariatric surgery. Set-point defense theory is based on the
tients without diabetes are common and “not yet fully un- idea that body fat before and after bariatric surgery is main-
derstood” negative consequence. Abdominal pain is the tained through homeostatic systems around a “set point.”
main complaint of half of the emergency hospital admis- Certain schools of thought suggest that intrinsic adjust-
sions after RYGB (54). The pathogenesis varies widely from ments to food intake and energy expenditure can occur with
behavioral and nutritional disorders, functional disorders, the purpose of maintaining a genetically pre-engineered
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1115
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
body fat set point in response to short-term fat gain or fat The peptide hormone releasing enteroendocrine cells in the
loss (44, 138, 171, 207, 238, 326). small intestine are classified according to a nomenclature
that differentiates between cell type according to discrete
A framework that incorporates this set-point theory is con- patterns of hormonal secretion. Recent evidence suggests
ceptually compelling as a means of understanding the con- that there is significant dynamic plasticity in the expression
sistent and resilient changes in body fat after bariatric sur- and release of enteroendocrine peptide hormones across the
gery as it implies that patients move to a new steady state recognized cell types. Plasticity permits adaptive changes in
characterized by a lower body fat set point. Many funda- hormone profile to occur as a function of dynamic change in
mental physiological questions still surround this theory. the surrounding environment, e.g., dietary nutrient compo-
What physiological parameter serves as the sensor to poten- sition, changes in relative anatomical position after surgery
tial deviations from set point, what structure(s) serves as the (127).
detector(s), and what system/systems are operative in de-
fending set point? Is set point really adjusted by bariatric
Cholecystokinin (CCK) is released from the I cells of the
surgery and could the process be mimicked nonsurgically?
upper intestinal enteroendocrine cells within minutes of
meal initiation (172). CCK was the first gut peptide estab-
All of these questions provide an ideal philosophical gate-
lished to have physiological relevance as an inhibitory sig-
way into the main topic of the present review, which seeks
nal to further food intake (114), and its role as a short-term
to delineate the role of changes in eating behavior as an
input into body fat set-point resetting after bariatric sur- meal-reducing signal has been extensively documented in
gery. mammalian species including humans (284).
Other prandial and postprandial signals are also generated
IV. BIOPSYCHOLOGY OF HUNGER, when nutrients are absorbed from the small intestine into
SATIATION, AND SATIETY the peripheral circulation. Those signals are vital in the
regulation of satiation and satiety processes. Insulin is re-
A useful first stop in the journey towards a comprehensive leased from the pancreas during the cephalic phase (pre-
description of what we know about changes to eating be- prandial) and peaks after the initiation of the meal to regu-
havior after bariatric surgery is a review of the biopsycho- late the absorption of glucose into the bloodstream. Glu-
logical framework of hunger and satiety. Hunger, the first cose is then carried to the brain to modulate the function of
phase of the satiety cascade, is defined as the urge to seek a variety of neurotransmitters and peptides associated with
and consume food, which triggers a feeding episode. The appetite regulation (135). The liver also plays a major role
behavior that terminates an eating episode is referred to as in metabolizing glucose, fatty acids, and amino acids (9).
satiation, whereas the process underpinning the transitional Hepatic energy metabolism generates satiety signals (9)
period between meals is referred to as satiety (30). transmitted from the liver to the central nervous system
(CNS) via the vagus nerve (135).
Hunger is driven by preprandial cognitive and sensory sig-
nals that promote food intake and prepare the body for A number of satiety peptides are released from the enteroen-
digestion (30). Preprandial signals are generated in part by docrine cells and peak after meal termination to sustain
hunger hormones such as ghrelin (69), hedonic stimulation satiety until the initiation of the next eating episode. Peptide
(the reward system), cognition and learned experiences
YY (PYY), glucagon-like peptide 1 (GLP-1), and oxynto-
(e.g., memory of last meal, meal times), and also by sensory
modulin (OXM) are released from the L cells in proportion
stimulation (e.g., sight and smell of food) (300). Once food
to the amount of calories consumed and meal composition
is present in the oral cavity, and during the early phase of an
(61, 74, 105). These hormones regulate short-term energy
eating episode, further hunger signals are generated by sen-
sory stimulation caused by the contact of food with taste balance. Leptin, on the other hand, is released from the
buds in the mouth (134). adipose tissues in proportion to body fat (179) and from the
gastric mucosa (281) to regulate long-term energy balance
During the meal (prandial phase), gastric distension caused (63). Similarly, insulin is also released in proportion to ad-
by the presence of food in the stomach is sensed by mecha- ipose tissues (229), and the brain interprets its levels to
noreceptors to detect the quantity eaten (188, 228) and adjust food intake accordingly (329).
signals are sent to the brain via the vagus nerve (23). When
chyme enters the small intestine, intestinal mechano- and It is important to highlight the fact that the short- and
chemoreceptors detect the quantity and quality of nutrients long-term signals modulate each other’s physiological func-
and send signals also via the vagus nerve to the nucleus tions. For instance, leptin stimulates GLP-1 secretion from
tractus solitarius (NTS) to alter the gastrointestinal motor, the L cells, and leptin resistance is associated with impaired
stimulate local peptide release, and activates vagal efferent secretion of GLP-1 (11). In addition, leptin may enhance the
fibers (182). CNS response to some gut hormones as suggested by Mor-
1116 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
ton et al. (206). Many other hormonal interactions take and soft food for a further period before proceeding to
place, but they are beyond the scope of this review. “normal food.” By 3 mo, patients are encouraged to eat a
normal diet. Humans and animals are able to compensate
FIGURE 2 shows an integrated diagram of the biopsychology for smaller meal sizes after surgery by increasing meal fre-
of hunger, satiation, and satiety. quency (36, 163, 339). Despite the small size of the gastric
pouch in RYGB, there is usually little restriction as the
V. EATING BEHAVIOR AFTER BARIATRIC stoma between the gastric pouch and the small bowel is
SURGERY wide. High pressure manometry suggests normal pressures
in the esophagus, low pressures in the pouch, and higher
Clinicians ask patients after bariatric surgery to follow a pressures in the small bowel, indicating no restriction at the
staged progression diet consisting of a liquid diet for the level of the pouch (29). This allows food to progress from
first few days or weeks, pureed diet for several more weeks, the esophagus rapidly into the small bowel. The small
Cortex
Hypothalamic
Nuclei
Neuronal signals
NTS
gus
Va
STOP GO
CCK
Physiological signals
Ghrelin
Leptin Insulin
PYY
Metabolic demand
(Hunger) GLP-1
OXM
Psychological signals
Cognitive Oro-sensory
(sight, smell, texture)
Cognitive Pre-absorptive
Sensory Post-absorptive
Food
Early Late
Pre-prandial motivation Satiation Satiety
FIGURE 2. Biopsychology of hunger and satiety. Hunger, stimulated by cognitive or sensory factors, initiates
an eating episode, which in turn terminates when satiety is reached. During the meal, short-term energy
regulation signals including gut hormones are sent from the stomach and small intestine to the brain. Leptin
is secreted from the adipose tissues and insulin from the pancreas in proportion to body fat to regulate
long-term energy balance. All these signals are integrated in the brain to regulate food intake.
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1117
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
pouch does not cause restriction but rather may act as con- nism, and the body can no longer respond to elevated en-
duit to accelerate food into the small bowel. The small dogenous leptin levels. After weight loss, body fat reduces
bowel then requires adaptation to cope with the sudden and leptin levels decrease, initiating an anti-starvation
delivery of undigested food, and consequently gut adapta- mechanism with increased hunger. This hunger drive is part
tion may occur. of a homeostatic balance that tries to draw the body fat
back to its predieting set point or even higher, often raising
Patients after RYGB and sleeve gastrostomy sometimes re- the set point higher each dieting attempt (178).
port a shift away from consuming high-fat and high-sugar
products to healthier options. Despite reporting a reduced After bariatric surgery, patients describe having lower hun-
liking for foods like chocolates, sweets, and fried food, it ger levels and more postprandial fullness (165, 181, 204),
has remained unknown whether this reflects a conscious which leads to a significant negative energy balance and
avoidance based on advice, expectations, or assumed re- thus weight loss. However, energy balance stabilizes ~1 yr
sponsibility; changes in taste and palatability; conditioned after bariatric surgery (152, 200) but weight does not go
avoidance; conditioned aversion; or a change in food pref- back to the baseline levels (1, 53, 139, 145, 150, 214, 225,
erences due to an yet undefined other mechanism. 226, 254, 275, 287) and seems to be protected by a new
body fat set-point level (132) (FIGURE 3).
We speculate that immediate and short-term phases of food
intake after bariatric surgery are critical to the shaping of Verbal report using Visual Analogue Scales (VAS) is the
long-term changes in food intake and preferences in a sim- most common method of assessing hunger and fullness. le
ilar way to early infancy food exposure. Bariatric surgery Roux et al. (168) used VAS in patients after RYGB to assess
“resets” the set point of eating behavior in a similar manner changes in appetite in as early as 2 days postoperation.
to the set point for body fat. Ratings of hunger reduced to half while ratings of fullness
doubled. Both were maintained up to 42 days (75). This
A. Hunger and Fullness was consistent with other findings (48, 165, 204, 296). On
the other hand, Laurenius et al. (163) did not find a signif-
After a period of dieting and successful weight loss, the icant effect of RYGB surgery on the perception of hunger
subcortical areas of the brain, particularly the hypothala- before the meal, satiation after the meal, or maintained
mus and hindbrain (22, 149, 328), respond to weight loss satiety 1 h after a meal at any time point for up to 2 yr
with a compensation reaction consisting of “but not limited postoperation. However, in their study two different meal
to” increased hunger and reduced fullness signals (12, 51, sizes were used to accommodate the changes after sur-
71, 83, 84, 86, 294). Exogenous leptin given to rodents gery (163). Thus in the same study, when ad libitum meal
leads to reduced hunger levels and food intake. Leptin re- was assessed, RYGB patients had a significant reduction
sistance in obese people causes a disruption in this mecha- in meal size which resulted in the same level of satiety as
FIGURE 3. Influence of weight loss interventions on body fat set point. During a conventional diet therapy,
weight decreases during negative energy balance. When the diet is stopped, weight gradually increases and is
pulled back to the pre-diet set point or even higher, raising the set point during each dieting attempt. With
bariatric surgery, the set point is reset to be 20 –30% lower. Therefore, during stable energy balance, the
weight fluctuates around the “new” set point.
1118 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
compared with presurgery (163), which supports the no- C. Frequency
tion that surgery results in the same level of satiation but
it only occurs with far fewer calories. Other studies also Bariatric procedures were originally designed to reduce the
confirmed similar levels of satiety using VAS post-RYGB size of the stomach in an attempt to cause restriction and
while subjects were losing weight (157), suggesting pa- induce weight loss, but most studies confirm that restriction
tients were not feeling deprived or hungry even while does not play a role in long-term weight loss maintenance.
they were losing weight secondary to being in a very steep Furnes et al. (112) suggested that the weight loss observed
negative energy balance. after VSG is independent of the food reservoir function of
the stomach. In addition, Wilson-Pérez et al. (325) hypoth-
Sleeve gastrectomy (SG) in some studies has been shown to esized that were VSG to result in reduced portion sizes due
reduce hunger and enhance postprandial fullness compara- to the reduced gastric size, then patients would develop a
ble to RYGB (312, 334). Differences between RYGB and compensatory adaptation by increasing fat intake to maxi-
BAND were assessed by Konor et al. (158) who demon- mise caloric intake. Wilson-Pérez et al. (325) used a rat
strated that RYGB produced higher levels of satiety at 3 h model of VSG and found that rats after VSG not only re-
post-meal ingestion as compared with BAND or subjects strict their food intake but also preferred less calorically
who were unoperated and overweight. dense foods. In addition, despite the markedly different sur-
gical manipulations, rats after VSG and RYGB had remark-
ably similar changes in food choices, i.e., less fat and more
B. Food Volume carbohydrates when compared with sham-operated rats
(325). This suggests a common underlying mechanism in
both procedures. Both procedures result in accelerated nu-
The first objectively quantifiable change after bariatric sur-
trient transfer to the small intestine, and this may be the
gery is the reduced volume of food consumed in one eating
decisive factor.
episode. Human studies are still limited in providing evi-
dence on meal size, but all the available studies are in sup- Patients after RYGB were followed for 2 yr to assess meal
port of positive change. Our research group has recently patterns using verbal report. Number of meals per day was
demonstrated that VSG changes eating behavior and, spe- reported to significantly increase from 4.9 meals/day pre-
cifically, reduces ad libitum meal size, meal duration, and surgery to 5.8 meal/day 1 yr after the operation and to
rate of eating (unpublished work). Similarly, Laurenies et decreased back to the baseline number at 2 yr after the
al. (163) showed that following RYGB meal size becomes operation (5.4 meals/day). The significant change only oc-
significantly smaller. Six weeks after surgery, RYGB pa- curred during the morning meals. Postoperatively, there
tients consume only 42% of the preoperative meal size. was a trend for patients to consume fewer meals at night
After 1 and 2 yr, the meal size increases to 57 and 66% of (163). Increased frequency of meal consumption was in line
the preoperative meal size, respectively (163). Using an ad with the animal data (36, 339).
libitum buffet meal targeting direct behavior, Mette et al.
(212) suggested that the reduction in total calorie intake Increasing the frequency of meals can be a natural compen-
measured 6 mo post RYGB and SG surgery was explained satory reaction, but it can also be a conditioned learned
solely by the reduction in portion size and not by energy behavior to control the unpleasant postprandial physiolog-
density or food choices. Animal studies are important to ical signals that occur after bariatric surgery. Five years
support the evidence due to the confounding effect of after RYGB, patients described going through a “learning”
social factors of wanting to lose weight after surgery in phase during the first year to learn new eating habits includ-
human studies. After RYGB, rats reduce their intake of ing eating smaller and more frequent meals (173). The in-
both liquid and solid diets in the acute and chronic phases crease in frequency of meals do however not compensate for
(339). Two other studies showed positive changes but the calorie deficit patients maintain as would have been
were not conclusive. One study reported strong trends expected if the procedures relied on restriction of the meal
for decreased meal size (⫺30%), but the results did not size only.
reach statistical significance (112). In the only other
study, chow meal size was significantly reduced 5–10 D. Calorie Intake and Energy Density
days but not 11–19 days after RYGB (330). More re-
cently, Mathes et al. (187) supported those findings by Patients after bariatric surgery do not only consume smaller
showing not only a reduction in total daily calorie but portion sizes as previously discussed but consume less total
also from calories consumption from all individual ma- calories per day. In the first few weeks after the operation,
cronutrients from a cafeteria diet, suggesting reduced the postoperative diet generally provides 500 – 800 kcal/
portion sizes. It is important to bear in mind methodolog- day, resembling a very-low-calorie diet. The calorie intake
ical variations where results are apparently contradic- increases gradually between 3 mo to 1 yr from an average of
tory. 800 to 1,000 kcal (152, 200). Total calorie intake increase
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1119
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
gradually up to 5 yr postoperation but remains lower than patients after RYGB reported a significant decrease in des-
the preoperative values, albeit not significantly different serts, cookies, and candies consumption, but an increase in
(199). fruits and vegetables. Avoidance of foods containing fat
was also documented for the RYGB group (217). le Roux et
Dietary energy density (DED) is the amount of kilocalories al. (166), using the same methodology and set of patients,
per gram of food (kcal/g) (93). Fat is the biggest influence on showed a decrease in reported preference for fat 6 yr after
DED due to its high energy content, which is more than RYGB in comparison to patients having VBG. Ernst et al.
protein and carbohydrates (9, 4, and 4 kcal/g, respectively). (96) also studied a group of patients who reported a reduc-
On the other hand, water containing foods such as fruits tion in consumption of desserts such as chocolates, cakes,
and vegetables have low DED (118). The consumption of and cookies and an increase in intake of vegetables, poultry,
larger volumes of food without increasing total calorie in- and protein-rich foods such as fish and eggs. Primeaux et al.
take has been shown to affect feelings of fullness (163) and
(235) again used verbal report by deploying a Food Prefer-
may lead to better weight loss outcomes (93, 169, 245).
ence Questionnaire and VAS comparing VSG to RYGB and
After bariatric surgery, DED also decreases significantly
found that VSG decreased the hedonic rating of most ma-
from 1.07 to 0.78 kcal/g at 6 wk and 0.90 kcal/g and
cronutrient profiles as opposed to RYGB, after which
0.96 kcal/g after 1 and 2 yr, respectively. DED does not
changes were more selective. Caution is needed in assessing
correlate with percentage weight loss at any time point
(164). However, viewing the change in calories 5 yr post- these results because follow-up was restricted to 1–3 mo
operation within the context of patients having lost and and the sample size was small. Postoperative diet changes
maintaining 20 –30% body weight loss patients are con- dramatically within 3 mo, and this could affect the interpre-
suming much less than expected, were they to be experienc- tation of the results (280).
ing a physiological drive to reestablish body fat at the pre
operative set point. In contrast, a number of other studies have reported no
changes in food preference after RYGB and VSG. A retro-
spective cross-sectional study compared food intake and
E. Food Preferences food preferences over 1 yr, and patients reported no differ-
ence in dietary intake and food preferences between RYGB
Changes in DED after surgery necessarily imply changes in and VSG groups (90). This agrees with the longest fol-
the type of food eaten. Halmi et al. (130) were the first to low-up study of 5 yr also comparing VSG and RYGB (199)
suggest that gastric bypass causes a change in macronutri- where patients reported the percentages of macronutrients
ents selection as patients reported they consumed fewer were not significantly different between the two surgical
calorically dense and carbohydrate-rich foods. These re- groups (199).
sults led other researchers to investigate the effect of bari-
atric surgery on food preferences and macronutrient con- Other studies also report that bariatric surgery does not
sumption. Halmi’s results on RYGB were supported over lower consumption and preference for sweet and fatty
the years by other short-term studies (34, 67, 152, 161, 201, foods. A study by Troslter et al. (306) found the opposite
293) and even studies up to 8 yr after RYGB (161). Most of with an increase in fat and decrease in protein intake after
these relied on verbal report. Another recent 2-yr follow-up surgery, while Bavaresco et al. (19) studied patients who
study carried out by Coluzzi et al. (62) assessed changes in reported an overall decrease in intake of all three macronu-
food intake associated with changes in taste again using
trients (carbohydrates, lipids, and protein), with no specific
verbal reports. Six months after surgery, daily caloric intake
preference to any macronutrient after surgery.
reduced by 68% and the reduction was maintained for 24
mo. In addition, 75% of the patients reported a change in
The major limitation is that most human studies rely on
taste associated with reduced interest in sweets, high-fat
indirect verbal reporting which have high risk of underre-
food, and alcoholic drinks (62). As VSG is becoming more
popular, studies on its effect on food preferences are now porting particularly as bariatric patients are asked by mul-
also becoming available. Ammon et al. (7) used verbal re- tiple healthcare professionals to eat less fat and sugars. An-
port by implementing a Food Preference Questionnaire and imal studies allow us to examine changes in food prefer-
VAS to assess changes in preference for different types of ences without being the confounding factor of social
food varying in their macronutrient composition 6 wk after pressure. Interestingly, animals behave similarly to many
VSG and found postoperative hedonic ratings decreased for of the reports from humans after RYGB. Bueter et al. (38)
foods high in fat and carbohydrate content. and le Roux et al. (166) used two-bottle preference test
and found a significant reduction in the consumption of
When comparing RYGB with BAND or vertical banded fat and sugar solution compared with sham-operated
gastroplasty (VBG), Olbers et al. (217) used verbal report rats. Rats after RYGB also showed an increased prefer-
by implementing the SOS (Swedish Obese Study) question- ence for a vegetable drink over low-sucrose and low-fat
naire to compare RYGB and VBG at 1 yr postsurgery. The liquids as demonstrated by Seyfried et al. (265).
1120 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
Furthermore, when rats after RYGB were presented with a
solid diet, an initial increase in preference for the high-fat
chow was observed, which then decreases to 51% of that
seen in sham-operated rats (249). This suggests the exis-
tence of an underlying mechanism for the “conditioned” Food frequency
shift in the chow preference. Mathes et al. (187) assessed the Postprandial discomfort
Fullness
preference for diets consisting of different macronutrients
composition, using a cafeteria study. The results indicated a
progressive reduction in the proportion of calories from fat,
but despite this dietary shift to lower fat consumption after
RYGB, both the RYGB as well as sham-operated rats con-
tinued to select the majority of their calories from the high- Food Intake after bariatric surgery
fat/high-sugar options (187). This is an important outcome
leading to the hypothesis that changes in food preferences
after RYGB may not result of the hedonic value of food
after RYGB, but rather influenced by learning that too
much fat may have negative visceral consequences. Food volume
Energy density
The only human study that tried to mimic the rigorous Calorie intake
experimental protocol in rats found that 6 mo after RYGB Hunger
and VSG humans consumed 50% fewer calories when of-
fered a buffet lunch, but that the macronutrient composi-
tion of these meals was similar to before surgery. An impor-
tant difference between the rodent and human cafeteria diet
FIGURE 4. Changes in food intake after bariatric surgery.
or buffet meal studies was that the rodents were tested when
they were weight stable, while the humans were still in a
negative energy balance and thus the humans were eating so
few calories that they may not have triggered the threshold We progress through satiation as our gut signals accumu-
where negative visceral consequences would necessitate late and indicate increasing loading with energy and nutri-
them to reduce the proportion of fat in their diet. ents. However, hedonic responses accompanying certain
foods can override the signal to terminate intake that arises
FIGURE 4 presents the direction of change of food intake even with complete satiation.
after bariatric surgery.
A. Mechanisms That Explain Reduction in
VI. MECHANISMS OF CHANGED EATING Calorie Intake
BEHAVIOR
1. Hypothalamic and nucleus tractus solitarius
Food intake is an innate behavior regulated by two comple- signaling
mentary drives, the homeostatic and hedonic pathways
(251). The homeostatic pathway controls energy balance by In the hypothalamus, the arcuate nucleus (ARC) is the main
increasing the motivation to eat following depletion of en- region involved in the homeostatic control of food intake
ergy stores or alternatively meal termination in response to (258). Within the ARC, two groups of neurons are promi-
physiological satiation signals (27). In contrast, hedonic or nently implicated in the regulation of feeding. One group
reward-based regulation is related to the sight, smell, and localized more laterally in the ARC coexpress anorexigenic
taste of food, along with emotional and social factors, all of (appetite suppressant) neuropeptides, i.e., cocaine- and am-
which integrate to impact on food intake (27). The hedonic phetamine-related transcript (CART) and proopiomelano-
pathway can override the homeostatic pathway during pe- cortin (POMC) (311). The second group of neurons cluster
riods of relative energy abundance by increasing the desire more medially in the ARC, coexpressing orexigenic (appe-
to consume foods that are highly palatable (27). tite stimulant) neuropeptides, i.e., neuropeptide Y (NPY)
and agouti-related protein (AgRP) (311). Neuronal projec-
Satiation is the process that culminates in termination of an tions from the ARC then communicate with other key hy-
eating episode and is achieved by prandial and postprandial pothalamic regions, such as the paraventricular nucleus,
signals that are generated when nutrients are absorbed from dorsomedial nucleus, and ventromedial and lateral hypo-
the small bowel into the peripheral circulation (30). Satia- thalamic nuclei (205, 311). The ARC has an incomplete
tion is an unconditioned behavior; it cannot be controlled blood-brain barrier that allows direct nutritional informa-
by the taste of food or whether the food is rewarding or not. tion from the periphery to be sensed as well as indirect
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1121
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
peripheral markers of ingestive physiology such as insulin, release is not observed after BAND which appears to rely on
leptin, and gut hormones to gain access to the signaling pressure on the IGLES and vagal signaling to reduce hunger
pathways that regulate appetite in the ARC (193). In addi- (165).
tion, the vagal nerve transmit peripheral signals produced in
the gastrointestinal tract to the nucleus of the tractus soli- Similarly to PYY, GLP-1 is also secreted by the L cells of the
tarius (NTS) in the brain stem where signals then integrate small bowel in response to a meal to decrease food intake
with those of the hypothalamus to control appetite (253). through its effects on the hypothalamus and brain stem
(295). Its physiological function on food intake and blood
Enhanced hypothalamic and NTS signaling has been pro- glucose has been postulated to be through its effect on gas-
posed as an underlying mechanism for the reduced appetite tric emptying, glucagon release, and secretion of insulin
and thus weight loss after bariatric surgery. Interestingly, from the pancreas (incretin effect) (248). Despite the phys-
despite the reduced food intake and body weight of differ- iological benefits of GLP-1, on its own it is not good enough
ent bariatric procedures, the majority of studies found an to explain all the effects of bariatric surgery (331), suggest-
upregulation of NPY and AgRP and unchanged POMC ing the appetite change after bariatric surgery is a result of a
levels (16, 208, 318). Stefater et al. (287) found unchanged synergistic response of multiple gut hormones (233).
NPY and AgRP expression after VSG in rats. However,
AgRP increased in pair-fed rats (287), suggesting that the 3. Bile acids
calorically restricted rats were hungry and the VSG rats
were not (198). Another study by Romanova et al. (246)
observed lowered levels of NPY 10 days after RYGB and in As far back as 1968, controlled studies of administration of
pair-fed controls compared with sham surgery. These ap- bile acids indicated that elevated circulating bile acids could
parently contradictory findings may relate to differences in suppress food intake (32). The physiological handling of
study periods examined (i.e., an acute vs. a chronic setting) bile acids in the small bowel has in more recent times been
or differences in transcriptional processing between the end linked to appetite and metabolic control through recogni-
point used as surrogates of orexigenesis (16). Barkholt et al. tion that bile is a potent endogenous stimulant of the endo-
(16) investigated the effect of RYGB on second-order crine L cell, liberating the satiety gut hormones PYY and
downstream orexigenic melanin-concentrating hormone GLP-1 (230). In humans, postprandial bile acids are posi-
(MCH) mRNA expression finding that RYGB but not pair- tively correlated with the circulating levels of some anorex-
fed rats had blunted MCH expression in the lateral hypo- igenic gut hormones (GLP-1 and PYY), but negatively cor-
thalams. This suggests that RYGB surgery puts a “brake” related with the orexigenic gut hormone (ghrelin) (242).
on orexigenic hypothalamic output signals as the hunger Bile acids can engage and activate the nuclear farnesoid X
signals arising from the ARC do not translate into sensa- receptor (FXR) and cytoplasmic G protein-coupled BA re-
tions of hunger nor into food-seeking behavior, potentially ceptor TGR5 (314). The activation of TGR5 in the gut
due to a reduced mesolimbic dopaminergic neurotransmis- stimulates the release of GLP-1 and PYY (15). On the other
sion (16). hand, activation of FXR by bile acids promotes the release
of fibroblast growth factors FGF19 and FGF21 (57). FGF21
2. Gut hormones mediates simple sugar consumption by reducing the appet-
itive behavior towards sweet food (315).
Bariatric surgery involves a profound anatomical change to
the gastrointestinal tract (247, 263), which causes a more Following gastric bypass, the levels of total plasma bile acid
rapid delivery of nutrients to the distal small bowel (49, are elevated (225); this is postulated to be due to the ana-
192, 313). As a result, gut adaptation facilitates an exag- tomical changes causing a prompt supply of undiluted bile
gerated rise in a number of peripheral satiety hormones to reach the distal L cells and activating the TGR5 recep-
including PYY and GLP-1, and reduced rise of the hunger tors. Bile acid metabolism is also markedly changed after
hormone ghrelin occurs within days after bariatric surgery RYGB, due to changes in bacteria-driven transformation
(70). Those hormones have receptors in the peripheral sys- and deconjugation and changes in hepatic extraction of
tem and in the CNS forming a gut-brain hormonal axis. recirculating bile acids (111). Primary bile acids are synthe-
sized and conjugated in the liver (87) and then deconjugated
PYY is released from the L cells of the distal small bowel and dehydroxylated to secondary bile acids by the gut mi-
after a meal in proportion to the consumed calories (18). crobiota when exported to the small intestine (52). Signifi-
After bariatric surgery, the postprandial levels of PYY are cant increases in the 12␣-hydroxylated/non-12␣-hydroxy-
elevated and the new levels correlate with the postoperative lated bile acid ratio have been described after RYGB. Cir-
weight loss (79, 191). The importance of PYY in the regu- culating bile acid profiles are not altered after BAND (156,
lation of feeding after RYGB has also been investigated 223, 230, 273) as there is no change in the pathway of
using octreotide, which blocks the release of most of the gut nutrients reaching the small bowel. In the normal anatomy,
hormones in humans and rats and, not surprisingly, in- bile acids are diluted and mixed with chyme and therefore
creases food intake (103, 115, 168). Exaggerated hormonal are less likely to stimulate L cells for peptide secretion. VSG
1122 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
does however also cause elevations in the levels of bile acids Liou et al. (174) have examined whether changes in the gut
possibly due to the increased gastric emptying (288). microbiota after RYGB are conserved across rodents and
humans and whether transplantation of RYGB modified
4. Gut microbiota microbiota can confer a transferable weight loss effect on
recipients. With the use of the diet-induced obesity-suscep-
tible C57BL/6J strain of mice a decrease in body weight of
Gut microbiota contributes to many physiological func- 30% was observed by 3 wk after RYGB. Food intake did
tions such as the production of short-chain fatty acids not differ between GB and SHAM groups, but increased
(SCFAs) (177), neurotransmitters (68), and regulation of fecal calorie loss occurred in the GB group signaling energy
gastrointestinal hormones (80, 143), which has led some wasting. Principal component analysis revealed that distal
researchers to consider it as a virtual organ on its own (58, gastric, ileal, cecal, and colonic microbiota were strongly
99, 107). modified by RYGB. Unique changes after RYGB not seen
after matched nonsurgical weight loss included increases in
The interest in the role of gut microbiota in the development Enterobacteriales and higher Verrucomicrobiales. Three
of obesity started with findings of intestinal bacterial colo- phylum level increases predominated in Bacteroidetes, Ver-
nizations that aid energy conversion into body fat (308). rucomicrobia, and Proteobacteria, with resolution to the
Bäckhed et al. (13) showed that germ-free (GF) mice can genus level of Alistipes, Akkermansia, and Escherichia. Re-
consume a higher number of calories but remain leaner than cipient lean, germ-free mice inoculated with cecal contents
conventionally raised mice. Moreover, transferring the mi- from RYGB-operated animals had reductions in adiposity
crobiota from conventionally raised mice to GF mice causes not seen after transplantation of microbiota from animals
a sharp increase in body fat even with low food intake (13). that had undergone food restriction-driven weight loss.
Phylogenetic analysis of gut bacteria of three human groups Shotgun sequencing of the human fecal metagenome to
(healthy weight, obese, and post-RYGB) showed six main functionally analyze the gut microbiota of weight-stable
bacterial phyla to be present. The majority of the bacterial women 9 yr after RYGB was conducted by Tremaroli et al.
sequencing were among Firmicutes and Bacteroidetes, with (305) and was coupled to human-mouse microbiota trans-
the rest distributed among Proteobacteria, Actinobacteria, plantation experiments. An increased presence of Gamma-
Fusobacteria, and Verrucomicrobia. Those bacterial phyla proteobacteria was notable after RYGB, while lower levels
are distributed differently in the intestines of the study within the Firmicutes phylum of Clostridium difficile, Clos-
groups. Prevotellaceae and Erysipelotrichaceae subphylum tridium hiranonis, and Gemella sanguinis were recorded
of Bacteroidetes and Firmicutes, respectively, are mostly after RYGB. Conversely, facultative anaerobes within Pro-
abundant in obese individuals; in fact, Prevotellaceae is teobacteria (Escherichia, Klebsiella, and Pseudomonas)
only found in obese individuals and is considered “obese were increased in relative abundance in RYGB recipients.
specific.” In contrast, Fusobacteria and the family Entero- Metabolomic comparisons revealed a decrease in SCFA/
bacteriaceae within Proteobacteria were found only in the branched-chain fatty acid ratio after gastric bypass, indicat-
RYGB group. This suggests that after bariatric surgery, par- ing increased amino acid fermentation. Genetic signatures
ticularly RYGB, the profile of the microbiota is substan- for microbial enzymes involved in the generation of second-
ary bile acids were increased and correlated with shifts in
tially altered (336). A recent meta-analysis study by Magou-
the ratio of secondary to primary bile acid profiles occurring
liotis et al. (180) reviewed 22 studies and 562 patients who
in recipients of RYGB microbiota, suggesting altered bile
underwent different bariatric procedures. Despite finding
acid profiles may participate in reductions in adiposity after
considerable variation in the documented bacterial species
surgery.
in different studies, the overall findings also support a post-
operative shift of the gut microbiota (180). This alteration
in abundance and diversity of gut microbiota is speculated B. Mechanisms That May Explain Reduction
to cause the shift in bile acid composition discussed above. in Calorie Density of Food
The mechanisms behind altered gut bacteria are not com- Humans and animals have innate preferences for nutritive,
pletely understood, but a role of the new dietary macronu- calorie-dense food that provide them with the essential en-
trient composition, anatomical manipulations that change ergy (259). Their biological system, however, is geared to-
the levels of oxygen in the intestines, and pH and bile flow, wards learning when consumption causes postingestive
have been suggested. On the contrary, alteration in gut malaise, and subsequently these foods may be remembered
microbiota may not be a result of weight loss after bariatric as harmful or “not good” for subsequent meals (259). After
surgery, but rather a cause of weight loss. An emerging bariatric surgery, food containing fat and simple carbohy-
concept suggests that metabolic regulation starts from the drate may be labeled as “not good” due to negative
gut and then sends signals to the brain, and other endocrine postingestive sequelae. This can result in altered food pref-
organs (104). erences observed after bariatric surgery as described in sec-
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1123
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
tion IVD. The mechanism behind this alteration is postu- increased total food intake with no specific changes in food
lated to be due to visceral signals and changes in taste func- selection or preference (59).
tion.
Orexin neurons (A and B) are activated in anticipation of
1. Neural and hormonal signals palatable food rewards (133), illustrating the ability of the
orexin system to respond not only to internal energy bal-
A) NEURAL SIGNALS. Similar to satiety regulation, macronutri- ance cues but also to external environmental cues linked to
ent preferences are also controlled by neural and hormonal the cognitive aspects of feeding and food reward behaviors.
signals as part of the food intake regulation system. This On that basis, Clegg et al. (59) demonstrated that central
section will summarize the available literature on the effect administration of orexin-A in rats prompted rats to choose
of neuropeptide and hormonal peptide on food choices. a high-fat diet instead of a low-fat one, suggesting a role of
orexin-A in controlling food selection.
Evidence from pharmacological and genetic data suggests a
role of POMC in eating behavior, particularly dietary fat The endocannabinoid system also plays a role in food
consumption. Tung et al. (307) found that POMC genotype choices (220). The cannabinoids [anandamide (AEA) and
was a strong predictor of dietary fat preference with POMC 2-arachidonoylgycerol (2-AG)] are important carriers of
null mice choosing to eat approximately twice as much fat, metabolic information between the CNS and the periphery
but similar amounts of carbohydrate and protein compared (78). Within the reward circuitries, they interact with opi-
with wild-type mice. Human studies validating this infor- oid and dopaminergic systems to enhance satisfaction com-
mation are scarce. However, a genome-wide scan based on ing from the ingestion of palatable food (220). Pérez et al.
data derived from food questionnaires collected from Mex-
(98) used intraperitoneal injection of the CB1 receptor ag-
ican-American families suggested that human chromosome
onist N-(2-chloroethyl)-5Z,8Z,11Z,14Z-eicosatetraen-
2p22, which is a region containing POMC, was linked with
amide (ACEA) in rats and showed increased ingestion of a
increased saturated fat intake in those families (45).
carbohydrate diet but not fat or protein. Rimonabant, a
selective CB1 receptor antagonist, was a medication devel-
As with most neuropeptides, studies on food choices are
oped for the treatment of obesity but withdrawn later from
limited and, therefore, the effect of CART on food selection
the market due to its adverse effects, which included anxi-
is not yet determined. Deletion of the CART gene in mice
ety, depression, and suicidal ideation (56, 203). In a func-
did not cause a change in sweet preference compared with
tional magnetic resonance imaging (fMRI) study of healthy
wild-type mice, suggesting that either CART peptides do
not modulate food preference or that compensatory normal-weight volunteers, rimonabant was shown to alter
changes in CART gene modified mice have obscured this the brain activation of key reward areas towards the sight
phenotype (66). and smell of rewarding foods (144). Direct measures of
food preferences in rimonabant-injected rats also showed
Orexogenic neuropeptides may play a more significant role supporting findings of reduced preference (186, 236) and
in food choices. AgRP-regulated appetite is affected by the motivation to palatable food choices (274).
opioid pathways, in which the hedonic and reward aspects
of feeding are implicated. Naloxone, a nonselective opioid TABLE 1 summarizes the effect of appetite neurotransmit-
antagonist, blocks AgRP-induced feeding (128, 159). Acti- ters on changes in food preferences.
vation of the opioid system, in turn, has been associated
with increased intake of preferred, high-fat-containing diets B) HORMONAL SIGNALS. Long- and short-term peripheral satiety
(337). Consistent with this, Hagan et al. (128) found that hormones also impact food preferences. However, the im-
AgRP selectively increases the intake of a high-fat diet when pact of hormones like leptin (a long-term peripheral hor-
rats have simultaneous access to two diets differing in their mone) was not as clear as the macronutrients preferences
relative amounts of fat. were different dependent on the age of rats, type of infusion
(acute or chronic), and their baseline macronutrients pref-
Similarly to AgRP, NPY-induced hyperphagia is dependent erences (323).
on opioid receptor activation, which also causes a shift in
food choices (128, 159). Increased consumption of carbo- The effect of insulin on sugar consumption has long been of
hydrates diet is linked to increased levels of NPY in the interest. In 1958, Jacobs et al. (147) found that insulin
hypothalamus. In addition, administration of NPY report- injections in rats resulted in a shift in consumption of sweet
edly increases the consumption of high-carbohydrate diets solutions from 10% concentration to 35% concentrations,
(285, 316). suggesting an increased preference for sweet solutions. In
our current understanding, this is not surprising as insulin-
MCH differs from NPY and AgRP in that its orexigenic induced hypoglycemia promotes the seeking for urgent and
effect does not depend on opioid reception activation. In- quick release source of energy to correct the blood sugar
terestingly, central MCH administration in rats resulted in concentrations.
1124 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
Table 1. Summary of the effect of appetite neurotransmitters on changes in food preferences
Factor Type of Study Method Food Preferences
POMC Animals (307) Examined Pomc-null, Pomc⫹/⫺, and Increases fat diet; no change in
wild-type mice protein or carbohydrates
Humans (45) Genome-wide scan and Food Frequency Increases saturated fat intake
Questionnaires
CART Animals (66) Two-bottle test in Carttm1Amgen knockout No change in sucrose preference
(Cart KO) and wild-type (WT) mice
AgRP Animals (128) Effect of central administration of AgRP Increases high-fat diet over low-fat
vs. saline into the third cerebral diet; no change in sucrose
ventricle in rats on high-fat, low-fat, preference
and sucrose preference
NPY Animals (316) Rats self-selected macronutrients or High-carbohydrate diets linked with
given a single-diet paradigm followed higher levels of NPY
by measurement of hypothalamic NPY
levels
Animals (285) Effect of NPY injected into the Increases carbohydrate
paraventricular nucleus in rats on consumption; no change in
carbohydrate, protein, and fat diet protein or fat consumption
MCH Animals (59) Effect of MCH injection into the third No change in food selection
cerebral ventricle in rats on high-fat
and low-fat diet
Orexins Animals (59) Effect of orexin-A injection into the third Increases high-fat diet
cerebral ventricle in rats on high-fat
and low-fat diet
Endocannabinoid Animals (98) Effect of intraperitoneal injection of CB1 Increases carbohydrate intake
receptor agonist, ACEA, on protein,
carbohydrate, and fat intake
Animals (186, Effect of CB1 receptor antagonist Reduced preference and
236, 274) (rimonabant) on food choice and motivation to seek palatable food
motivation to palatable food options choices
Humans Effect of CB1 receptor antagonist Reduced brain activation towards
(144) (rimonabant) on brain activation the sight and smell of chocolates
(rewarding food)
Reference numbers are given in parentheses.
Conversely to leptin and insulin, PYY is a short-term pe- (309). In their study, Peters et al. (227) found that exendin
ripheral hormone. Central administration of PYY1–36 in 9 –39 significantly enhanced food intake suppression occur-
satiated rats resulted in an increase in carbohydrate and fat ring after glucose, but not after corn oil or albumin preloads
intake as opposed to protein when given all three macronu- supporting the nutrient selection action. In the diet selection
trients (285). No current studies are available on the effect studies, exendin 9 –39 selectively decreased intake of a high-
of PYY3–36 on food choice. carbohydrate diet, suggesting that blocking GLP-1 activity
leads to a selective feeding response to the carbohydrate
The effect of GLP-1 on the quantity of food intake is well portion of the diet. On the other hand, exendin 4 selectively
evidenced in humans (105, 125) and experimental animals decreased the intake of a high-protein diet (227). Rats
(309). However, its effect on the composition of food intake treated with liraglutide (Victoza/Saxenda), a synthetic
has not been as clear. GLP-1 is a nutrient-specific hormone. GLP-1 receptor agonist used as a type 2 diabetes mellitus/
Its secretion has been reported to be particularly sensitive to obesity treatment, decrease their intake of foods high in
the ingestion of carbohydrates (241) and long-chain unsat- sugar and/or fat relative to laboratory chow (131, 237).
urated fatty acids (244), but slightly if at all sensitive to Only recently, the impact of GLP-1 on macronutrient selec-
proteins (92) and amino acids (64). To investigate if this can tion in humans became available. Blundell et al. (31) found
impact on macronutrient selection, Peters et al. (227) in- that semaglutide caused reduced liking and wanting based
jected rats with exendin 4 and exendin 9 –39. Exendin 4 is a on verbal reports, and reduced intake of high-fat and savory
GLP-1 receptor agonist and exendin 9 –39 GLP-1 is a recep- food in an ad libitum evening snack meal. Hyde et al. (146)
tor antagonist, which both have been used in animal studies however tested liraglutide in a highly controlled cafeteria
in place of GLP-1, due to its short half-life (227). Central diet paradigm to directly measure food choices. They found
administration of exendin 4 in rats has been shown to de- although the GLP-1 analog potently reduced food intake
crease food intake (81, 209, 244a, 309), whereas treatment both when rats were offered a palatable or less palatable
with exendin 9 –39, increases food intake in sated rats diet, it did not alter food preferences (146).
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1125
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
Table 2. Summary of the effect of appetite hormones on changes in food preferences
Factor Type of Study Method Food Selection
Leptin Animals (323) Intraperitoneal injection Leptin has different effects on macronutrient preferences,
dependent on age and the type (acute or chronic) of
injection
Insulin Animals (147) Insulin injections Increased glucose preference
CCK No studies — —
PYY Animals (285) PYY injected into the paraventricular nucleus Increases CHO intake, and small (significant) increase in
in rats fat consumption; no change in PRO consumption
PP No studies — —
GLP-1 Animals (227) Intraperitoneal injection of GLP-1 antagonist Exendin 9–39 selectively decreased intake of CHO; exendin
(exendin 9–39) and its agonist (exendin 4) 4 decreased intake of PRO
Animals (146) Once daily injections No alteration in food preferences
Humans (31) Once weekly subcutaneous injection Reduced intake of high-fat and nonsweet snacks
Ghrelin Animals (267) Central injection Increases fat intake over CHO intake
Animals (88) Peripheral administration Stimulates the intake of fat-rich palatable foods
Reference numbers are given in parentheses.
Ghrelin was also linked to changes in food choices. Shim- Once the taste is identified, signals are sent to the NTS in
bara et al. (267) demonstrated increased fat intake and the hindbrain to determine the appropriate responses.
reduced carbohydrate intake after central administration of Responses are classified into aversive or appetitive, de-
ghrelin. Peripheral ghrelin administration also stimulates pending on the effect the stimulus has on the hedonic
the intake of fat-rich palatable foods, whereas blocking the system. Physiological responses are in turn the body’s
release of ghrelin through genetic or pharmacological inhi- way of preparing the digestion and ingestion of that par-
bition results in a decrease in their intake (88). TABLE 2 ticular stimulus (282). Those three functional domains
summarizes the effect of peripheral hormones on changes in (FIGURE 4) are equally important for the function of taste.
food preferences. Therefore, the taste systems can be broken down into
three main functional domains: stimulus identification,
2. Taste function ingestive motivation, and digestive preparation (FIGURE
5) (282).
Taste directly influences eating behavior through its effect
on food preference and food intake. Taste is the sensation A) STIMULUS IDENTIFICATION. The stimulus identification dom-
produced when a substance enters the mouth and reacts ain or “sensory domain” encompasses the sensory function
with the taste receptors cells located on the taste buds. of the taste system to detect “sweet,” “salty,” “bitter,”
Reward
*Consummatory
Reward
*Appetitive
Sensory Reward Physiology
Detection or post-ingestive
Discrimination effects FIGURE 5. The taste domains as described by A. C. Spec-
tor (282).
Taste
1126 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
“sour,” and “umami” (e.g., monosodium glutamate taste) blood sugar that cause a “satiation effect” towards sweet
tastes. taste and/or neuropathy causing a reduced taste sensitivity
overall (255). A number of studies subsequently established
Taste is detected when the concentration of the tastant that patients with T2DM have higher thresholds for glucose
reaches a threshold level that activates taste receptors to and sucrose detection than patients with type 1 and controls
generate action potentials in gustatory nerve fibers that are (43, 116, 291, 291). In addition, hyperglycemia is associ-
potent enough to elicit a taste perception (124). Taste sen- ated with higher sweet taste thresholds when patients with
sitivity ranges from the lowest concentration of taste stimuli diabetes and pre-diabetes are compared (43, 319).
that can be detected (taste detection thresholds) to the in-
tensity perceived for that stimulus (above-threshold re- Depression and anxiety, common comorbidities of obesity
sponses) (33). (219, 262), also alter taste. Severely depressed patients have
reduced sensitivity to all tastes, most commonly sweet
Taste may contribute to the development of obesity; how- (290), which normalizes on recovery. They also report
ever, it is difficult to assess whether hypogeusia (reduced lower intensity responses to suprathreshold stimuli (8).
taste sensation) causes hyperphagia and weight gain or vice Based on the “monoamine theory of depression,” it is the
versa. Bartoshuk et al. (17) stated, “The obese live in differ- result of a deficiency in circulating monoamine concentra-
ent orosensory and orohedonic worlds than do the tions and hence reduced neurotransmission of norepineph-
non-obese.” rine, dopamine, and serotonin (5-HT), and/or reduced sen-
sitivity of their receptors (140). Taste cells express 5-HT, its
Many studies have shown associations between taste synthetic enzymes, and its receptors. Therefore, 5-HT is
thresholds and weight (202, 269, 272). Kawai et al. (151) involved in the taste signaling by altering ion channel func-
found that leptin, an adipokine, inhibited specific sweet tion. Measurement of taste function in healthy humans
taste responses in lean mice but not in obese diabetic (db/ showed that enhancing 5-HT increased sweet taste sensitiv-
db) mice, suggesting a role of this hormone in sweet taste ity by significantly reducing the sucrose taste threshold by
sensitivity. Kawai et al. (151) found that Ob-R, the leptin 27% (136).
receptor, is also found in the taste cells of circumvallate
papillae in mice in addition to where it has previously been 5-HT is implicated in the development of anxiety and stress
suggested to be present, i.e., the CNS (65), peripheral cells (117). Anxiety and stress, similarly to depression, often lead
such as T cells (175), vascular endothelial cells (317), mus- to increased intake of high sugary food (47, 335) which
cle cells (155), and pancreatic cells (142), indicating that could be a result of the reduced sweet taste sensitivity
taste cells are a site of leptin action (151). Peripheral leptin caused by the reduction in 5-HT (136).
resistance is well described in obese mice and humans as a
mechanism increasing food intake, and whether this phe- Taste stimulation was attributed to be one of the contribu-
nomenon extends into the sensory taste domain is unclear tors to the change in appetite and eating behavior, particu-
(109). Obese rodents and humans have increased levels of larly to the changes in food preferences. De Wys and Wal-
circulating leptin compared with normal weight subjects ters (77) reported a connection between taste changes and
(179). During weight gain, basal plasma leptin levels should food aversions. They found that increased taste acuity for
gradually rise, concomitantly sweet taste sensitivity reduce. urea (bitter) in cancer patients correlated with meat aver-
However, chronic adaptation to high concentrations of lep- sions. Aversions to sweet foods have been associated with
tin may elicit leptin resistance in the taste cells as suggested increases in taste acuity for sucrose (sweet) (39). Based on
by Yoshida et al. (333). This means that any further in- these results, Scruggs et al. (264) were the first to suggest
creases in leptin concentration would not elicit further sup- that the changes in food preferences after RYGB may be
pression (151). attributed to the permutation in taste acuity. To test their
hypothesis, taste detection and recognition thresholds for
Weight loss reduces leptin levels and increases sweet taste the four basic tastes (salt, sweet, sour, and bitter) were
sensitivity, i.e., decreased thresholds, both after invasive, assessed using a modification of the Henkin forced choice
i.e., surgical-induced weight loss (37, 40, 264), and nonin- three-stimulus technique before and after RYGB in women
vasive, i.e., diet-induced weight loss (310), procedures. (137). This technique involves placing drops of water or
Taste sensitivity correlates with reductions in leptin levels tastant on the tongue of the volunteer. The lowest concen-
(310). tration at which the volunteer is able to detect the difference
between the tastant and water represents the detection
Obesity is associated with many related comorbidities in- threshold (137). In this study, Scruggs et al. (264) found
cluding type 2 diabetes mellitus (T2DM). Fabbi (100) was that following gastric bypass surgery, a significant improve-
the first researcher who suggested that patients with diabe- ment in taste acuity for bitter and sour was observed along
tes may have impaired taste function. Later they suggested with a trend toward a reduction in salt and sweet detection
that this abnormality might be due to the elevated levels of thresholds. Methodological limitations of the study include
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1127
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
the use of a small sample number (n ⫽ 6), use of tiny tastant “reward domain” comes into play to promote or discour-
drops that causes limited receptor stimulation, and the lack age the ingestion of food (FIGURE 5) (282). The ingestive
of control for the effects of repeated testing. Additionally, motivation domain differs from the stimulus identification
the concentrations of the solutions used were very high, domain in that it represents the hedonic aspects of gustation
especially for sucrose (197). (282). For example, we can distinguish between the differ-
ent taste qualities of food and drinks regardless of whether
Burge et al. (40) used a staircase method of stimulus presen- they are pleasant or aversive by the stimulus identification
tation and found that sucrose recognition thresholds also domain; however, we will only ingest more when it is de-
decreased after RYGB. The group also noted that patients termined to “tastes pleasant” by the ingestive motivation
reported that food tasted sweeter, and they modified food domain.
selection accordingly. Burge et al. (40) also found that pa-
tients who reported an aversion to meat were associated Spector (282) described the taste-related ingestive motiva-
with increased nausea and vomiting. tion as having two subdomains or components: appetitive
behavior and consummatory behavior. Appetitive behavior
Using direct measures of behavior, we investigated the ef- describes the efforts that the subject will undertake to be put
fects of RYGB on the sweet taste sensory domain using a in contact with the food, e.g., searching, foraging, ap-
method of constant stimuli (37) and showed that sweet taste proaching a drinking spout, whereas consummatory behav-
acuity improves after RYGB (37). ior represents the behaviors elicited by the final act when
contact is made with the stimulus (282). Some authors have
Despite all the previous studies showing improvement in equated appetitive behavior to “wanting” and consumma-
taste acuity after RYGB, the change in taste detection tory behavior to “liking” of the stimulus, but it may be
thresholds for sucrose remains controversial. The latest more helpful to consider the actual behaviors as these can
study by Pepino et al. (224) found no change in detection be directly measured experimentally rather than relying on
thresholds for any of the taste qualities [sucrose, glucose, verbal report.
NaCl, and monosodium glutamate (prototypical savory
stimuli)] after RYGB and BAND. The discrepancy between In research, the two ingestive behavior components can be
the earlier studies may be due to differences in the method- studied in combination but also in isolation, depending on
ologies employed to measure taste thresholds, variation in the outcome required. The brief access test is an experi-
the diet composition of subjects at the time of testing, time mental test used for measuring both components of the
from surgery, and sex differences. ingestive motivation domain (324). In this test, a very
small sample of the tastant is presented for a brief dura-
The current literature lacks any studies on taste detection in tion (e.g., 10 s) and the animal’s licking responses are
VSG. Our research group carried out the first taste detection measured using a lick monitoring system (gustometer)
experiment on VSG adolescents in Saudi Arabia by follow- (324). Therefore, it allows measurement of the amount of
ing the same protocol we have previously used on RYGB effort the animal is prepared to undertake to approach
patients (37). We found that VSG did not have an effect on the spout (which may broadly equate to “wanting” the
the detection threshold for sucrose in adolescent patients taste stimulus), and also measurement of the repetitivity
(G. Abdeen et al., unpublished work). Our results suggest per unit time of tongue protrusions over the duration of
that VSG might not fundamentally shift the sensory domain the test (equating to “liking” the stimulus) (3). The ben-
of taste, but food preference changes may instead be related efit of the brief access test is that it minimizes any
to other factors such as conditioned avoidance. postingestive effects of the taste stimuli as only small
amounts are ingested (278, 283).
Several gut peptides, including GLP-1 (102), NPY (338),
glucagon (94), and ghrelin (270) are secreted in response to When the appetitive and the consummatory behavior com-
various taste stimuli and may contribute to taste quality ponents of the ingestive motivation domain are studied in
coding (82, 113). A recent study by Takai et al. (298) found isolation, different experimental tests and tools are re-
that GLP-1 is released from the sweet-sensitive taste cells quired. The appetitive behavior can be assessed using the
(T1R3) immediately after stimulation with sweet com- progressive ratio task (PRT) which was originally designed
pounds, suggesting that GLP-1 might stimulate sweet-sen- by Hodos in 1961 for the use in animal studies (141). This
sitive gustatory nerve fibers. RYGB and VSG patients have task was adopted for the use in human studies for the same
increased postprandial GLP-1 levels (165), which may con- purpose (196). During this task, the subject is required to
tribute to the increased sweet taste sensitivity reported pre- perform a certain number of responses to obtain a rein-
viously (37, 40, 264). forcer (i.e., a reward). After consumption of each reward,
the response demand progressively increases until it is so
B) INGESTIVE MOTIVATION. When a taste is detected in the stimulus great that the subject stops responding. This is referred to as
identification domain, the ingestive motivation domain or the breakpoint and represents the reward value of the rein-
1128 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
forcer. The PRT is thus an assessment of appetitive respon- In 2012, Mathes et al. (185) also used a brief access test with
siveness (196). gustometer. Surprisingly, they showed almost a doubling in
the appetitive behavior of rats after RYGB for sweet stimuli
Consummatory behavior can be assessed using a taste reac- (185, 339). Although not quite the same outcome, Mathes
tivity test (3). This test has been used in animal studies, et al. (184) repeated the experiment using (PR) lick operant
where an intraoral cannula infuses a taste stimulus directly to study the effect of RYGB in rats on the reinforcement
into the oral cavity and the facial reactions are videotaped value of palatable fluid stimuli. After surgery, RYGB oper-
and analyzed by the investigator (122). Common ingestive ated rats did not show lower breakpoints than SHAM rats
(i.e., positive) animal reactions include tongue protrusions for reinforcers consisting of Ensure, sucrose, or 5% Intr-
and paw licking. While the common aversive (i.e., negative) alipid, even though they had blunted preferences for these
reactions include gapes and chin rubbing (21). Our research caloric fluids versus water in two-bottle preference tests
group has adopted this test for the use in human obesity (184). Those results are also supported by the work of Wil-
studies (G. Abdeen et al., unpublished work). In this human son-Pérez et al. (325) on VSG rats for fat or a carbohydrate
study, a 50-ml chocolate milkshake flowed directly into the food reinforcer. Collectively, those studies started to shift
subjects’ mouths using gravity to deliver a rate of 25 ml/ our thinking that bariatric surgery may not cause changes in
min. Subjects’ facial expressions were recorded on a camera food preferences due to altered palatability of foods but
and were later analyzed using a Facial Expression Food rather due to a learned adjustment to altered postingestive
Preference Rating Scale (G. Abdeen et al., unpublished feedback.
work). Common ingestive human facial reactions to pleas-
ant stimuli include tongue protrusion, mouth movements, The discrepancies with human studies are intriguing and
and ingestion of the stimuli. While aversive facial reactions raise the question of whether, despite best efforts, patients
include gaping, head shaking, wrinkling of the nose, retrac- may still behave in a specific way to “please” the investiga-
tor, a problem that is not seen in rats. An alternative expla-
tion of the head away from the source, and fluid expulsion
nation may be that humans were studied in an acute nega-
(89, 121, 289).
tive energy balance phase while rats were studied when they
were maintaining weight loss and were in a stable energy
C) APPETITIVE BEHAVIOR. To objectively assess the role of this
balance phase.
taste subdomain on changes in the food preferences ob-
served after bariatric surgery, Miras et al. (196) used the
D) CONSUMMATORY BEHAVIOR. This ingestive behavior is actioned
PRT in patients before and after RYGB surgery. He
by the reward value of the stimuli tasted. When food is in
found that the surgery resulted in the selective reduction
the oral cavity, the taste signal is sent to the orbitofrontal
of the reward value of a sweet and fat tastant. Our re-
cortex in the CNS to encode the reward value of a food
search group has also found the same results after VSG
stimulus. The orbitofrontal cortex further communicates
surgery in adolescents (G. Abdeen et al., unpublished
with other limbic structures such as the ventral tegmental
work). area, nucleus accumbens, amygdala, hippocampus, and
ventral striatum with dopamine acting as the primary neu-
Importantly, employing the same task in animal models of rotransmitter. This hedonic activation has led many re-
RYGB and VSG expands our understanding of the mecha- searchers to focus on neuroimaging in the form of fMRI and
nisms that underlie the change in behavior (196). In animal positron emission tomography scans to investigate the
studies, there have been mixed findings as some have shown changes in the hedonic value of food after RYGB.
increases in appetitive responsiveness to sweet-tasting or
fatty stimuli but other studies have not. Tichansky et al. Indeed, a number of studies have found that RYGB is asso-
(304) attempted to assess taste sensitivity in rats using a ciated with decreased hedonic value for food after RYGB
brief access test with gustometer consisting of different su- and particularly sweet or highly palatable foods (215, 257).
crose concentrations. While this experiment may not be These were well-structured studies and showed promising
appropriately designed for the assessment of “taste sensitiv- results but did not particularly assess consummatory behav-
ity,” the result can be interpreted to reflect the “appetitive ior, i.e., the liking and disliking of food; they were also
behavior” to different sweet concentrations. In this study, based on visual and auditory cues, not taste, and therefore
the overall mean licks for the five different sucrose concen- are not actual ingestive behavioral in response to a food. In
trations did not differ significantly. Rats showed a signifi- a step forward, Ochner et al. (216) used VAS and fMRI
cant reduction in the mean licks over a 10-s period for the scans to correlate brain activation with the rating of the
highest three concentrations. Nevertheless, they still had a desire to eat “wanting” and “liking,” though it was also
considerably high mean licks compared with water or with based on visual cues and not real food stimuli. The group
the low sucrose concentrations, suggesting that the rats still found that “liking” of food was not changed despite the
worked harder for the sweeter stimuli than they did to com- reduction in hedonic activation. Scholtz et al. (256) com-
pletely avoid them (304). pared RYGB to BAND patients and found that RYGB
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1129
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
caused a greater reduction in the activation of brain reward Berthoud et al. (28) provided three concentrations of su-
areas to high-energy food pictures. In addition, this work crose solution to lean, sham-operated obese, and RYGB
associated the hedonic brain activation with the rating of rats. Lean and sham-operated obese rats showed a right
high-sugar/high-fat food ingestion and found that lower shift of the concentration-response curve, and RYGB rats
hedonic brain activation was associated with the rating of had an essentially flat curve, with more responding to the
ice cream ingestion as “less pleasant to eat” in the RYGB lowest, and less responding to the highest, sucrose concen-
group (256). The findings of this study were explicable by tration (though not significantly different) (28).
differences in the anorexigenic plasma gut hormones
(GLP-1 and PYY), plasma bile acids, and symptoms of Taste plays an important role in pre-
E) DIGESTIVE PREPARATION.
dumping syndrome (256). paring the body for the digestion of a meal. Once the food is
present in the mouth, a number of physiological reflexes can
Faulconbridge et al. (101) compared the neural response to take place as part of cephalic phase responses (FIGURE 5).
pictures of high- and low-calorie foods (HCF and LCF), Salivation is the most obvious cephalic response (190) and
before and 6 mo after RYGB and VSG and in nonsurgical can be triggered by the mere thought of food but increases
weight-stable control participants. Liking ratings for HCF mostly when food is present in the oral cavity (240). Powley
decreased significantly in the RYGB and VSG groups but (234) suggested that cephalic phase responses are increased
remained stable in the control group, indicating reduction with the appetite for food; however, subsequent studies
in liking of highly palatable foods after obesity surgery. found that salivation rate is not actually dependent on the
However, blood oxygen level-dependent (BOLD) response level of hunger (55, 210). The rate of salivation does differ
in the ventral tegmental area (VTA) to HCF (vs. LCF) de- based on the taste of stimuli, with the highest saliva stimu-
clined significantly more at 6 mo in RYGB compared with lation produced by a sour taste, followed by salt, sweet, and
control participants but not in VSG participants (101). bitter (72, 154). Salivation rates are increased with higher
There was no significant changes in any of the other regions concentration of the stimuli (110, 320). A number of studies
relevant to reward processing (101). have suggested that body weight can affect salivation, with
people with obesity having a higher salivation rate; this may
Another method used to explore consummatory taste be- be explained by people with obesity having higher re-
havior in RYGB patient is the Sweet Taste Palatability Test. sponses to food cues and higher food reinforcing value (95,
In this test subjects rate different sucrose concentrations 126, 213). People with obesity also have a slower habitua-
using VAS or global Label Magnitude Scales (gLMS). In tion rate (reduced salivation to the same ingested food)
patients after RYGB, no changes in the sucrose concentra- which can partially contribute to increased food intake (95,
tion that is considered as “just about right” were detected 303).
when comparing patients before and after surgery (37). On
the contrary, Pepino et al. (224) carried out a modified Additional evidence supports the existence of other taste-
version of this test on RYGB and BAND patients and found related physiological reflexes such as delayed increase in
that RYGB surgery, but not BAND, affected the consum- blood triacylglycerol levels (189) and secretion of gastric
matory component of sweet taste perception, characterized acid (148) as well as amylase, gastrin, CCK, glucagon, and
by a rapid shift in sweetness palatability from pleasant to pancreatic polypeptide (327). Another taste-related ce-
unpleasant when repetitively tasting sucrose. phalic response is preabsorptive insulin release, which has
been studied extensively in animals (24 –26, 271) and hu-
The taste reactivity test can also be used to assess facial mans (176, 243, 301, 302). Measuring preabsorptive insu-
expressions for liking and disliking of sweet/fatty stimulus. lin release can be challenging and require a large sample size
This test has not been used in RYGB patients as yet, but we and careful protocol consideration as suggested by Teff et
completed a pilot study to investigate facial expressions in al. (302).
obese adolescent VSG patients in response to high-fat/high-
sugar food stimuli (unpublished work). We used the facial Food odors stimulate cephalic phase responses (332). Using
expression method to assess changes in the consummatory the threshold-discrimination-identification (TDI) test, Juro-
behavior relating to a single, specific food item after VSG wich et al. (148a) found a significant increase in olfactory
surgery. VSG resulted in increased negative (dislike) facial function 24 wk after sleeve gastrectomy (SG), but not after
expressions and decreased positive (liking) facial expres- RYGB. Richardson et al. (239) also did not show improve-
sions for a chocolate milkshake stimulus. In addition, facial ment in olfactory function following RYGB, using cross-
expressions remained unchanged across a similar test-retest cultural smell identification test (CC-SIT). More studies on
interval in nonsurgical control subjects. On the other hand, changes in cephalic phase responses after bariatric surgery
animal studies by Shin et al. (268) found more positive are needed to expand our understanding of this domain.
orofacial responses to low concentrations of sucrose but
fewer to high concentrations after RYGB, indicating re- FIGURE 6 presents the integration of the three functional
duced consummatory behavior for higher sweet stimuli. domains of taste in eating behavior.
1130 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
Psychological traits, cognition,
and learned behavior
Social and
environmental triggers
n FIGURE 6. The integration of the three functional do-
io
ct
mains of taste (stimulus identification, ingestive motiva-
te
de
Pe
Pr
n
tion, and digestive preparation) in eating behavior.
io
e-
rip
e
at
ab
st
Black arrows represent triggers of eating behavior,
he
liv
Ta
so
Sa
ra
un
green arrows represent response signals from the
rp
ls
ge
tiv
ig
Reward value for taste
brain to initiate or terminate an eating episode, and
ra
na
in
nd
ls
orange arrows represent cephalic phase responses.
su
sa
lin
The three functional domains discussed above inte-
tie
re
ty
le
grate together via multiple signals sent to the brain to
si
as
gn
e
determine the reward value for taste of the ingested
al
s
food. The ingestive motivation domain can influence in-
gestive behavior by any or all of the following: 1) the
metabolic (e.g., hunger, thirst), 2) the oro-sensory
(e.g., taste, texture), and 3) the postabsorptive (e.g.,
Ap
glycemic excursions, satiation) dimensions. Any change
pe
tit
to one or all of the stimulus identification, ingestive
iv
e
motivation, and digestive preparation domains can also
be
ha
alter eating behavior and thus obesity.
vi
C
or
on
su
m
m
at
or
y
be
ha
vi
or
C. Other Contributing Mechanisms The acquisition of conditioned taste aversion occurs when
the subject associates the novel taste of a new sickness-
Memory impacts on food intake and preferences. As hu- inducing food (unconditioned stimulus) with nausea gener-
mans and animals evolved, they had to learn which food in ated from its consumption (unconditioned reaction). “Un-
the wild was safe or not safe to eat (322). Taste provides conditioned” is a term used for first time exposure to the
critical initial signals about the safety of the food. Sweet stimulus and reaction. However, future exposures become
taste often indicates that the food is energy dense and safe, “conditioned” as the subject has learned what reaction
whereas bitter taste often indicates toxicity and potentially could be expected (322). Avoiding the conditioned stimulus
hazards (76). However, taste is only the initial indication; altogether in the future is a sign of an established condi-
once the food is consumed further consequences can be tioned aversion reaction (322).
generated. For example, nutritious food will suppress hun-
ger and provide energy, and therefore, it will be labeled as In contrast, conditioned taste avoidance refers to the con-
“familiar and safe.” If the food results in significant gastro- scious avoidance of food that is still palatable but has
intestinal malaise, it will be labeled “familiar and not safe,” caused adverse reactions when larger quantities are con-
which is referred to as conditioned taste aversion (260). sumed, for example, lactose intolerance or nut allergy.
Conditioned behavior is of a particular interest in obesity Studies with rats indicate that the two terms “conditioned
and obesity surgery studies as patients often report changes taste avoidance” and “conditioned taste aversion” should
in their likes and dislikes of certain types of food. In this not be used interchangeably as they are different processes
section, we review the difference between aversion and (221). Aversion to food is accompanied by a strong dislike
avoidance of certain types of food and their possible mech- or disinclination to the stimuli with almost complete resis-
anisms. tance to any ingestion, whereas avoidance of food happens
as the subject starts ingestion but then stops the consump-
1. Conditioned aversion versus conditioned tion of the food subsequently despite its palatability.
avoidance
Facial and somatic reactions of rats were used to determine
Conditioned taste aversion is a form of classical condition- taste avoidance and aversion in a taste reactivity test (TR
ing, which is the simplest form of associative learning (322). test), which is a classic technique to investigate consumma-
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1131
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
tory behavior (122). When rats are exposed to a flavored (97, 129, 166, 184, 325). However, if we plot a trend in
solution like sucrose, which does not induce negative con- those studies, we can see that humans and rats did not
sequences, they develop a “liking” of the solution. How- completely avoid the food provided to them which indicates
ever, if the sucrose solution is then paired with a drug that that they may still “like” sweet and fatty food but they
induces nausea, they will feel endangered and develop a “avoid” eating the same quantity as they did before the
taste aversion to the same solution. This is expressed by operation, possibly in an attempt to avoid negative visceral
conditioned disgust reactions such as mouth gaping (221). signals associated with larger quantities. Therefore, they are
On the other hand, if taste avoidance occurs, then the ani- more likely to have developed conditioned taste avoidance.
mal may still like the food and choose it over others but tries A study comparing intake of high-fat diets after RYGB in
to avoid large quantities of it. In further tests, Suncus mu- rats that were either exposed or not exposed to the same
rinus (house musk shrew) were tested with a sucrose solu- high-fat diet before surgery suggest that if the high-fat diet
tion paired with amphetamine, cocaine, or morphine. The was novel, then the rats completely avoided subsequent
shrew showed positive, euphoric reactions to solutions. intake when the high-fat diet was presented after surgery.
However, they reacted to the change in their physiological However, if the rats were familiar with the high-fat diet
state as a sign of danger and thus avoided approaching these before surgery, they again consumed the diet after surgery,
solutions. The shrew yet preferred the solution that it had but quickly reduced the total consumption to much lower
taste avoidance towards rather than the other solution it levels. The rats however never stopped consuming the high-
had a learned taste aversion towards (221, 222, 279). fat diet, suggesting that the palatability did not change but
rather they became conditioned to avoid larger quantities
During the early phase after bariatric surgery, patients suf- (265).
fer from a number of symptoms associated with eating that
can be grouped under an umbrella term of “postprandial
discomfort.” Postprandial discomfort may have a signifi- VII. CONCLUSION AND PERSPECTIVES
cant impact on conditioned eating behavior including food
choices, portion size, frequency of food consumption, meal Weight loss following bariatric surgery is a result of reduced
times, and so on. calorie intake. Altered satiety, food reward, and food pref-
erences may all contribute to the reduction in calorie intake.
2. Postprandial discomfort None of those eating behavior entities works in isolation.
Instead, they interact in the same individual and have addi-
Postprandial discomfort refers to a number of symptoms tive or synergistic effects as a consequence of conditioned
that can occur individually or collectively after an eating and/or unconditioned factors. However, bariatric surgery
episode. Those symptoms include abdominal pain, diar- procedures still have risks, and not all obese patients are
rhea, borborygmi, nausea, bloating, fatigue, a desire to lie eligible or indeed want surgery. Therefore, understanding
down after meals, facial flushing, palpitations, perspiration the mechanisms of successful therapies such as bariatric
tachycardia, hypotension, syncope, and hypoglycemia surgery may help improve other treatment options for obe-
(297). Most research studies focus on Dumping Syndrome sity. In addition, a number of patients after bariatric surgery
(DS) as the main cause of postprandial discomfort. The have suboptimal weight loss. Understanding how these pa-
rapid absorption of simple carbohydrates causes an ele- tients differ from those that lose more weight especially as
vated production of insulin, which in turn lead to a signifi- regards eating behavior may help make the surgical treat-
cant reduction in blood sugar glucose and hypoglycemia. ments even more successful.
Changing the diet to a high-protein, low gastrointestinal
diet can prevent the symptoms of DS in the majority of The future is likely to see more combined gut hormone
patients. However, we cannot disregard certain eating hab- therapies (299), minimally invasive devices such as the En-
its, for example, eating large amount of food or fast eating doBarrier (170), or even a combined multi-model “medical
pace, in resulting with increased postprandial production of bypass” approach (195), on appetite and food preferences.
satiety peripheral signals and therefore negative visceral sig- These treatments can mimic various components of the
nals being sent to the brain. RYGB and could collectively help us guide perspective stud-
ies and treatments in the right direction. The challenge will
Postprandial discomfort often occurs after the consumption remain in finding out whether these minimally invasive
of high carbohydrates and fatty meals (91). It was originally treatments are ultimately capable of shifting or “resetting”
thought that because the brain associates those food groups the body’s fat “set point” similarly to RYGB.
with sickness, a conditioned taste aversion to “sweet” and
“fatty” food occurs. Sclafani and Koopmans (261) were the ACKNOWLEDGMENTS
first researchers to report that a jejunoileal bypass surgery in
rats produces a strong and persistent conditioned taste aver- We acknowledge the work done by Ghalia Abdeen on VSG
sion to novel-flavored solutions. Extensive research in this adolescents in Saudi Arabia and referenced in the manu-
area over the last few decades supported that hypothesis script as unpublished work.
1132 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
Address for reprint requests and other correspondence: C. 15. Bala V, Rajagopal S, Kumar DP, Nalli AD, Mahavadi S, Sanyal AJ, Grider JR, Murthy KS.
Release of GLP-1 and PYY in response to the activation of G protein-coupled bile acid
le Roux, Diabetes Complications Research Centre, UCD receptor TGR5 is mediated by Epac/PLC- pathway and modulated by endogenous
Conway Institute, School of Medicine and Medical Science, H2S. Front Physiol 5: 420, 2014. doi:10.3389/fphys.2014.00420.
University College Dublin, Dublin 4, Ireland (e-mail: carel.
16. Barkholt P, Pedersen PJ, Hay-Schmidt A, Jelsing J, Hansen HH, Vrang N. Alterations in
leroux@ucd.ie). hypothalamic gene expression following Roux-en-Y gastric bypass. Mol Metab 5: 296 –
304, 2016. doi:10.1016/j.molmet.2016.01.006.
GRANTS 17. Bartoshuk LM, Duffy VB, Hayes JE, Moskowitz HR, Snyder DJ. Psychophysics of
sweet and fat perception in obesity: problems, solutions and new perspectives. Philos
This work was supported by Science Foundation Ireland Trans R Soc Lond B Biol Sci 361: 1137–1148, 2006. doi:10.1098/rstb.2006.1853.
Grant 12/YI/B2480 and Health Research Board Grant 18. Batterham RL, Cowley MA, Small CJ, Herzog H, Cohen MA, Dakin CL, Wren AM,
USIRL-2016-2. Brynes AE, Low MJ, Ghatei MA, Cone RD, Bloom SR. Gut hormone PYY(3-36)
physiologically inhibits food intake. Nature 418: 650 – 654, 2002. doi:10.1038/
nature00887.
DISCLOSURES 19. Bavaresco M, Paganini S, Lima TP, Salgado W Jr, Ceneviva R, Dos Santos JE, Nonino-
Borges CB. Nutritional course of patients submitted to bariatric surgery. Obes Surg 20:
716 –721, 2010. doi:10.1007/s11695-008-9721-6.
No conflicts of interest, financial or otherwise, are declared
by the authors. 20. Belachew M, Legrand M, Vincent V, Lismonde M, Le Docte N, Deschamps V. Lapa-
roscopic adjustable gastric banding. World J Surg 22: 955–963, 1998. doi:10.1007/
s002689900499.
REFERENCES 21. Berridge KC. Measuring hedonic impact in animals and infants: microstructure of
affective taste reactivity patterns. Neurosci Biobehav Rev 24: 173–198, 2000. doi:10.
1016/S0149-7634(99)00072-X.
1. Abbatini F, Capoccia D, Casella G, Soricelli E, Leonetti F, Basso N. Long-term remis-
sion of type 2 diabetes in morbidly obese patients after sleeve gastrectomy. Surg Obes 22. Berthoud H-R, Morrison C. The brain, appetite, and obesity. Annu Rev Psychol 59:
Relat Dis 9: 498 –502, 2013. doi:10.1016/j.soard.2012.09.003. 55–92, 2008. doi:10.1146/annurev.psych.59.103006.093551.
2. Abdeen G, le Roux CW. Mechanism Underlying the Weight Loss and Complications of 23. Berthoud H-R, Neuhuber WL. Functional and chemical anatomy of the afferent vagal
Roux-en-Y Gastric Bypass. Review. Obes Surg 26: 410 – 421, 2016. doi:10.1007/ system. Auton Neurosci 85: 1–17, 2000. doi:10.1016/S1566-0702(00)00215-0.
s11695-015-1945-7.
24. Berthoud H, Bereiter D, Trimble E, Siegel E, Jeanrenaud B. Cephalic phase, reflex
3. Alan S. Psychophysical Evaluation of Taste Function in Nonhuman Mammals. In: insulin secretion Neuroanatomical and physiological characterization. Diabetologia 20,
Handbook of Olfaction and Gustation. New York: Informa Healthcare, 2003.
S1: 393– 401, 1981. doi:10.1007/BF00254508.
4. Alden JF. Gastric and jejunoileal bypass. A comparison in the treatment of mor-
25. Berthoud HR, Jeanrenaud B. Sham feeding-induced cephalic phase insulin release in
bid obesity. Arch Surg 112: 799 – 806, 1977. doi:10.1001/archsurg.1977.
the rat. Am J Physiol Endocrinol Metab 242: E280 –E285, 1982.
01370070011001.
26. Berthoud HR, Trimble ER, Siegel EG, Bereiter DA, Jeanrenaud B. Cephalic-phase
5. Almogy G, Crookes PF, Anthone GJ. Longitudinal gastrectomy as a treatment for the
insulin secretion in normal and pancreatic islet-transplanted rats. Am J Physiol Endocri-
high-risk super-obese patient. Obes Surg 14: 492– 497, 2004. doi:10.1381/
nol Metab 238: E336 –E340, 1980.
096089204323013479.
27. Berthoud HR. Homeostatic and non-homeostatic pathways involved in the control of
6. AMA. Recognition of Obesity as a Disease. https://policysearch.ama-assn.org/
food intake and energy balance. Obesity (Silver Spring) 14, Suppl 5: 197S–200S, 2006.
policyfinder/detail/H-440.842?uri⫽%2FAMADoc%2FHOD.xml-0-3858.xml.
doi:10.1038/oby.2006.308.
7. Ammon BS, Bellanger DE, Geiselman PJ, Primeaux SD, Yu Y, Greenway FL. Short-
28. Berthoud HR, Zheng H, Shin AC. Food reward in the obese and after weight loss
term pilot study of the effect of sleeve gastrectomy on food preference. Obes Surg 25:
1094 –1097, 2015. doi:10.1007/s11695-015-1602-1. induced by calorie restriction and bariatric surgery. Ann N Y Acad Sci 1264: 36 – 48,
2012. doi:10.1111/j.1749-6632.2012.06573.x.
8. Amsterdam JD, Settle RG, Doty RL, Abelman E, Winokur A. Taste and smell percep-
tion in depression. Biol Psychiatry 22: 1481–1485, 1987. doi:10.1016/0006- 29. Björklund P, Lönroth H, Fändriks L. Manometry of the upper gut following Roux-en-Y
3223(87)90108-9. gastric bypass indicates that the gastric pouch and Roux limb act as a common cavity.
Obes Surg 25: 1833–1841, 2015. doi:10.1007/s11695-015-1639-1.
9. Andersson U, Filipsson K, Abbott CR, Woods A, Smith K, Bloom SR, Carling D, Small
CJ. AMP-activated protein kinase plays a role in the control of food intake. J Biol Chem 30. Blundell J. Pharmacological approaches to appetite suppression. Trends Pharmacol Sci
279: 12005–12008, 2004. doi:10.1074/jbc.C300557200. 12: 147–157, 1991. doi:10.1016/0165-6147(91)90532-W.
10. Angrisani L, Santonicola A, Iovino P, Formisano G, Buchwald H, Scopinaro N. Bariatric 31. Blundell J, Finlayson G, Axelsen M, Flint A, Gibbons C, Kvist T, Hjerpsted JB. Effects of
surgery worldwide 2013. Obes Surg 25: 1822–1832, 2015. doi:10.1007/s11695-015- once-weekly semaglutide on appetite, energy intake, control of eating, food prefer-
1657-z. ence and body weight in subjects with obesity. Diabetes Obes Metab 19: 1242–1251,
2017. doi:10.1111/dom.12932.
11. Anini Y, Brubaker PL. Role of leptin in the regulation of glucagon-like peptide-1
secretion. Diabetes 52: 252–259, 2003. doi:10.2337/diabetes.52.2.252. 32. Bray GA, Gallagher TF Jr. Suppression of appetite by bile acids. Lancet 291: 1066 –
1067, 1968. doi:10.1016/S0140-6736(68)91415-3.
12. Anton SD, Han H, York E, Martin CK, Ravussin E, Williamson DA. Effect of calorie
restriction on subjective ratings of appetite. J Hum Nutr Diet 22: 141–147, 2009. 33. Breslin PA, Spector AC. Mammalian taste perception. Curr Biol 18: R148 –R155, 2008.
doi:10.1111/j.1365-277X.2008.00943.x. doi:10.1016/j.cub.2007.12.017.
13. Bäckhed F, Ding H, Wang T, Hooper LV, Koh GY, Nagy A, Semenkovich CF, Gordon 34. Brolin RE, Robertson LB, Kenler HA, Cody RP. Weight loss and dietary intake after
JI. The gut microbiota as an environmental factor that regulates fat storage. Proc Natl vertical banded gastroplasty and Roux-en-Y gastric bypass. Ann Surg 220: 782–790,
Acad Sci USA 101: 15718 –15723, 2004. doi:10.1073/pnas.0407076101. 1994. doi:10.1097/00000658-199412000-00012.
14. Bal BS, Finelli FC, Shope TR, Koch TR. Nutritional deficiencies after bariatric surgery. 35. Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2011. Obes Surg 23:
Nat Rev Endocrinol 8: 544 –556, 2012. doi:10.1038/nrendo.2012.48. 427– 436, 2013. doi:10.1007/s11695-012-0864-0.
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1133
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
36. Bueter M, Löwenstein C, Olbers T, Wang M, Cluny NL, Bloom SR, Sharkey KA, Lutz 55. Christensen CM, Navazesh M. Anticipatory salivary flow to the sight of different
TA, le Roux CW. Gastric bypass increases energy expenditure in rats. Gastroenterol- foods. Appetite 5: 307–315, 1984. doi:10.1016/S0195-6663(84)80003-3.
ogy 138: 1845–1853, 2010. doi:10.1053/j.gastro.2009.11.012.
56. Christensen R, Kristensen PK, Bartels EM, Bliddal H, Astrup A. Efficacy and safety of
37. Bueter M, Miras AD, Chichger H, Fenske W, Ghatei MA, Bloom SR, Unwin RJ, Lutz the weight-loss drug rimonabant: a meta-analysis of randomised trials. Lancet 370:
TA, Spector AC, le Roux CW. Alterations of sucrose preference after Roux-en-Y 1706 –1713, 2007. doi:10.1016/S0140-6736(07)61721-8.
gastric bypass. Physiol Behav 104: 709 –721, 2011. doi:10.1016/j.physbeh.2011.07.
025. 57. Cicione C, Degirolamo C, Moschetta A. Emerging role of fibroblast growth factors
15/19 and 21 as metabolic integrators in the liver. Hepatology 56: 2404 –2411, 2012.
38. Bueter M, Miras AD, Chichger H, Fenske W, Ghatei MA, Bloom SR, Unwin RJ, Lutz doi:10.1002/hep.25929.
TA, Spector AC, le Roux CW. Alterations of sucrose preference after Roux-en-Y
gastric bypass. Physiol Behav 104: 709 –721, 2011. doi:10.1016/j.physbeh.2011.07. 58. Clarke G, Stilling RM, Kennedy PJ, Stanton C, Cryan JF, Dinan TG. Minireview: gut
025. microbiota: the neglected endocrine organ. Mol Endocrinol 28: 1221–1238, 2014.
doi:10.1210/me.2014-1108.
39. Burge JC, Park HS, Whitlock CP, Schemmel RA. Taste acuity in patients undergoing
long-term hemodialysis. Kidney Int 15: 49 –53, 1979. doi:10.1038/ki.1979.7. 59. Clegg DJ, Air EL, Woods SC, Seeley RJ. Eating elicited by orexin-a, but not melanin-
concentrating hormone, is opioid mediated. Endocrinology 143: 2995–3000, 2002.
40. Burge JC, Schaumburg JZ, Choban PS, DiSilvestro RA, Flancbaum L. Changes in doi:10.1210/endo.143.8.8977.
patients’ taste acuity after Roux-en-Y gastric bypass for clinically severe obesity. J Am
Diet Assoc 95: 666 – 670, 1995. doi:10.1016/S0002-8223(95)00182-4. 60. CMA. CMA recognizes obesity as a disease https://www.cma.ca/En/Pages/cma-
recognizes-obesity-as-a-disease.aspx. [8 May, 2016].
41. Burton PR, Yap K, Brown WA, Laurie C, O’Donnell M, Hebbard G, Kalff V, O’Brien
PE. Changes in satiety, supra- and infraband transit, and gastric emptying following 61. Cohen MA, Ellis SM, Le Roux CW, Batterham RL, Park A, Patterson M, Frost GS,
laparoscopic adjustable gastric banding: a prospective follow-up study. Obes Surg 21: Ghatei MA, Bloom SR. Oxyntomodulin suppresses appetite and reduces food intake
217–223, 2011. doi:10.1007/s11695-010-0312-y. in humans. J Clin Endocrinol Metab 88: 4696 – 4701, 2003. doi:10.1210/jc.2003-
030421.
43. Bustos-Saldaña R, Alfaro-Rodríguez M, Solís-Ruiz ML, Trujillo-Hernández B, Pacheco-
Carrasco M, Vázquez-Jiménez C, Celis-de la Rosa AJ. [Taste sensitivity diminution in 62. Coluzzi I, Raparelli L, Guarnacci L, Paone E, Del Genio G, le Roux CW, Silecchia G.
hyperglycemic type 2 diabetics patients]. Rev Med Inst Mex Seguro Soc 47: 483– 488, Food Intake and Changes in Eating Behavior After Laparoscopic Sleeve Gastrectomy.
2009. Obes Surg 26: 2059 –2067, 2016. doi:10.1007/s11695-015-2043-6.
44. Cabanac M. Regulation and the ponderostat. Int J Obes Relat Metab Disord 25, Suppl 5: 63. Considine RV, Sinha MK, Heiman ML, Kriauciunas A, Stephens TW, Nyce MR, Ohan-
S7–S12, 2001. doi:10.1038/sj.ijo.0801904. nesian JP, Marco CC, McKee LJ, Bauer TL, Caro JF. Serum immunoreactive-leptin
concentrations in normal-weight and obese humans. N Engl J Med 334: 292–295,
45. Cai G, Cole SA, Bastarrachea-Sosa RA, Maccluer JW, Blangero J, Comuzzie AG.
1996. doi:10.1056/NEJM199602013340503.
Quantitative trait locus determining dietary macronutrient intakes is located on hu-
man chromosome 2p22. Am J Clin Nutr 80: 1410 –1414, 2004. doi:10.1093/ajcn/80. 64. Cordier-Bussat M, Bernard C, Levenez F, Klages N, Laser-Ritz B, Philippe J, Chayvialle
5.1410. J-A, Cuber J-C. Peptones stimulate both the secretion of the incretin hormone glu-
cagon-like peptide 1 and the transcription of the proglucagon gene. Diabetes 47:
46. Carlin AM, Zeni TM, English WJ, Hawasli AA, Genaw JA, Krause KR, Schram JL, Kole
1038 –1045, 1998. doi:10.2337/diabetes.47.7.1038.
KL, Finks JF, Birkmeyer JD, Share D, Birkmeyer NJ; Michigan Bariatric Surgery Col-
laborative. The comparative effectiveness of sleeve gastrectomy, gastric bypass, and 65. Couce ME, Burguera B, Parisi JE, Jensen MD, Lloyd RV. Localization of leptin receptor
adjustable gastric banding procedures for the treatment of morbid obesity. Ann Surg in the human brain. Neuroendocrinology 66: 145–150, 1997. doi:10.1159/000127232.
257: 791–797, 2013. doi:10.1097/SLA.0b013e3182879ded.
66. Couceyro PR, Evans C, McKinzie A, Mitchell D, Dube M, Hagshenas L, White FJ,
47. Cartwright M, Wardle J, Steggles N, Simon AE, Croker H, Jarvis MJ. Stress and dietary Douglass J, Richards WG, Bannon AW. Cocaine- and amphetamine-regulated tran-
practices in adolescents. Health Psychol 22: 362–369, 2003. doi:10.1037/0278-6133. script (CART) peptides modulate the locomotor and motivational properties of psy-
22.4.362. chostimulants. J Pharmacol Exp Ther 315: 1091–1100, 2005. doi:10.1124/jpet.105.
091678.
48. Cazzo E, Pareja JC, Chaim EA, Geloneze B, Barreto MR, Magro DO. GLP-1 and
GLP-2 Levels Are Correlated with Satiety Regulation After Roux-en-Y Gastric Bypass:
67. Coughlin K, Bell RM, Bivins BA, Wrobel S, Griffen WO Jr. Preoperative and
Results of an Exploratory Prospective Study. Obes Surg 27: 703–708, 2017. doi:10.
postoperative assessment of nutrient intakes in patients who have undergone
1007/s11695-016-2345-3.
gastric bypass surgery. Arch Surg 118: 813– 816, 1983. doi:10.1001/archsurg.1983.
49. Chambers AP, Smith EP, Begg DP, Grayson BE, Sisley S, Greer T, Sorrell J, Lemmen 01390070025006.
L, LaSance K, Woods SC, Seeley RJ, D’Alessio DA, Sandoval DA. Regulation of gastric
68. Cryan JF, Dinan TG. Mind-altering microorganisms: the impact of the gut microbiota
emptying rate and its role in nutrient-induced GLP-1 secretion in rats after vertical
on brain and behaviour. Nat Rev Neurosci 13: 701–712, 2012. doi:10.1038/nrn3346.
sleeve gastrectomy. Am J Physiol Endocrinol Metab 306: E424 –E432, 2014. doi:10.
1152/ajpendo.00469.2013. 69. Cummings DE, Frayo RS, Marmonier C, Aubert R, Chapelot D. Plasma ghrelin levels
and hunger scores in humans initiating meals voluntarily without time- and food-
50. Chang S-H, Stoll CR, Song J, Varela JE, Eagon CJ, Colditz GA. The effectiveness and
related cues. Am J Physiol Endocrinol Metab 287: E297–E304, 2004. doi:10.1152/
risks of bariatric surgery: an updated systematic review and meta-analysis, 2003-2012.
ajpendo.00582.2003.
JAMA Surg 149: 275–287, 2014. doi:10.1001/jamasurg.2013.3654.
70. Dar MS, Chapman WH III, Pender JR, Drake AJ III, O’Brien K, Tanenberg RJ, Dohm
51. Chaput JP, Drapeau V, Hetherington M, Lemieux S, Provencher V, Tremblay A.
GL, Pories WJ. GLP-1 response to a mixed meal: what happens 10 years after Roux-
Psychobiological effects observed in obese men experiencing body weight loss pla-
en-Y gastric bypass (RYGB)? Obes Surg 22: 1077–1083, 2012. doi:10.1007/s11695-
teau. Depress Anxiety 24: 518 –521, 2007. doi:10.1002/da.20264.
012-0624-1.
52. Chiang JY. Bile acids: regulation of synthesis. J Lipid Res 50: 1955–1966, 2009. doi:10.
1194/jlr.R900010-JLR200. 71. Das SK, Gilhooly CH, Golden JK, Pittas AG, Fuss PJ, Cheatham RA, Tyler S, Tsay M,
McCrory MA, Lichtenstein AH, Dallal GE, Dutta C, Bhapkar MV, Delany JP, Saltzman
53. Chiu CJ, Birch DW, Shi X, Karmali S. Outcomes of the adjustable gastric band in a E, Roberts SB. Long-term effects of 2 energy-restricted diets differing in glycemic load
publicly funded obesity program. Can J Surg 56: 233–236, 2013. doi:10.1503/cjs. on dietary adherence, body composition, and metabolism in CALERIE: a 1-y random-
002712. ized controlled trial. Am J Clin Nutr 85: 1023–1030, 2007. doi:10.1093/ajcn/85.4.1023.
54. Cho M, Kaidar-Person O, Szomstein S, Rosenthal RJ. Emergency room visits after 72. Dawes C, Watanabe S. The effect of taste adaptation on salivary flow rate
laparoscopic Roux-en-Y gastric bypass for morbid obesity. Surg Obes Relat Dis 4: and salivary sugar clearance. J Dent Res 66: 740 –744, 1987. doi:10.1177/
104 –109, 2008. doi:10.1016/j.soard.2007.05.008. 00220345870660030701.
1134 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
74. Degen L, Oesch S, Casanova M, Graf S, Ketterer S, Drewe J, Beglinger C. Effect of 93. Ello-Martin JA, Roe LS, Ledikwe JH, Beach AM, Rolls BJ. Dietary energy density in the
peptide YY3-36 on food intake in humans. Gastroenterology 129: 1430 –1436, 2005. treatment of obesity: a year-long trial comparing 2 weight-loss diets. Am J Clin Nutr 85:
doi:10.1053/j.gastro.2005.09.001. 1465–1477, 2007. doi:10.1093/ajcn/85.6.1465.
75. Delgado-Aros S, Cremonini F, Castillo JE, Chial HJ, Burton DD, Ferber I, Camilleri M. 94. Elson AE, Dotson CD, Egan JM, Munger SD. Glucagon signaling modulates sweet taste
Independent influences of body mass and gastric volumes on satiation in humans. responsiveness. FASEB J 24: 3960 –3969, 2010. doi:10.1096/fj.10-158105.
Gastroenterology 126: 432– 440, 2004. doi:10.1053/j.gastro.2003.11.007.
95. Epstein LH, Paluch R, Coleman KJ. Differences in salivation to repeated food cues in
76. Desor JA, Maller O, Andrews K. Ingestive responses of human newborns to salty, obese and nonobese women. Psychosom Med 58: 160 –164, 1996. doi:10.1097/
sour, and bitter stimuli. J Comp Physiol Psychol 89: 966 –970, 1975. doi:10.1037/ 00006842-199603000-00011.
h0077171.
96. Ernst B, Thurnheer M, Wilms B, Schultes B. Differential changes in dietary habits after
77. DeWys WD, Walters K. Abnormalities of taste sensation in cancer patients. gastric bypass versus gastric banding operations. Obes Surg 19: 274 –280, 2009. doi:
Cancer 36: 1888 –1896, 1975. doi:10.1002/1097-0142(197511)36:5⬍1888::AID- 10.1007/s11695-008-9769-3.
CNCR2820360546⬎3.0.CO;2-Y.
97. Ervin GN, Mosher JT, Birkemo LS, Johnson MF. Multiple, small doses of cholecysto-
78. Di Marzo V, Melck D, Bisogno T, De Petrocellis L. Endocannabinoids: endogenous kinin octapeptide are more efficacious at inducing taste aversion conditioning than
cannabinoid receptor ligands with neuromodulatory action. Trends Neurosci 21: 521– single, large doses. Peptides 16: 539 –545, 1995. doi:10.1016/0196-9781(95)00001-Z.
528, 1998. doi:10.1016/S0166-2236(98)01283-1.
98. Escartín-Pérez RE, Cendejas-Trejo NM, Cruz-Martínez AM, González-Hernández B,
79. Dirksen C, Jørgensen NB, Bojsen-Møller KN, Kielgast U, Jacobsen SH, Clausen TR, Mancilla-Díaz JM, Florán-Garduño B. Role of cannabinoid CB1 receptors on macro-
Worm D, Hartmann B, Rehfeld JF, Damgaard M, Madsen JL, Madsbad S, Holst JJ, nutrient selection and satiety in rats. Physiol Behav 96: 646 – 650, 2009. doi:10.1016/
Hansen DL. Gut hormones, early dumping and resting energy expenditure in patients j.physbeh.2008.12.017.
with good and poor weight loss response after Roux-en-Y gastric bypass. Int J Obes 37:
1452–1459, 2013. doi:10.1038/ijo.2013.15. 99. Evans JM, Morris LS, Marchesi JR. The gut microbiome: the role of a virtual organ in
the endocrinology of the host. J Endocrinol 218: R37–R47, 2013. doi:10.1530/JOE-13-
80. Dockray GJ. Gastrointestinal hormones and the dialogue between gut and brain. J 0131.
Physiol 592: 2927–2941, 2014. doi:10.1113/jphysiol.2014.270850.
100. Fabbi F. Gustatory sense modifications in diabetes. Nasen-und Kehlkopfheilkunde 164:
81. Donahey JC, van Dijk G, Woods SC, Seeley RJ. Intraventricular GLP-1 reduces short- 543–546, 1954. doi:10.1007/BF02105163.
but not long-term food intake or body weight in lean and obese rats. Brain Res 779:
75– 83, 1998. doi:10.1016/S0006-8993(97)01057-3. 101. Faulconbridge LF, Ruparel K, Loughead J, Allison KC, Hesson LA, Fabricatore AN,
Rochette A, Ritter S, Hopson RD, Sarwer DB, Williams NN, Geliebter A, Gur RC,
82. Dotson CD, Geraedts MC, Munger SD. Peptide regulators of peripheral taste func- Wadden TA. Changes in neural responsivity to highly palatable foods following roux-
tion. In: Seminars in Cell & Developmental Biology. New York: Elsevier, 2013, p. 232– en-Y gastric bypass, sleeve gastrectomy, or weight stability: an fMRI study. Obesity
239. (Silver Spring) 24: 1054 –1060, 2016. doi:10.1002/oby.21464.
83. Doucet E, Imbeault P, St-Pierre S, Alméras N, Mauriège P, Richard D, Tremblay A. 102. Feng X-H, Liu X-M, Zhou L-H, Wang J, Liu G-D. Expression of glucagon-like pep-
Appetite after weight loss by energy restriction and a low-fat diet-exercise follow-up. tide-1 in the taste buds of rat circumvallate papillae. Acta Histochem 110: 151–154,
Int J Obes Relat Metab Disord 24: 906 –914, 2000. doi:10.1038/sj.ijo.0801251. 2008. doi:10.1016/j.acthis.2007.10.005.
84. Doucet E, St-Pierre S, Alméras N, Tremblay A. Relation between appetite ratings 103. Fenske WK, Bueter M, Miras AD, Ghatei MA, Bloom SR, le Roux CW. Exogenous
before and after a standard meal and estimates of daily energy intake in obese and peptide YY3-36 and Exendin-4 further decrease food intake, whereas octreotide
reduced obese individuals. Appetite 40: 137–143, 2003. doi:10.1016/S0195- increases food intake in rats after Roux-en-Y gastric bypass. Int J Obes 36: 379 –384,
6663(02)00143-5. 2012. doi:10.1038/ijo.2011.126.
85. Dovey TM, Dovey T. Eating Behaviour. London: McGraw-Hill Education, 2010. 104. Fetissov SO. Role of the gut microbiota in host appetite control: bacterial growth to
animal feeding behaviour. Nat Rev Endocrinol 13: 11–25, 2017. doi:10.1038/nrendo.
86. Drapeau V, King N, Hetherington M, Doucet E, Blundell J, Tremblay A. Appetite 2016.150.
sensations and satiety quotient: predictors of energy intake and weight loss. Appetite
48: 159 –166, 2007. doi:10.1016/j.appet.2006.08.002. 105. Flint A, Raben A, Astrup A, Holst JJ. Glucagon-like peptide 1 promotes satiety and
suppresses energy intake in humans. J Clin Invest 101: 515–520, 1998. doi:10.1172/
87. Dutia R, Embrey M, O’Brien CS, Haeusler RA, Agénor KK, Homel P, McGinty J, JCI990.
Vincent RP, Alaghband-Zadeh J, Staels B, le Roux CW, Yu J, Laferrère B. Temporal
changes in bile acid levels and 12␣-hydroxylation after Roux-en-Y gastric bypass 106. Fobi MA, Lee H, Felahy B, Che K, Ako P, Fobi N. Choosing an operation for weight
surgery in type 2 diabetes. Int J Obes 39: 806 – 813, 2015. doi:10.1038/ijo.2015.1. control, and the transected banded gastric bypass. Obes Surg 15: 114 –121, 2005.
doi:10.1381/0960892052993404.
88. Egecioglu E, Jerlhag E, Salomé N, Skibicka KP, Haage D, Bohlooly-Y M, Andersson D,
Bjursell M, Perrissoud D, Engel JA, Dickson SL. Ghrelin increases intake of rewarding 107. Forsythe P, Sudo N, Dinan T, Taylor VH, Bienenstock J. Mood and gut feelings. Brain
food in rodents. Addict Biol 15: 304 –311, 2010. doi:10.1111/j.1369-1600.2010. Behav Immun 24: 9 –16, 2010. doi:10.1016/j.bbi.2009.05.058.
00216.x.
108. Franco JVA, Ruiz PA, Palermo M, Gagner M. A review of studies comparing three
89. Ekman P, Rosenberg EL. What the Face Reveals: Basic and Applied Studies of Sponta- laparoscopic procedures in bariatric surgery: sleeve gastrectomy, Roux-en-Y gastric
neous Expression Using the Facial Action Coding System (FACS). New York: Oxford bypass and adjustable gastric banding. Obes Surg 21: 1458 –1468, 2011. doi:10.1007/
Univ. Press, 1997. s11695-011-0390-5.
90. El Labban S, Safadi B, Olabi A. The Effect of Roux-en-Y Gastric Bypass and Sleeve 109. Friedman JM, Halaas JL. Leptin and the regulation of body weight in mammals. Nature
Gastrectomy Surgery on Dietary Intake, Food Preferences, and Gastrointestinal 395: 763–770, 1998. doi:10.1038/27376.
Symptoms in Post-Surgical Morbidly Obese Lebanese Subjects: A Cross-Sectional
Pilot Study. Obes Surg 25: 2393–2399, 2015. doi:10.1007/s11695-015-1713-8. 110. Froehlich DA, Pangborn RM, Whitaker JR. The effect of oral stimulation on human
parotid salivary flow rate and alpha-amylase secretion. Physiol Behav 41: 209 –217,
91. Elliot K. Nutritional considerations after bariatric surgery. Crit Care Nurs Q 26: 133– 1987. doi:10.1016/0031-9384(87)90355-6.
138, 2003. doi:10.1097/00002727-200304000-00007.
111. Furet J-P, Kong L-C, Tap J, Poitou C, Basdevant A, Bouillot J-L, Mariat D, Corthier G,
92. Elliott RM, Morgan LM, Tredger JA, Deacon S, Wright J, Marks V. Glucagon-like Doré J, Henegar C, Rizkalla S, Clément K. Differential adaptation of human gut
peptide-1 (7-36)amide and glucose-dependent insulinotropic polypeptide secretion microbiota to bariatric surgery-induced weight loss: links with metabolic and low-
in response to nutrient ingestion in man: acute post-prandial and 24-h secretion grade inflammation markers. Diabetes 59: 3049 –3057, 2010. doi:10.2337/db10-
patterns. J Endocrinol 138: 159 –166, 1993. doi:10.1677/joe.0.1380159. 0253.
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1135
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
112. Furnes MW, Stenström B, Tømmerås K, Skoglund T, Dickson SL, Kulseng B, Zhao 133. Harris GC, Wimmer M, Aston-Jones G. A role for lateral hypothalamic orexin neurons
C-M, Chen D. Feeding behavior in rats subjected to gastrectomy or gastric bypass in reward seeking. Nature 437: 556 –559, 2005. doi:10.1038/nature04071.
surgery. Eur Surg Res 40: 279 –288, 2008. doi:10.1159/000114966.
134. Harrold JA, Dovey TM, Blundell JE, Halford JC. CNS regulation of appetite. Neuro-
113. Geraedts MC, Munger SD. Gustatory stimuli representing different perceptual qual- pharmacology 63: 3–17, 2012. doi:10.1016/j.neuropharm.2012.01.007.
ities elicit distinct patterns of neuropeptide secretion from taste buds. J Neurosci 33:
7559 –7564, 2013. doi:10.1523/JNEUROSCI.0372-13.2013. 135. Havel PJ. Peripheral signals conveying metabolic information to the brain: short-term
and long-term regulation of food intake and energy homeostasis. Exp Biol Med (May-
114. Gibbs J, Young RC, Smith GP. Cholecystokinin elicits satiety in rats with open gastric wood) 226: 963–977, 2001. doi:10.1177/153537020122601102.
fistulas. Nature 245: 323–325, 1973. doi:10.1038/245323a0.
136. Heath TP, Melichar JK, Nutt DJ, Donaldson LF. Human taste thresholds are modu-
115. Goldstone AP, Miras AD, Scholtz S, Jackson S, Neff KJ, Pénicaud L, Geoghegan J, lated by serotonin and noradrenaline. J Neurosci 26: 12664 –12671, 2006. doi:10.
Chhina N, Durighel G, Bell JD, Meillon S, le Roux CW. Link between increased satiety 1523/JNEUROSCI.3459-06.2006.
gut hormones and reduced food reward after gastric bypass surgery for obesity. J Clin
Endocrinol Metab 101: 599 – 609, 2016. doi:10.1210/jc.2015-2665. 137. Henkin RI, Bartter FC. Studies on olfactory thresholds in normal man and in patients
with adrenal cortical insufficiency: the role of adrenal cortical steroids and of serum
116. Gondivkar SM, Indurkar A, Degwekar S, Bhowate R. Evaluation of gustatory function sodium concentration. J Clin Invest 45: 1631–1639, 1966. doi:10.1172/JCI105470.
in patients with diabetes mellitus type 2. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod 108: 876 – 880, 2009. doi:10.1016/j.tripleo.2009.08.015. 138. Hervey GR. Regulation of energy balance. Nature 222: 629 – 631, 1969. doi:10.1038/
222629a0.
117. Graeff FG. Role of 5-HT in defensive behavior and anxiety. Rev Neurosci 4: 181–211,
1993. doi:10.1515/REVNEURO.1993.4.2.181. 139. Himpens J, Dobbeleir J, Peeters G. Long-term results of laparoscopic sleeve
gastrectomy for obesity. Ann Surg 252: 319 –324, 2010. doi:10.1097/SLA.
118. Greene LF, Malpede CZ, Henson CS, Hubbert KA, Heimburger DC, Ard JD. Weight 0b013e3181e90b31.
maintenance 2 years after participation in a weight loss program promoting low-
energy density foods. Obesity (Silver Spring) 14: 1795–1801, 2006. doi:10.1038/oby. 140. Hirschfeld RM. History and evolution of the monoamine hypothesis of depression. J
2006.207. Clin Psychiatry 61, Suppl 6: 4 – 6, 2000.
119. Greenstein AJ, O’Rourke RW. Abdominal pain after gastric bypass: suspects and 141. Hodos W. Progressive ratio as a measure of reward strength. Science 134: 943–944,
solutions. Am J Surg 201: 819 – 827, 2011. doi:10.1016/j.amjsurg.2010.05.007. 1961. doi:10.1126/science.134.3483.943.
120. Griffen WO Jr, Young VL, Stevenson CC. A prospective comparison of gastric and 142. Hoggard N, Mercer JG, Rayner DV, Moar K, Trayhurn P, Williams LM. Localization of
jejunoileal bypass procedures for morbid obesity. Ann Surg 186: 500 –509, 1977. leptin receptor mRNA splice variants in murine peripheral tissues by RT-PCR and in
doi:10.1097/00000658-197710000-00012. situ hybridization. Biochem Biophys Res Commun 232: 383–387, 1997. doi:10.1006/
bbrc.1997.6245.
121. Grill HJ, Berridge KC. Taste reactivity as a measure of the neural control of palatabil-
ity. Prog Psychobiol Physiol Psychol 11: 1– 61, 1985. 143. Holzer P, Reichmann F, Farzi A. Neuropeptide Y, peptide YY and pancreatic poly-
peptide in the gut-brain axis. Neuropeptides 46: 261–274, 2012. doi:10.1016/j.npep.
122. Grill HJ, Norgren R. The taste reactivity test. I. Mimetic responses to gustatory stimuli 2012.08.005.
in neurologically normal rats. Brain Res 143: 263–279, 1978. doi:10.1016/0006-
8993(78)90568-1. 144. Horder J, Harmer CJ, Cowen PJ, McCabe C. Reduced neural response to reward
following 7 days treatment with the cannabinoid CB1 antagonist rimonabant in
123. Gudzune KA, Huizinga MM, Chang H-Y, Asamoah V, Gadgil M, Clark JM. Screening healthy volunteers. Int J Neuropsychopharmacol 13: 1103–1113, 2010. doi:10.1017/
and diagnosis of micronutrient deficiencies before and after bariatric surgery. Obes S1461145710000453.
Surg 23: 1581–1589, 2013. doi:10.1007/s11695-013-0919-x.
145. Hüttl TP, Obeidat FW, Parhofer KG, Zügel N, Hüttl PE, Jauch K-W, Lang RA. Oper-
124. Gutierrez R, Simon SA. Chemosensory processing in the taste-reward pathway. Fla- ative Techniken und deren Outcome in der metabolischen Chirurgie: Sleeve-Gas-
vour Fragrance J 26: 231–238, 2011. doi:10.1002/ffj.2050. trektomie. Zentralbl Chir 134: 24 –31, 2009. doi:10.1055/s-0028-1098811.
125. Gutzwiller J-P, Drewe J, Göke B, Schmidt H, Rohrer B, Lareida J, Beglinger C. Glu- 146. Hyde KM, Blonde GD, le Roux CW, Spector AC. Liraglutide suppression of caloric
cagon-like peptide-1 promotes satiety and reduces food intake in patients with dia- intake competes with the intake-promoting effects of a palatable cafeteria diet, but
betes mellitus type 2. Am J Physiol Regul Integr Comp Physiol 276: R1541–R1544, 1999. does not impact food or macronutrient selection. Physiol Behav 177: 4 –12, 2017.
doi:10.1016/j.physbeh.2017.03.045.
126. Guy-Grand B, Goga H. Conditioned salivation in obese subjects with different weight
kinetics. Appetite 2: 351–355, 1981. doi:10.1016/S0195-6663(81)80020-7. 147. Jacobs HL. Studies on sugar preference. I. The preference for glucose solutions and its
modification by injections of insulin. J Comp Physiol Psychol 51: 304 –310, 1958. doi:
127. Habib AM, Richards P, Cairns LS, Rogers GJ, Bannon CA, Parker HE, Morley TC, Yeo 10.1037/h0046679.
GS, Reimann F, Gribble FM. Overlap of endocrine hormone expression in the mouse
intestine revealed by transcriptional profiling and flow cytometry. Endocrinology 153: 148. Jordan N. Role of Thought, Sight, Smell, and Taste of Food in the Cephalic Phase of
3054 –3065, 2012. doi:10.1210/en.2011-2170. Gastric Acid Secretion in Humans M. FELDMAN AND CT RICHARDSON Gastro-
enterology 90: 428 –33, 1986. Nutr Clin Pract 1: 221–222, 1986. doi:10.1177/
128. Hagan MM, Rushing PA, Benoit SC, Woods SC, Seeley RJ. Opioid receptor involve- 088453368600100411.
ment in the effect of AgRP- (83-132) on food intake and food selection. Am J Physiol
Regul Integr Comp Physiol 280: R814 –R821, 2001. doi:10.1152/ajpregu.2001.280.3. 148a.Jurowich CF, Seyfried F, Miras AD, Bueter M, Deckelmann J, Fassnacht M, Germer
R814. CT, Thalheimer A. Does bariatric surgery change olfactory perception? Results of the
early postoperative course. Int J Colorectal Dis 29: 253–260, 2014. doi:10.1007/
129. Halatchev IG, Cone RD. Peripheral administration of PYY(3-36) produces condi- s00384-013-1795-5.
tioned taste aversion in mice. Cell Metab 1: 159 –168, 2005. doi:10.1016/j.cmet.2005.
02.003. 149. Kalra SP, Dube MG, Pu S, Xu B, Horvath TL, Kalra PS. Interacting appetite-regulating
pathways in the hypothalamic regulation of body weight. Endocr Rev 20: 68 –100,
130. Halmi KA, Mason E, Falk JR, Stunkard A. Appetitive behavior after gastric bypass for 1999.
obesity. Int J Obes 5: 457– 464, 1981.
150. Karamanakos SN, Vagenas K, Kalfarentzos F, Alexandrides TK. Weight loss, appetite
131. Hansen G, Jelsing J, Vrang N. Effects of liraglutide and sibutramine on food intake, suppression, and changes in fasting and postprandial ghrelin and peptide-YY levels
palatability, body weight and glucose tolerance in the gubra DIO-rats. Acta Pharmacol after Roux-en-Y gastric bypass and sleeve gastrectomy: a prospective, double blind
Sin 33: 194 –200, 2012. doi:10.1038/aps.2011.168. study. Ann Surg 247: 401– 407, 2008. doi:10.1097/SLA.0b013e318156f012.
132. Hao Z, Mumphrey MB, Morrison CD, Münzberg H, Ye J, Berthoud HR. Does gastric 151. Kawai K, Sugimoto K, Nakashima K, Miura H, Ninomiya Y. Leptin as a modulator of
bypass surgery change body weight set point? Int J Obes Suppl 6, Suppl 1: S37–S43, sweet taste sensitivities in mice. Proc Natl Acad Sci USA 97: 11044 –11049, 2000.
2016. doi:10.1038/ijosup.2016.9. doi:10.1073/pnas.190066697.
1136 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
152. Kenler HA, Brolin RE, Cody RP. Changes in eating behavior after horizontal gastro- 172. Liddle RA, Goldfine ID, Rosen MS, Taplitz RA, Williams JA. Cholecystokinin bioactivity
plasty and Roux-en-Y gastric bypass. Am J Clin Nutr 52: 87–92, 1990. doi:10.1093/ajcn/ in human plasma. Molecular forms, responses to feeding, and relationship to gallblad-
52.1.87. der contraction. J Clin Invest 75: 1144 –1152, 1985. doi:10.1172/JCI111809.
154. Kerr AC. The physiological regulation of salivary secretions in man. A study of the 173. Lier HØ, Aastrom S, Rørtveit K. Patients’ daily life experiences five years after gastric
response of human salivary glands to reflex stimulation. Int Ser Monogr Oral Biol 1: bypass surgery–a qualitative study. J Clin Nurs 25: 322–331, 2016. doi:10.1111/jocn.
1–12, 1961. 13049.
155. Kieffer TJ, Heller RS, Leech CA, Holz GG, Habener JF. Leptin suppression of insulin 174. Liou AP, Paziuk M, Luevano JM Jr, Machineni S, Turnbaugh PJ, Kaplan LM. Conserved
secretion by the activation of ATP-sensitive K⫹ channels in pancreatic -cells. Diabe- shifts in the gut microbiota due to gastric bypass reduce host weight and adiposity. Sci
tes 46: 1087–1093, 1997. doi:10.2337/diab.46.6.1087. Transl Med 5: 178ra41, 2013. doi:10.1126/scitranslmed.3005687.
156. Kohli R, Bradley D, Setchell KD, Eagon JC, Abumrad N, Klein S. Weight loss induced 175. Lord GM, Matarese G, Howard JK, Baker RJ, Bloom SR, Lechler RI. Leptin modulates
by Roux-en-Y gastric bypass but not laparoscopic adjustable gastric banding increases the T-cell immune response and reverses starvation-induced immunosuppression.
circulating bile acids. J Clin Endocrinol Metab 98: E708 –E712, 2013. doi:10.1210/jc. Nature 394: 897–901, 1998. doi:10.1038/29795.
2012-3736.
176. Lorentzen M, Madsbad S, Kehlet H, Tronier B. Effect of sham-feeding on glucose
157. Korner J, Bessler M, Cirilo LJ, Conwell IM, Daud A, Restuccia NL, Wardlaw SL. Effects tolerance and insulin secretion. Acta Endocrinol (Copenh) 115: 84 – 86, 1987.
of Roux-en-Y gastric bypass surgery on fasting and postprandial concentrations of
177. Macfarlane GT, Macfarlane S. Bacteria, colonic fermentation, and gastrointestinal
plasma ghrelin, peptide YY, and insulin. J Clin Endocrinol Metab 90: 359 –365, 2005. health. J AOAC Int 95: 50 – 60, 2012. doi:10.5740/jaoacint.SGE_Macfarlane.
doi:10.1210/jc.2004-1076.
178. MacLean PS, Bergouignan A, Cornier M-A, Jackman MR. Biology’s response to diet-
158. Korner J, Inabnet W, Conwell IM, Taveras C, Daud A, Olivero-Rivera L, Restuccia NL, ing: the impetus for weight regain. Am J Physiol Regul Integr Comp Physiol 301: R581–
Bessler M. Differential effects of gastric bypass and banding on circulating gut hor- R600, 2011. doi:10.1152/ajpregu.00755.2010.
mone and leptin levels. Obesity (Silver Spring) 14: 1553–1561, 2006. doi:10.1038/oby.
2006.179. 179. Maffei M, Halaas J, Ravussin E, Pratley RE, Lee GH, Zhang Y, Fei H, Kim S, Lallone R,
Ranganathan S, Kern PA, Friedman JM. Leptin levels in human and rodent: measure-
159. Kotz CM, Grace MK, Briggs J, Levine AS, Billington CJ. Effects of opioid antagonists ment of plasma leptin and ob RNA in obese and weight-reduced subjects. Nat Med 1:
naloxone and naltrexone on neuropeptide Y-induced feeding and brown fat thermo- 1155–1161, 1995. doi:10.1038/nm1195-1155.
genesis in the rat. Neural site of action. J Clin Invest 96: 163–170, 1995. doi:10.1172/
JCI118017. 180. Magouliotis DE, Tasiopoulou VS, Sioka E, Chatedaki C, Zacharoulis D. Impact of
Bariatric Surgery on Metabolic and Gut Microbiota Profile: a Systematic Review and
160. Kraschnewski JL, Boan J, Esposito J, Sherwood NE, Lehman EB, Kephart DK, Scia- Meta-analysis. Obes Surg 27: 1345–1357, 2017. doi:10.1007/s11695-017-2595-8.
manna CN. Long-term weight loss maintenance in the United States. Int J Obes 34:
1644 –1654, 2010. doi:10.1038/ijo.2010.94. 181. Makaronidis JM, Neilson S, Cheung W-H, Tymoszuk U, Pucci A, Finer N, Doyle J,
Hashemi M, Elkalaawy M, Adamo M, Jenkinson A, Batterham RL. Reported appetite,
161. Kruseman M, Leimgruber A, Zumbach F, Golay A. Dietary, weight, and psychological taste and smell changes following Roux-en-Y gastric bypass and sleeve gastrectomy:
changes among patients with obesity, 8 years after gastric bypass. J Am Diet Assoc 110: effect of gender, type 2 diabetes and relationship to post-operative weight loss.
527–534, 2010. doi:10.1016/j.jada.2009.12.028. Appetite 107: 93–105, 2016. doi:10.1016/j.appet.2016.07.029.
162. Kuzmak LI, Yap IS, McGuire L, Dixon JS, Young MP. Surgery for morbid obesity. Using 182. Mei MH, Chen Q. [Interaction of vagal stimulation and duodenal acidification in the
an inflatable gastric band. AORN J 51: 1307–1324, 1990. doi:10.1016/S0001- regulation of pancreatic secretion]. Sheng Li Xue Bao 37: 410 – 415, 1985.
2092(07)70154-0.
183. Mason EE, Ito C. Gastric bypass in obesity. Surg Clin North Am 47: 1345–1351, 1967.
163. Laurenius A, Larsson I, Bueter M, Melanson KJ, Bosaeus I, Forslund HB, Lönroth H, doi:10.1016/S0039-6109(16)38384-0.
Fändriks L, Olbers T. Changes in eating behaviour and meal pattern following Roux-
184. Mathes CM, Bohnenkamp RA, Blonde GD, Letourneau C, Corteville C, Bueter M,
en-Y gastric bypass. Int J Obes 36: 348 –355, 2012. doi:10.1038/ijo.2011.217.
Lutz TA, le Roux CW, Spector AC. Gastric bypass in rats does not decrease appetitive
164. Laurenius A, Larsson I, Melanson KJ, Lindroos AK, Lönroth H, Bosaeus I, Olbers T. behavior towards sweet or fatty fluids despite blunting preferential intake of sugar and
Decreased energy density and changes in food selection following Roux-en-Y gastric fat. Physiol Behav 142: 179 –188, 2015. doi:10.1016/j.physbeh.2015.02.004.
bypass. Eur J Clin Nutr 67: 168 –173, 2013. doi:10.1038/ejcn.2012.208.
185. Mathes CM, Bueter M, Smith KR, Lutz TA, le Roux CW, Spector AC. Roux-en-Y
165. Le Roux CW, Aylwin SJ, Batterham RL, Borg CM, Coyle F, Prasad V, Shurey S, Ghatei gastric bypass in rats increases sucrose taste-related motivated behavior independent
MA, Patel AG, Bloom SR. Gut hormone profiles following bariatric surgery favor an of pharmacological GLP-1-receptor modulation. Am J Physiol Regul Integr Comp Physiol
anorectic state, facilitate weight loss, and improve metabolic parameters. Ann Surg 302: R751–R767, 2012. doi:10.1152/ajpregu.00214.2011.
243: 108 –114, 2006. doi:10.1097/01.sla.0000183349.16877.84.
186. Mathes CM, Ferrara M, Rowland NE. Cannabinoid-1 receptor antagonists reduce
166. Le Roux CW, Bueter M, Theis N, Werling M, Ashrafian H, Löwenstein C, Athanasiou caloric intake by decreasing palatable diet selection in a novel dessert protocol in
female rats. Am J Physiol Regul Integr Comp Physiol 295: R67–R75, 2008. doi:10.1152/
T, Bloom SR, Spector AC, Olbers T, Lutz TA. Gastric bypass reduces fat intake and
ajpregu.00150.2008.
preference. Am J Physiol Regul Integr Comp Physiol 301: R1057–R1066, 2011. doi:10.
1152/ajpregu.00139.2011. 187. Mathes CM, Letourneau C, Blonde GD, le Roux CW, Spector AC. Roux-en-Y gastric
bypass in rats progressively decreases the proportion of fat calories selected from a
168. Le Roux CW, Welbourn R, Werling M, Osborne A, Kokkinos A, Laurenius A, Lönroth
palatable cafeteria diet. Am J Physiol Regul Integr Comp Physiol 310: R952–R959, 2016.
H, Fändriks L, Ghatei MA, Bloom SR, Olbers T. Gut hormones as mediators of
doi:10.1152/ajpregu.00444.2015.
appetite and weight loss after Roux-en-Y gastric bypass. Ann Surg 246: 780 –785, 2007.
doi:10.1097/SLA.0b013e3180caa3e3. 188. Mathis C, Moran TH, Schwartz GJ. Load-sensitive rat gastric vagal afferents encode
volume but not gastric nutrients. Am J Physiol Regul Integr Comp Physiol 274: R280 –
169. Ledikwe JH, Rolls BJ, Smiciklas-Wright H, Mitchell DC, Ard JD, Champagne C,
R286, 1998.
Karanja N, Lin P-H, Stevens VJ, Appel LJ. Reductions in dietary energy density are
associated with weight loss in overweight and obese participants in the PREMIER trial. 189. Mattes RD. Oral fat exposure alters postprandial lipid metabolism in humans. Am J Clin
Am J Clin Nutr 85: 1212–1221, 2007. doi:10.1093/ajcn/85.5.1212. Nutr 63: 911–917, 1996.
170. Lee PC, Dixon J. Medical devices for the treatment of obesity. Nat Rev Gastroenterol 190. Mattes RD. Physiologic responses to sensory stimulation by food: nutritional implica-
Hepatol 14: 553–564, 2017. doi:10.1038/nrgastro.2017.80. tions. J Am Diet Assoc 97: 406 – 413, 1997. doi:10.1016/S0002-8223(97)00101-6.
171. Levitsky DA. The non-regulation of food intake in humans: hope for reversing the 191. Meguid MM, Glade MJ, Middleton FA. Weight regain after Roux-en-Y: a significant
epidemic of obesity. Physiol Behav 86: 623– 632, 2005. doi:10.1016/j.physbeh.2005. 20% complication related to PYY. Nutrition 24: 832– 842, 2008. doi:10.1016/j.nut.
08.053. 2008.06.027.
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1137
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
192. Melissas J, Daskalakis M, Koukouraki S, Askoxylakis I, Metaxari M, Dimitriadis E, 211. Neff KJ, Baud G, Raverdy V, Caiazzo R, Verkindt H, Noel C, le Roux CW, Pattou F.
Stathaki M, Papadakis JA. Sleeve gastrectomy–a “food limiting” operation. Obes Surg Renal Function and Remission of Hypertension After Bariatric Surgery: a 5-Year Pro-
18: 1251–1256, 2008. doi:10.1007/s11695-008-9634-4. spective Cohort Study. Obes Surg 27: 613– 619, 2017. doi:10.1007/s11695-016-
2333-7.
193. Merchenthaler I. Neurons with access to the general circulation in the central nervous
system of the rat: a retrograde tracing study with fluoro-gold. Neuroscience 44: 655– 212. Nielsen MS, Christensen BJ, Ritz C, Rasmussen S, Hansen TT, Bredie WLP, le Roux
662, 1991. doi:10.1016/0306-4522(91)90085-3. CW, Sjödin A, Schmidt JB. Roux-En-Y Gastric Bypass and Sleeve Gastrectomy Does
Not Affect Food Preferences When Assessed by an Ad libitum Buffet Meal. Obes Surg
194. Mingrone G, Panunzi S, De Gaetano A, Guidone C, Iaconelli A, Nanni G, Castagneto
27: 2599 –2605, 2017. doi:10.1007/s11695-017-2678-6.
M, Bornstein S, Rubino F. Bariatric-metabolic surgery versus conventional medical
treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, 213. Nirenberg TD, Miller PM. Salivation: an assessment of food craving? Behav Res Ther
single-centre, randomised controlled trial. Lancet 386: 964 –973, 2015. doi:10.1016/ 20: 405– 407, 1982. doi:10.1016/0005-7967(82)90102-4.
S0140-6736(15)00075-6.
214. O’Brien PE, McPhail T, Chaston TB, Dixon JB. Systematic review of medium-term
195. Miras AD, le Roux CW. Can medical therapy mimic the clinical efficacy or physiolog- weight loss after bariatric operations. Obes Surg 16: 1032–1040, 2006. doi:10.1381/
ical effects of bariatric surgery? Int J Obes 38: 325–333, 2014. doi:10.1038/ijo.2013. 096089206778026316.
205.
215. Ochner CN, Kwok Y, Conceição E, Pantazatos SP, Puma LM, Carnell S, Teixeira J,
196. Miras AD, Jackson RN, Jackson SN, Goldstone AP, Olbers T, Hackenberg T, Spector Hirsch J, Geliebter A. Selective reduction in neural responses to high calorie foods
AC, le Roux CW. Gastric bypass surgery for obesity decreases the reward value of a following gastric bypass surgery. Ann Surg 253: 502–507, 2011. doi:10.1097/SLA.
sweet-fat stimulus as assessed in a progressive ratio task. Am J Clin Nutr 96: 467– 473,
0b013e318203a289.
2012. doi:10.3945/ajcn.112.036921.
216. Ochner CN, Stice E, Hutchins E, Afifi L, Geliebter A, Hirsch J, Teixeira J. Relation
197. Miras AD, le Roux CW. Bariatric surgery and taste: novel mechanisms of weight loss.
between changes in neural responsivity and reductions in desire to eat high-calorie
Curr Opin Gastroenterol 26: 140 –145, 2010. doi:10.1097/MOG.0b013e328333e94a.
foods following gastric bypass surgery. Neuroscience 209: 128 –135, 2012. doi:10.
198. Miras AD, le Roux CW. Mechanisms underlying weight loss after bariatric surgery. Nat 1016/j.neuroscience.2012.02.030.
Rev Gastroenterol Hepatol 10: 575–584, 2013. doi:10.1038/nrgastro.2013.119.
217. Olbers T, Björkman S, Lindroos A, Maleckas A, Lönn L, Sjöström L, Lönroth H. Body
199. Moizé V, Andreu A, Flores L, Torres F, Ibarzabal A, Delgado S, Lacy A, Rodriguez L, composition, dietary intake, and energy expenditure after laparoscopic Roux-en-Y
Vidal J. Long-term dietary intake and nutritional deficiencies following sleeve gastrec- gastric bypass and laparoscopic vertical banded gastroplasty: a randomized clinical
tomy or Roux-En-Y gastric bypass in a Mediterranean population. J Acad Nutr Diet trial. Ann Surg 244: 715–722, 2006. doi:10.1097/01.sla.0000218085.25902.f8.
113: 400 – 410, 2013. doi:10.1016/j.jand.2012.11.013.
218. Olbers T, Lönroth H, Fagevik-Olsén M, Lundell L. Laparoscopic gastric bypass: de-
200. Moize V, Geliebter A, Gluck ME, Yahav E, Lorence M, Colarusso T, Drake V, velopment of technique, respiratory function, and long-term outcome. Obes Surg 13:
Flancbaum L. Obese patients have inadequate protein intake related to protein intol- 364 –370, 2003. doi:10.1381/096089203765887679.
erance up to 1 year following Roux-en-Y gastric bypass. Obes Surg 13: 23–28, 2003.
doi:10.1381/096089203321136548. 219. Onyike CU, Crum RM, Lee HB, Lyketsos CG, Eaton WW. Is obesity associated with
major depression? Results from the Third National Health and Nutrition Examination
201. Molin Netto BD, Earthman CP, Farias G, Landi Masquio DC, Grotti Clemente AP, Survey. Am J Epidemiol 158: 1139 –1147, 2003. doi:10.1093/aje/kwg275.
Peixoto P, Bettini SC, von Der Heyde ME, Dâmaso AR. Eating patterns and food
choice as determinant of weight loss and improvement of metabolic profile after 220. Pagotto U, Marsicano G, Cota D, Lutz B, Pasquali R. The emerging role of the
RYGB. Nutrition 33: 125–131, 2017. doi:10.1016/j.nut.2016.05.007. endocannabinoid system in endocrine regulation and energy balance. Endocr Rev 27:
73–100, 2006. doi:10.1210/er.2005-0009.
202. Monneuse M-O, Rigal N, Frelut M-L, Hladik C-M, Simmen B, Pasquet P. Taste acuity
of obese adolescents and changes in food neophobia and food preferences during a 221. Parker LA. Taste avoidance and taste aversion: evidence for two different processes.
weight reduction session. Appetite 50: 302–307, 2008. doi:10.1016/j.appet.2007.08. Learn Behav 31: 165–172, 2003. doi:10.3758/BF03195979.
004.
222. Parker LA, Mechoulam R, Schlievert C. Cannabidiol, a non-psychoactive component
203. Moreira FA, Crippa JAS. The psychiatric side-effects of rimonabant. Rev Bras Psiquiatr of cannabis and its synthetic dimethylheptyl homolog suppress nausea in an experi-
31: 145–153, 2009. doi:10.1590/S1516-44462009000200012. mental model with rats. Neuroreport 13: 567–570, 2002. doi:10.1097/00001756-
200204160-00006.
204. Morínigo R, Moizé V, Musri M, Lacy AM, Navarro S, Marín JL, Delgado S, Casamitjana
R, Vidal J. Glucagon-like peptide-1, peptide YY, hunger, and satiety after gastric bypass 223. Patti ME, Houten SM, Bianco AC, Bernier R, Larsen PR, Holst JJ, Badman MK, Mara-
surgery in morbidly obese subjects. J Clin Endocrinol Metab 91: 1735–1740, 2006. tos-Flier E, Mun EC, Pihlajamaki J, Auwerx J, Goldfine AB. Serum bile acids are higher
doi:10.1210/jc.2005-0904. in humans with prior gastric bypass: potential contribution to improved glucose and
lipid metabolism. Obesity (Silver Spring) 17: 1671–1677, 2009. doi:10.1038/oby.2009.
205. Morton GJ, Cummings DE, Baskin DG, Barsh GS, Schwartz MW. Central nervous 102.
system control of food intake and body weight. Nature 443: 289 –295, 2006. doi:10.
1038/nature05026. 224. Pepino MY, Bradley D, Eagon JC, Sullivan S, Abumrad NA, Klein S. Changes in taste
perception and eating behavior after bariatric surgery-induced weight loss in women.
206. Morton GJ, Schwartz MW. Leptin and the central nervous system control of glucose
Obesity (Silver Spring) 22: E13–E20, 2014. doi:10.1002/oby.20649.
metabolism. Physiol Rev 91: 389 – 411, 2011. doi:10.1152/physrev.00007.2010.
225. Peterli R, Borbély Y, Kern B, Gass M, Peters T, Thurnheer M, Schultes B, Laederach
207. Mrosovsky N, Powley TL. Set points for body weight and fat. Behav Biol 20: 205–223,
K, Bueter M, Schiesser M. Early results of the Swiss Multicentre Bypass or Sleeve
1977. doi:10.1016/S0091-6773(77)90773-8.
Study (SM-BOSS): a prospective randomized trial comparing laparoscopic sleeve gas-
208. Nadreau E, Baraboi ED, Samson P, Blouin A, Hould FS, Marceau P, Biron S, Richard D. trectomy and Roux-en-Y gastric bypass. Ann Surg 258: 690 – 695, 2013. doi:10.1097/
Effects of the biliopancreatic diversion on energy balance in the rat. Int J Obes 30: SLA.0b013e3182a67426.
419 – 429, 2006. doi:10.1038/sj.ijo.0803166.
226. Peterli R, Wölnerhanssen B, Peters T, Devaux N, Kern B, Christoffel-Courtin C,
209. Navarro M, Rodriquez de Fonseca F, Alvarez E, Chowen JA, Zueco JA, Gomez R, Eng Drewe J, von Flüe M, Beglinger C. Improvement in glucose metabolism after bariatric
J, Blázquez E. Colocalization of glucagon-like peptide-1 (GLP-1) receptors, glucose surgery: comparison of laparoscopic Roux-en-Y gastric bypass and laparoscopic
transporter GLUT-2, and glucokinase mRNAs in rat hypothalamic cells: evidence for sleeve gastrectomy: a prospective randomized trial. Ann Surg 250: 234 –241, 2009.
a role of GLP-1 receptor agonists as an inhibitory signal for food and water intake. J doi:10.1097/SLA.0b013e3181ae32e3.
Neurochem 67: 1982–1991, 1996. doi:10.1046/j.1471-4159.1996.67051982.x.
227. Peters CT, Choi Y-H, Brubaker PL, Anderson GH. A glucagon-like peptide-1 recep-
210. Nederkoorn C, Smulders FT, Jansen A. Cephalic phase responses, craving and food tor agonist and an antagonist modify macronutrient selection by rats. J Nutr 131:
intake in normal subjects. Appetite 35: 45–55, 2000. doi:10.1006/appe.2000.0328. 2164 –2170, 2001. doi:10.1093/jn/131.8.2164.
1138 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
228. Phillips RJ, Powley TL. Gastric volume rather than nutrient content inhibits food 247. Roslin MS, Dudiy Y, Weiskopf J, Damani T, Shah P. Comparison between RYGB, DS,
intake. Am J Physiol Regul Integr Comp Physiol 271: R766 –R769, 1996. and VSG effect on glucose homeostasis. Obes Surg 22: 1281–1286, 2012. doi:10.1007/
s11695-012-0686-0.
229. Polonsky KS, Given BD, Van Cauter E. Twenty-four-hour profiles and pulsatile pat-
terns of insulin secretion in normal and obese subjects. J Clin Invest 81: 442– 448, 1988. 248. Russell-Jones D, Gough S. Recent advances in incretin-based therapies. Clin Endocrinol
doi:10.1172/JCI113339. (Oxf) 77: 489 – 499, 2012. doi:10.1111/j.1365-2265.2012.04483.x.
230. Pournaras DJ, Glicksman C, Vincent RP, Kuganolipava S, Alaghband-Zadeh J, Mahon 249. Saeidi N, Nestoridi E, Kucharczyk J, Uygun MK, Yarmush ML, Stylopoulos N. Sleeve
D, Bekker JH, Ghatei MA, Bloom SR, Walters JR, Welbourn R, le Roux CW. The role gastrectomy and Roux-en-Y gastric bypass exhibit differential effects on food prefer-
of bile after Roux-en-Y gastric bypass in promoting weight loss and improving glycae- ences, nutrient absorption and energy expenditure in obese rats. Int J Obes 36: 1396 –
mic control. Endocrinology 153: 3613–3619, 2012. doi:10.1210/en.2011-2145. 1402, 2012. doi:10.1038/ijo.2012.167.
232. Pournaras DJ, le Roux CW. After bariatric surgery, what vitamins should be measured 250. Santoro S. From bariatric to pure metabolic surgery: new concepts on the rise. Ann
and what supplements should be given? Clin Endocrinol (Oxf) 71: 322–325, 2009. Surg 262: e79 – e80, 2015. doi:10.1097/SLA.0000000000000590.
doi:10.1111/j.1365-2265.2009.03564.x.
251. Saper CB, Chou TC, Elmquist JK. The need to feed: homeostatic and hedonic control
233. Pournaras DJ, Osborne A, Hawkins SC, Mahon D, Ghatei MA, Bloom SR, Welbourn of eating. Neuron 36: 199 –211, 2002. doi:10.1016/S0896-6273(02)00969-8.
R, le Roux CW. The gut hormone response following Roux-en-Y gastric bypass:
cross-sectional and prospective study. Obes Surg 20: 56 – 60, 2010. doi:10.1007/ 252. Sarkhosh K, Switzer NJ, El-Hadi M, Birch DW, Shi X, Karmali S. The impact of
s11695-009-9989-1. bariatric surgery on obstructive sleep apnea: a systematic review. Obes Surg 23:
414 – 423, 2013. doi:10.1007/s11695-012-0862-2.
234. Powley TL. The ventromedial hypothalamic syndrome, satiety, and a cephalic phase
253. Sawchenko PE. Central connections of the sensory and motor nuclei of the vagus
hypothesis. Psychol Rev 84: 89 –126, 1977. doi:10.1037/0033-295X.84.1.89.
nerve. J Auton Nerv Syst 9: 13–26, 1983. doi:10.1016/0165-1838(83)90129-7.
235. Primeaux SD, Tzeng TH, Allerton TD, Chiang MC, Cosentino G, Dubin RL,
254. Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Aminian A, Brethauer SA, Navaneethan
Varughese A, Moore R, Geiselman PJ, Greenway FL, Uwaifo GI. Differences in short-
SD, Singh RP, Pothier CE, Nissen SE, Kashyap SR; STAMPEDE Investigators. Bariatric
term food preferences following vertical sleeve gastrectomy and Roux-en-Y gastric
Surgery versus Intensive Medical Therapy for Diabetes–5-Year Outcomes. N Engl J
bypass surgery. Obes Res Clin Pract 9: 628 – 632, 2015. doi:10.1016/j.orcp.2015.09.
Med 376: 641– 651, 2017. doi:10.1056/NEJMoa1600869.
003.
255. Schelling J-L, Tétreault L, Lasagna L, Davis M. Abnormal taste threshold in diabetes.
236. Rasmussen EB, Huskinson SL. Effects of rimonabant on behavior maintained by pro-
Lancet 258: 508 –511, 1965. doi:10.1016/S0140-6736(65)92017-9.
gressive ratio schedules of sucrose reinforcement in obese Zucker (fa/fa) rats. Behav
Pharmacol 19: 735–742, 2008. doi:10.1097/FBP.0b013e3283123cc2. 256. Scholtz S, Miras AD, Chhina N, Prechtl CG, Sleeth ML, Daud NM, Ismail NA, Durighel
G, Ahmed AR, Olbers T, Vincent RP, Alaghband-Zadeh J, Ghatei MA, Waldman AD,
237. Raun K, von Voss P, Gotfredsen CF, Golozoubova V, Rolin B, Knudsen LB. Liraglutide,
Frost GS, Bell JD, le Roux CW, Goldstone AP. Obese patients after gastric bypass
a long-acting glucagon-like peptide-1 analog, reduces body weight and food intake in
surgery have lower brain-hedonic responses to food than after gastric banding. Gut
obese candy-fed rats, whereas a dipeptidyl peptidase-IV inhibitor, vildagliptin, does
63: 891–902, 2014. doi:10.1136/gutjnl-2013-305008.
not. Diabetes 56: 8 –15, 2007. doi:10.2337/db06-0565.
257. Schultes B, Ernst B, Wilms B, Thurnheer M, Hallschmid M. Hedonic hunger is in-
238. Reddingius J. Control theory and the dynamics of body weight. Physiol Behav 24:
creased in severely obese patients and is reduced after gastric bypass surgery. Am J
27–32, 1980. doi:10.1016/0031-9384(80)90009-8.
Clin Nutr 92: 277–283, 2010. doi:10.3945/ajcn.2009.29007.
239. Richardson BE, Vanderwoude EA, Sudan R, Leopold DA, Thompson JS. Gastric by-
258. Schwartz MW, Woods SC, Porte D Jr, Seeley RJ, Baskin DG. Central nervous system
pass does not influence olfactory function in obese patients. Obes Surg 22: 283–286,
control of food intake. Nature 404: 661– 671, 2000. doi:10.1038/35007534.
2012. doi:10.1007/s11695-011-0487-x.
259. Sclafani A. Conditioned food preferences and appetite. Appetite 17: 71–72, 1991.
240. Richardson CT, Feldman M. Salivary response to food in humans and its effect on
doi:10.1016/0195-6663(91)90087-9.
gastric acid secretion. Am J Physiol Gastrointest Liver Physiol 250: G85–G91, 1986.
260. Sclafani A. Learned controls of ingestive behaviour. Appetite 29: 153–158, 1997.
241. Ritzel U, Fromme A, Ottleben M, Leonhardt U, Ramadori G. Release of glucagon-like
doi:10.1006/appe.1997.0120.
peptide-1 (GLP-1) by carbohydrates in the perfused rat ileum. Acta Diabetol 34:
18 –21, 1997. doi:10.1007/s005920050059. 261. Sclafani A, Koopmans HS. Intestinal bypass surgery produces conditioned taste aver-
sion in rats. Int J Obes 5: 497–500, 1981.
242. Roberts RE, Glicksman C, Alaghband-Zadeh J, Sherwood RA, Akuji N, le Roux CW.
The relationship between postprandial bile acid concentration, GLP-1, PYY and ghre- 262. Scott KM, McGee MA, Wells JE, Oakley Browne MA. Obesity and mental disorders in
lin. Clin Endocrinol (Oxf) 74: 67–72, 2011. doi:10.1111/j.1365-2265.2010.03886.x. the adult general population. J Psychosom Res 64: 97–105, 2008. doi:10.1016/j.
jpsychores.2007.09.006.
243. Robertson MD, Jackson KG, Williams CM, Fielding BA, Frayn KN. Prolonged effects
of modified sham feeding on energy substrate mobilization. Am J Clin Nutr 73: 111– 263. Scott WR, Batterham RL. Roux-en-Y gastric bypass and laparoscopic sleeve gastrec-
117, 2001. doi:10.1093/ajcn/73.1.111. tomy: understanding weight loss and improvements in type 2 diabetes after bariatric
surgery. Am J Physiol Regul Integr Comp Physiol 301: R15–R27, 2011. doi:10.1152/
244. Rocca AS, Brubaker PL. Stereospecific effects of fatty acids on proglucagon-derived ajpregu.00038.2011.
peptide secretion in fetal rat intestinal cultures. Endocrinology 136: 5593–5599, 1995.
doi:10.1210/endo.136.12.7588313. 264. Scruggs DM, Buffington C, Cowan GS Jr. Taste acuity of the morbidly obese before
and after gastric bypass surgery. Obes Surg 4: 24 –28, 1994. doi:10.1381/
244a.Rodriquez de Fonseca F, Navarro M, Alvarez E, Roncero I, Chowen JA, Maestre O, 096089294765558854.
Gómez R, Muñoz RM, Eng J, Blázquez E. Peripheral versus central effects of glucagon-
like peptide-1 receptor agonists on satiety and body weight loss in Zucker obese rats. 265. Seyfried F, Miras AD, Bueter M, Prechtl CG, Spector AC, le Roux CW. Effects of
Metabolism 49: 709 –717, 2000. doi:10.1053/meta.2000.6251. preoperative exposure to a high-fat versus a low-fat diet on ingestive behavior after
gastric bypass surgery in rats. Surg Endosc 27: 4192– 4201, 2013. doi:10.1007/s00464-
245. Rolls BJ, Roe LS, Beach AM, Kris-Etherton PM. Provision of foods differing in energy 013-3020-6.
density affects long-term weight loss. Obes Res 13: 1052–1060, 2005. doi:10.1038/
oby.2005.123. 267. Shimbara T, Mondal MS, Kawagoe T, Toshinai K, Koda S, Yamaguchi H, Date Y,
Nakazato M. Central administration of ghrelin preferentially enhances fat ingestion.
246. Romanova IV, Ramos EJ, Xu Y, Quinn R, Chen C, George ZM, Inui A, Das U, Meguid Neurosci Lett 369: 75–79, 2004. doi:10.1016/j.neulet.2004.07.060.
MM. Neurobiologic changes in the hypothalamus associated with weight loss after
gastric bypass. J Am Coll Surg 199: 887– 895, 2004. doi:10.1016/j.jamcollsurg.2004.07. 268. Shin AC, Zheng H, Pistell PJ, Berthoud H-R. Roux-en-Y gastric bypass surgery changes
013. food reward in rats. Int J Obes 35: 642– 651, 2011. doi:10.1038/ijo.2010.174.
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1139
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
AL-NAJIM ET AL.
269. Shin IH, Park DC, Kwon C, Yeo SG. Changes in taste function related to obesity and 287. Stefater MA, Pérez-Tilve D, Chambers AP, Wilson-Pérez HE, Sandoval DA, Berger J,
chronic otitis media with effusion. Arch Otolaryngol Head Neck Surg 137: 242–246, Toure M, Tschöp M, Woods SC, Seeley RJ. Sleeve gastrectomy induces loss of weight
2011. doi:10.1001/archoto.2011.23. and fat mass in obese rats, but does not affect leptin sensitivity. Gastroenterology 138:
2426 –2436.e3, 2010. doi:10.1053/j.gastro.2010.02.059.
270. Shin Y-K, Martin B, Kim W, White CM, Ji S, Sun Y, Smith RG, Sévigny J, Tschöp MH,
Maudsley S, Egan JM. Ghrelin is produced in taste cells and ghrelin receptor null mice 288. Stefater MA, Sandoval DA, Chambers AP, Wilson-Pérez HE, Hofmann SM, Jandacek
show reduced taste responsivity to salty (NaCl) and sour (citric acid) tastants. PLoS R, Tso P, Woods SC, Seeley RJ. Sleeve gastrectomy in rats improves postprandial lipid
One 5: e12729, 2010. doi:10.1371/journal.pone.0012729. clearance by reducing intestinal triglyceride secretion. Gastroenterology 141: 939 –
949.e4, 2011. doi:10.1053/j.gastro.2011.05.008.
271. Siegel EG, Trimble ER, Renold AE, Berthoud HR. Importance of preabsorptive insulin
release on oral glucose tolerance: studies in pancreatic islet transplanted rats. Gut 21: 289. Steiner JE. Facial expressions of the neonate infant indicating the hedonics of
1002–1009, 1980. doi:10.1136/gut.21.11.1002. food-related chemical stimuli. In: Taste and Development: The Genesis of Sweet
Preference, edited by Weiffenbach JM. Bethesda, MD: NIH, 1977, p.
272. Simchen U, Koebnick C, Hoyer S, Issanchou S, Zunft H-J. Odour and taste sensitivity 173–188.
is associated with body weight and extent of misreporting of body weight. Eur J Clin
Nutr 60: 698 –705, 2006. doi:10.1038/sj.ejcn.1602371. 290. Steiner JE, Rosenthal-Zifroni A, Edelstein EL. Taste perception in depressive illness. Isr
Ann Psychiatr Relat Discip 7: 223–232, 1969.
273. Simonen M, Dali-Youcef N, Kaminska D, Venesmaa S, Käkelä P, Pääkkönen M, Hal-
likainen M, Kolehmainen M, Uusitupa M, Moilanen L, Laakso M, Gylling H, Patti ME, 291. Stolbová K, Hahn A, Benes B, Andel M, Treslová L. Gustometry of diabetes mellitus
Auwerx J, Pihlajamäki J. Conjugated bile acids associate with altered rates of glucose patients and obese patients. Int Tinnitus J 5: 135–140, 1999.
and lipid oxidation after Roux-en-Y gastric bypass. Obes Surg 22: 1473–1480, 2012.
doi:10.1007/s11695-012-0673-5. 293. Sugerman HJ, Starkey JV, Birkenhauer R. A randomized prospective trial of gastric
bypass versus vertical banded gastroplasty for morbid obesity and their effects on
274. Sink KS, Vemuri VK, Olszewska T, Makriyannis A, Salamone JD. Cannabinoid CB1 sweets versus non-sweets eaters. Ann Surg 205: 613– 624, 1987. doi:10.1097/
antagonists and dopamine antagonists produce different effects on a task involving 00000658-198706000-00002.
response allocation and effort-related choice in food-seeking behavior. Psychophar-
macology (Berl) 196: 565–574, 2008. doi:10.1007/s00213-007-0988-4. 294. Sumithran P, Prendergast LA, Delbridge E, Purcell K, Shulkes A, Kriketos A, Proietto
J. Long-term persistence of hormonal adaptations to weight loss. N Engl J Med 365:
275. Sjöström L. Review of the key results from the Swedish Obese Subjects (SOS) trial–a 1597–1604, 2011. doi:10.1056/NEJMoa1105816.
prospective controlled intervention study of bariatric surgery. J Intern Med 273: 219 –
234, 2013. doi:10.1111/joim.12012. 295. Suzuki K, Jayasena CN, Bloom SR. Obesity and appetite control. Exp Diabetes Res
2012: 824305, 2012. doi:10.1155/2012/824305.
276. Sjöström L, Lindroos A-K, Peltonen M, Torgerson J, Bouchard C, Carlsson B, Dahl-
gren S, Larsson B, Narbro K, Sjöström CD, Sullivan M, Wedel H; Swedish Obese 296. Svane MS, Jørgensen NB, Bojsen-Møller KN, Dirksen C, Nielsen S, Kristiansen VB,
Subjects Study Scientific Group. Lifestyle, diabetes, and cardiovascular risk factors 10 Toräng S, Wewer Albrechtsen NJ, Rehfeld JF, Hartmann B, Madsbad S, Holst JJ.
years after bariatric surgery. N Engl J Med 351: 2683–2693, 2004. doi:10.1056/ Peptide YY and glucagon-like peptide-1 contribute to decreased food intake after
NEJMoa035622. Roux-en-Y gastric bypass surgery. Int J Obes 40: 1699 –1706, 2016. doi:10.1038/ijo.
2016.121.
277. Sjöström L, Peltonen M, Jacobson P, Sjöström CD, Karason K, Wedel H, Ahlin S,
Anveden Å, Bengtsson C, Bergmark G, Bouchard C, Carlsson B, Dahlgren S, Karlsson 297. Tack J, Arts J, Caenepeel P, De Wulf D, Bisschops R. Pathophysiology, diagnosis and
J, Lindroos AK, Lönroth H, Narbro K, Näslund I, Olbers T, Svensson PA, Carlsson LM. management of postoperative dumping syndrome. Nat Rev Gastroenterol Hepatol 6:
Bariatric surgery and long-term cardiovascular events. JAMA 307: 56 – 65, 2012. doi: 583–590, 2009. doi:10.1038/nrgastro.2009.148.
10.1001/jama.2011.1914.
298. Takai S, Yasumatsu K, Inoue M, Iwata S, Yoshida R, Shigemura N, Yanagawa Y,
278. Smith JC. The history of the “Davis Rig”. Appetite 36: 93–98, 2001. doi:10.1006/appe. Drucker DJ, Margolskee RF, Ninomiya Y. Glucagon-like peptide-1 is specifically in-
2000.0372. volved in sweet taste transmission. FASEB J 29: 2268 –2280, 2015. doi:10.1096/fj.14-
265355.
279. Smith JE, Friedman MI, Andrews PLR. Conditioned food aversion in Suncus murinus
(house musk shrew): a new model for the study of nausea in a species with an emetic 299. Tan T, Behary P, Tharakan G, Minnion J, Al-Najim W, Albrechtsen NJW, Holst JJ,
reflex. Physiol Behav 73: 593–598, 2001. doi:10.1016/S0031-9384(01)00538-8. Bloom SR. The effect of a subcutaneous infusion of GLP-1, OXM and PYY on Energy
intake and Expenditure in Obese volunteers. J Clin Endocrinol Metab 102: 2364 –2372,
280. Snyder-Marlow G, Taylor D, Lenhard MJ. Nutrition care for patients undergoing 2017. doi:10.1210/jc.2017-00469.
laparoscopic sleeve gastrectomy for weight loss. J Am Diet Assoc 110: 600 – 607, 2010.
doi:10.1016/j.jada.2009.12.022. 300. Teff K. Nutritional implications of the cephalic-phase reflexes: endocrine responses.
Appetite 34: 206 –213, 2000. doi:10.1006/appe.1999.0282.
281. Sobhani I, Bado A, Vissuzaine C, Buyse M, Kermorgant S, Laigneau JP, Attoub S, Lehy
T, Henin D, Mignon M, Lewin MJ. Leptin secretion and leptin receptor in the human 301. Teff KL, Levin BE, Engelman K. Oral sensory stimulation in men: effects on insulin,
stomach. Gut 47: 178 –183, 2000. doi:10.1136/gut.47.2.178. C-peptide, and catecholamines. Am J Physiol Regul Integr Comp Physiol 265: R1223–
R1230, 1993.
282. Spector AC. Linking gustatory neurobiology to behavior in vertebrates. Neurosci
Biobehav Rev 24: 391– 416, 2000. doi:10.1016/S0149-7634(00)00013-0. 302. Teff KL, Mattes RD, Engelman K. Cephalic phase insulin release in normal weight
males: verification and reliability. Am J Physiol Endocrinol Metab 261: E430 –E436,
283. Spector AC, Glendinning JI. Linking peripheral taste processes to behavior. Curr Opin 1991.
Neurobiol 19: 370 –377, 2009. doi:10.1016/j.conb.2009.07.014.
303. Temple JL, Giacomelli AM, Roemmich JN, Epstein LH. Overweight children habituate
284. Stacher G, Steinringer H, Schmierer G, Schneider C, Winklehner S. Cholecystokinin slower than non-overweight children to food. Physiol Behav 91: 250 –254, 2007. doi:
octapeptide decreases intake of solid food in man. Peptides 3: 133–136, 1982. doi:10. 10.1016/j.physbeh.2007.03.009.
1016/0196-9781(82)90041-9.
304. Tichansky DS, Glatt AR, Madan AK, Harper J, Tokita K, Boughter JD. Decrease in
285. Stanley BG, Daniel DR, Chin AS, Leibowitz SF. Paraventricular nucleus injections of sweet taste in rats after gastric bypass surgery. Surg Endosc 25: 1176 –1181, 2011.
peptide YY and neuropeptide Y preferentially enhance carbohydrate ingestion. Pep- doi:10.1007/s00464-010-1335-0.
tides 6: 1205–1211, 1985. doi:10.1016/0196-9781(85)90452-8.
305. Tremaroli V, Karlsson F, Werling M, Ståhlman M, Kovatcheva-Datchary P, Olbers T,
286. Stefanidis A, Forrest N, Brown WA, Dixon JB, O’Brien PB, Juliane Kampe, Oldfield BJ. Fändriks L, le Roux CW, Nielsen J, Bäckhed F. Roux-en-Y Gastric Bypass and Vertical
An investigation of the neural mechanisms underlying the efficacy of the adjustable Banded Gastroplasty Induce Long-Term Changes on the Human Gut Microbiome
gastric band. Surg Obes Relat Dis 12: 828 – 838, 2016. doi:10.1016/j.soard.2015.11. Contributing to Fat Mass Regulation. Cell Metab 22: 228 –238, 2015. doi:10.1016/j.
020. cmet.2015.07.009.
1140 Physiol Rev • VOL 98 • JULY 2018 • www.prv.org
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
BARIATRIC SURGERY, FOOD INTAKE, AND BEHAVIOR
306. Trostler N, Mann A, Zilberbush N, Avinoach E, Charuzi I. Weight Loss and Food 322. Welzl H, D’Adamo P, Lipp H-P. Conditioned taste aversion as a learning and
Intake 18 Months Following Vertical Banded Gastroplasty or Gastric Bypass for Se- memory paradigm. Behav Brain Res 125: 205–213, 2001. doi:10.1016/S0166-
vere Obesity. Obes Surg 5: 39 –51, 1995. doi:10.1381/096089295765558141. 4328(01)00302-3.
307. Tung YC, Rimmington D, O’Rahilly S, Coll AP. Pro-opiomelanocortin modulates the 323. Wetzler S, Dumaz V, Goubern M, Tomé D, Larue-Achagiotis C. Intraperitoneal leptin
thermogenic and physical activity responses to high-fat feeding and markedly influ- modifies macronutrient choice in self-selecting rats. Physiol Behav 83: 65–72, 2004.
ences dietary fat preference. Endocrinology 148: 5331–5338, 2007. doi:10.1210/en. doi:10.1016/S0031-9384(04)00311-7.
2007-0797.
324. Whishaw IQ. The Behavior of the Laboratory Rat: A Handbook with Tests: A Handbook
308. Turnbaugh PJ, Ley RE, Mahowald MA, Magrini V, Mardis ER, Gordon JI. An obesity- With Tests. New York: Oxford Univ. Press, 2004. doi:10.1093/acprof:oso/
associated gut microbiome with increased capacity for energy harvest. Nature 444: 9780195162851.001.0001.
1027–1031, 2006. doi:10.1038/nature05414. 325. Wilson-Pérez HE, Chambers AP, Sandoval DA, Stefater MA, Woods SC, Benoit SC,
Seeley RJ. The effect of vertical sleeve gastrectomy on food choice in rats. Int J Obes
309. Turton MD, O’Shea D, Gunn I, Beak SA, Edwards CM, Meeran K, Choi SJ, Taylor GM,
37: 288 –295, 2013. doi:10.1038/ijo.2012.18.
Heath MM, Lambert PD, Wilding JP, Smith DM, Ghatei MA, Herbert J, Bloom SR. A
role for glucagon-like peptide-1 in the central regulation of feeding. Nature 379: 326. Wirtshafter D, Davis JD. Set points, settling points, and the control of body weight.
69 –72, 1996. doi:10.1038/379069a0. Physiol Behav 19: 75–78, 1977. doi:10.1016/0031-9384(77)90162-7.
310. Umabiki M, Tsuzaki K, Kotani K, Nagai N, Sano Y, Matsuoka Y, Kitaoka K, Okami Y, 327. Wisén O, Björvell H, Cantor P, Johansson C, Theodorsson E. Plasma concentrations
Sakane N, Higashi A. The improvement of sweet taste sensitivity with decrease in of regulatory peptides in obesity following modified sham feeding (MSF) and a liquid
serum leptin levels during weight loss in obese females. Tohoku J Exp Med 220: 267– test meal. Regul Pept 39: 43–54, 1992. doi:10.1016/0167-0115(92)90007-H.
271, 2010. doi:10.1620/tjem.220.267.
328. Woods SC, D’Alessio DA. Central control of body weight and appetite. J Clin Endo-
311. Valassi E, Scacchi M, Cavagnini F. Neuroendocrine control of food intake. Nutr Metab crinol Metab 93, Suppl 1: S37–S50, 2008. doi:10.1210/jc.2008-1630.
Cardiovasc Dis 18: 158 –168, 2008. doi:10.1016/j.numecd.2007.06.004.
329. Woods SC, Lutz TA, Geary N, Langhans W. Pancreatic signals controlling food intake;
312. Valderas JP, Irribarra V, Boza C, de la Cruz R, Liberona Y, Acosta AM, Yolito M, Maiz insulin, glucagon and amylin. Philos Trans R Soc Lond B Biol Sci 361: 1219 –1235, 2006.
A. Medical and surgical treatments for obesity have opposite effects on peptide YY doi:10.1098/rstb.2006.1858.
and appetite: a prospective study controlled for weight loss. J Clin Endocrinol Metab
330. Xu Y, Ohinata K, Meguid MM, Marx W, Tada T, Chen C, Quinn R, Inui A. Gastric
95: 1069 –1075, 2010. doi:10.1210/jc.2009-0983.
bypass model in the obese rat to study metabolic mechanisms of weight loss. J Surg Res
313. Vigneshwaran B, Wahal A, Aggarwal S, Priyadarshini P, Bhattacharjee H, Khadgawat 107: 56 – 63, 2002. doi:10.1016/S0022-4804(02)96508-X.
R, Yadav R. Impact of Sleeve Gastrectomy on Type 2 Diabetes Mellitus, Gastric 331. Ye J, Hao Z, Mumphrey MB, Townsend RL, Patterson LM, Stylopoulos N, Münzberg
Emptying Time, Glucagon-Like Peptide 1 (GLP-1), Ghrelin and Leptin in Non-mor- H, Morrison CD, Drucker DJ, Berthoud H-R. GLP-1 receptor signaling is not required
bidly Obese Subjects with BMI 30-35.0 kg/m2: a Prospective Study. Obes Surg 26: for reduced body weight after RYGB in rodents. Am J Physiol Regul Integr Comp Physiol
2817–2823, 2016. doi:10.1007/s11695-016-2226-9. 306: R352–R362, 2014. doi:10.1152/ajpregu.00491.2013.
314. Vítek L, Haluzík M. The role of bile acids in metabolic regulation. J Endocrinol 228: 332. Yeomans MR. Olfactory influences on appetite and satiety in humans. Physiol Behav 87:
R85–R96, 2016. doi:10.1530/JOE-15-0469. 800 – 804, 2006. doi:10.1016/j.physbeh.2006.01.029.
315. Von Holstein-Rathlou S, BonDurant LD, Peltekian L, Naber MC, Yin TC, Claflin KE, 333. Yoshida R, Noguchi K, Shigemura N, Jyotaki M, Takahashi I, Margolskee RF, Ninomiya
Urizar AI, Madsen AN, Ratner C, Holst B, Karstoft K, Vandenbeuch A, Anderson CB, Y. Leptin suppresses mouse taste cell responses to sweet compounds. Diabetes 64:
Cassell MD, Thompson AP, Solomon TP, Rahmouni K, Kinnamon SC, Pieper AA, 3751–3762, 2015. doi:10.2337/db14-1462.
Gillum MP, Potthoff MJ. FGF21 mediates endocrine control of simple sugar intake and
sweet taste preference by the liver. Cell Metab 23: 335–343, 2016. doi:10.1016/j. 334. Yousseif A, Emmanuel J, Karra E, Millet Q, Elkalaawy M, Jenkinson AD, Hashemi M,
cmet.2015.12.003. Adamo M, Finer N, Fiennes AG, Withers DJ, Batterham RL. Differential effects of
laparoscopic sleeve gastrectomy and laparoscopic gastric bypass on appetite, circu-
316. Wang J, Akabayashi A, Dourmashkin J, Yu HJ, Alexander JT, Chae HJ, Leibowitz SF. lating acyl-ghrelin, peptide YY3-36 and active GLP-1 levels in non-diabetic humans.
Neuropeptide Y in relation to carbohydrate intake, corticosterone and dietary obe- Obes Surg 24: 241–252, 2014. doi:10.1007/s11695-013-1066-0.
sity. Brain Res 802: 75– 88, 1998. doi:10.1016/S0006-8993(98)00551-4.
335. Zellner DA, Loaiza S, Gonzalez Z, Pita J, Morales J, Pecora D, Wolf A. Food selection
317. Wang J, Liu R, Hawkins M, Barzilai N, Rossetti L. A nutrient-sensing pathway regulates changes under stress. Physiol Behav 87: 789 –793, 2006. doi:10.1016/j.physbeh.2006.
01.014.
leptin gene expression in muscle and fat. Nature 393: 684 – 688, 1998. doi:10.1038/
31474. 336. Zhang H, DiBaise JK, Zuccolo A, Kudrna D, Braidotti M, Yu Y, Parameswaran P,
Crowell MD, Wing R, Rittmann BE, Krajmalnik-Brown R. Human gut microbiota in
318. Warne JP, Padilla BE, Horneman HF, Ginsberg AB, Pecoraro NC, Akana SF, Dallman
obesity and after gastric bypass. Proc Natl Acad Sci USA 106: 2365–2370, 2009. doi:
MF. Metabolic and neuroendocrine consequences of a duodenal-jejunal bypass in rats
10.1073/pnas.0812600106.
on a choice diet. Ann Surg 249: 269 –276, 2009. doi:10.1097/SLA.0b013e3181961d5d.
337. Zhang M, Gosnell BA, Kelley AE. Intake of high-fat food is selectively enhanced by mu
319. Wasalathanthri S, Hettiarachchi P, Prathapan S. Sweet taste sensitivity in pre-diabet- opioid receptor stimulation within the nucleus accumbens. J Pharmacol Exp Ther 285:
ics, diabetics and normoglycemic controls: a comparative cross sectional study. BMC 908 –914, 1998.
Endocr Disord 14: 67, 2014. doi:10.1186/1472-6823-14-67.
338. Zhao F-L, Shen T, Kaya N, Lu S-G, Cao Y, Herness S. Expression, physiological action,
320. Watanabe S, Dawes C. The effects of different foods and concentrations of citric acid and coexpression patterns of neuropeptide Y in rat taste-bud cells. Proc Natl Acad Sci
on the flow rate of whole saliva in man. Arch Oral Biol 33: 1–5, 1988. doi:10.1016/ USA 102: 11100 –11105, 2005. doi:10.1073/pnas.0501988102.
0003-9969(88)90089-1.
339. Zheng H, Shin AC, Lenard NR, Townsend RL, Patterson LM, Sigalet DL, Berthoud
321. Weiss EC, Galuska DA, Kettel Khan L, Gillespie C, Serdula MK. Weight regain in U.S. H-R. Meal patterns, satiety, and food choice in a rat model of Roux-en-Y gastric bypass
adults who experienced substantial weight loss, 1999-2002. Am J Prev Med 33: 34 – 40, surgery. Am J Physiol Regul Integr Comp Physiol 297: R1273–R1282, 2009.
2007. doi:10.1016/j.amepre.2007.02.040. doi:10.1152/ajpregu.00343.2009.
Physiol Rev • VOL 98 • JULY 2018 • www.prv.org 1141
Downloaded from www.physiology.org/journal/physrev by ${individualUser.givenNames} ${individualUser.surname} (163.015.154.053) on July 26, 2018.
Copyright © 2018 American Physiological Society. All rights reserved.
Vous aimerez peut-être aussi
- Scientific Evidence of Diets For Weight Loss Different Macronutrient... (BITAN ČLANAK)Document11 pagesScientific Evidence of Diets For Weight Loss Different Macronutrient... (BITAN ČLANAK)mirkoPas encore d'évaluation
- Emergency Care Algorithms 2019 PDFDocument75 pagesEmergency Care Algorithms 2019 PDFsiraj ammed75% (4)
- Clinical Chemistry Notes With BlanksDocument34 pagesClinical Chemistry Notes With Blanksepson printerPas encore d'évaluation
- Pressure Sore: GradingDocument2 pagesPressure Sore: GradingAnusha VerghesePas encore d'évaluation
- Chapter 27 Bariatric SurgeryDocument16 pagesChapter 27 Bariatric SurgeryJuan Francisco Alfayate GarcíaPas encore d'évaluation
- Ck4tzxj55reuochnn2p5ecwaDocument6 pagesCk4tzxj55reuochnn2p5ecwaMuscle Arora0% (1)
- Extended Essay Chemistry (HL) - Extraction of Citrus Essential Oil From Citrus Fruit Skin and Determination of Limonene Content and Its Antibacterial Potency: Comparative InvestigationDocument39 pagesExtended Essay Chemistry (HL) - Extraction of Citrus Essential Oil From Citrus Fruit Skin and Determination of Limonene Content and Its Antibacterial Potency: Comparative InvestigationGracielle Jesslyne CahyadiPas encore d'évaluation
- Nursing Diagnosis: Risk For Deficient Fluid Volume R/T Traumatic InjuryDocument2 pagesNursing Diagnosis: Risk For Deficient Fluid Volume R/T Traumatic Injuryarreane yookPas encore d'évaluation
- Nursing Process of PneumoniaDocument5 pagesNursing Process of Pneumoniatin2x061275% (8)
- ESPEN Guidelines On Parenteral Nutrition. Intensive Care 2009Document38 pagesESPEN Guidelines On Parenteral Nutrition. Intensive Care 2009ERINSONPas encore d'évaluation
- Nutrients 16 00419 v2Document22 pagesNutrients 16 00419 v2ela.sofiaPas encore d'évaluation
- Clinical NutritionDocument8 pagesClinical Nutritionlorenza osornioPas encore d'évaluation
- The Effects of Gastric Bypass Surgery On Drug Absorption and PharmacokineticsDocument15 pagesThe Effects of Gastric Bypass Surgery On Drug Absorption and PharmacokineticsAndrés MaldonadoPas encore d'évaluation
- Dietary Intake and Ghrelin and Leptin Changes After SleeveDocument8 pagesDietary Intake and Ghrelin and Leptin Changes After Sleevea12345644321Pas encore d'évaluation
- Effects of A Meal Replacement On Body CompositionDocument10 pagesEffects of A Meal Replacement On Body CompositionGiffariPas encore d'évaluation
- Diet and Exercise in Management of Obesity and OveDocument6 pagesDiet and Exercise in Management of Obesity and OveXavi Martinez SantamariaPas encore d'évaluation
- Treating Obesity Seriously. When Recommendations For As Recomendações Por Um Estilo de Vida São Confrontados Pelas Adaptações BiológicasDocument3 pagesTreating Obesity Seriously. When Recommendations For As Recomendações Por Um Estilo de Vida São Confrontados Pelas Adaptações BiológicasClaudia GuimarãesPas encore d'évaluation
- Iron de Ficiency After Bariatric Surgery: What Is The Real Problem?Document11 pagesIron de Ficiency After Bariatric Surgery: What Is The Real Problem?NAYARA CAETANOPas encore d'évaluation
- Approaches To Obesity Management: ClinicalperspectivesDocument6 pagesApproaches To Obesity Management: ClinicalperspectivesSandra CardosoPas encore d'évaluation
- Nutrisi in SurgeryDocument26 pagesNutrisi in Surgeryfeby ary annasPas encore d'évaluation
- Artigo - Metabolic ImpactsDocument11 pagesArtigo - Metabolic ImpactsRaissa Porta da Cruz RaissaPas encore d'évaluation
- Sinclair 2017Document10 pagesSinclair 2017Alterego RPas encore d'évaluation
- Fat Malabsorption in Critical IllnessDocument6 pagesFat Malabsorption in Critical Illnesslakshminivas PingaliPas encore d'évaluation
- 3 Potential Hormone Mechanisms of Bariatric SurgeryDocument13 pages3 Potential Hormone Mechanisms of Bariatric SurgeryJuan Luis RuizPas encore d'évaluation
- (2019) Metabolic Support Challenges With Obesity During Critical IllnessDocument8 pages(2019) Metabolic Support Challenges With Obesity During Critical IllnessAnna Maria Ariesta PutriPas encore d'évaluation
- 13 - 2017 - Nutritional Recommendations For Adult BariatricDocument13 pages13 - 2017 - Nutritional Recommendations For Adult Bariatricvictor eduardoPas encore d'évaluation
- Guidelines Metabolic IndiaDocument3 pagesGuidelines Metabolic Indiadrjohn232323Pas encore d'évaluation
- Do Gut Hormones Contribute To Weight Loss and Glycaemic Outcomes After Bariatric Surgery?Document26 pagesDo Gut Hormones Contribute To Weight Loss and Glycaemic Outcomes After Bariatric Surgery?Douglas RodriguesPas encore d'évaluation
- Unravelling The Health Effects of Fasting A Long Road From Obesity Treatment To Healthy Life Span Increase and Improved CognitionDocument16 pagesUnravelling The Health Effects of Fasting A Long Road From Obesity Treatment To Healthy Life Span Increase and Improved CognitionLarissa calvoPas encore d'évaluation
- Surgery in Morbid ObesityDocument28 pagesSurgery in Morbid ObesityalaaPas encore d'évaluation
- White Paper AGA: POWER - Practice Guide On Obesity and Weight Management, Education, and ResourcesDocument29 pagesWhite Paper AGA: POWER - Practice Guide On Obesity and Weight Management, Education, and ResourcesCin Gzlz PsicoPas encore d'évaluation
- Quick Fix or Long-Term Cure? Pros and Cons of Bariatric SurgeryDocument9 pagesQuick Fix or Long-Term Cure? Pros and Cons of Bariatric SurgeryJuan Luis RuizPas encore d'évaluation
- Gastrectomy NutritionDocument10 pagesGastrectomy NutritionBalasubramanian NatarajanPas encore d'évaluation
- Manejo Sobrep e Obesidade Pos TX. Chadban Et Al., 2010Document4 pagesManejo Sobrep e Obesidade Pos TX. Chadban Et Al., 2010Priscila MansurPas encore d'évaluation
- A Time To FastDocument7 pagesA Time To Fastangela pavaPas encore d'évaluation
- Materi Dono Indarto, DR., M. Biotech. ST., PHDDocument32 pagesMateri Dono Indarto, DR., M. Biotech. ST., PHDTaufik RacePas encore d'évaluation
- 1 s2.0 S0002916522004385 MainDocument11 pages1 s2.0 S0002916522004385 Maincarlos santamariaPas encore d'évaluation
- A Time To FastDocument7 pagesA Time To Fastubiktrash1492Pas encore d'évaluation
- 2017 Popular Weight Loss StrategiesDocument4 pages2017 Popular Weight Loss StrategiesClau ArtPas encore d'évaluation
- Reviews in Basic and Clinical GastroenterologyDocument10 pagesReviews in Basic and Clinical GastroenterologyAGkawaiPas encore d'évaluation
- Jejunoileal Shunt in Surgical Treatment of Morbid ObesityDocument11 pagesJejunoileal Shunt in Surgical Treatment of Morbid ObesityTiago VieiraPas encore d'évaluation
- Glycemic Index and Obesity: Janette C Brand-Miller, Susanna Ha Holt, Dorota B Pawlak, and Joanna McmillanDocument5 pagesGlycemic Index and Obesity: Janette C Brand-Miller, Susanna Ha Holt, Dorota B Pawlak, and Joanna McmillanSzasz Helen HenriettaPas encore d'évaluation
- MNT PaperDocument5 pagesMNT Paperapi-301959052Pas encore d'évaluation
- Worksheet2 NDTDocument5 pagesWorksheet2 NDTaudsPas encore d'évaluation
- Metabolites: Physiological Responses of Post-Dietary Effects: Lessons From Pre-Clinical and Clinical StudiesDocument16 pagesMetabolites: Physiological Responses of Post-Dietary Effects: Lessons From Pre-Clinical and Clinical StudiesSarah OctaviaPas encore d'évaluation
- Plasma Ghrelin LevelDocument8 pagesPlasma Ghrelin Levelmilenerato2240Pas encore d'évaluation
- Aktar 2017Document14 pagesAktar 2017Arsal Wildan wildanPas encore d'évaluation
- The Physiological Regulation of Body Fat Mass (Sumithran, 2023)Document16 pagesThe Physiological Regulation of Body Fat Mass (Sumithran, 2023)sunriseskzPas encore d'évaluation
- Bariatric SurgeryDocument5 pagesBariatric SurgeryMiguelito JohnsonPas encore d'évaluation
- Alimentacion Basada en PlantasDocument9 pagesAlimentacion Basada en PlantasMaria Luz KraanPas encore d'évaluation
- 10 1016@j PSC 2019 01 014Document11 pages10 1016@j PSC 2019 01 014deja234Pas encore d'évaluation
- Polydextrose and Weight ManagementDocument4 pagesPolydextrose and Weight Managementchef Sergio rojasPas encore d'évaluation
- Evidencia Científica de Dietas para Bajar de Peso Diferente Composición de Macronutrientes, Ayuno Intermitente y Dietas PopularesDocument35 pagesEvidencia Científica de Dietas para Bajar de Peso Diferente Composición de Macronutrientes, Ayuno Intermitente y Dietas PopularesCesar Flores VallePas encore d'évaluation
- Aspen - EspenDocument38 pagesAspen - EspenJake BastoPas encore d'évaluation
- Nutrients 16 01071Document35 pagesNutrients 16 01071Gabriela VazquezPas encore d'évaluation
- Jurnal DindaDocument6 pagesJurnal Dindachiendo ymPas encore d'évaluation
- Addressing Obesity in DiabetesDocument11 pagesAddressing Obesity in DiabetesFahmi Fauzi SugandiPas encore d'évaluation
- D Evander Schue Ren 2019Document3 pagesD Evander Schue Ren 2019Joseneide Custódio RodriguesPas encore d'évaluation
- CNR 8 247Document7 pagesCNR 8 247Zule FloresPas encore d'évaluation
- Paper 8677Document13 pagesPaper 8677IJARSCT JournalPas encore d'évaluation
- Analysis: Dietary and Nutritional Approaches For Prevention and Management of Type 2 DiabetesDocument9 pagesAnalysis: Dietary and Nutritional Approaches For Prevention and Management of Type 2 DiabetesMr. LPas encore d'évaluation
- 2021 Behavioral and Diet Therapies in Integrated Care For Patients With IBSDocument16 pages2021 Behavioral and Diet Therapies in Integrated Care For Patients With IBSanonPas encore d'évaluation
- Chap172 PDFDocument3 pagesChap172 PDFOlga BragaPas encore d'évaluation
- Dietary Plants, Gut Microbiota, and Obesity. Effects and Mechanisms-DikonversiDocument18 pagesDietary Plants, Gut Microbiota, and Obesity. Effects and Mechanisms-DikonversiIndri Dewi ListianiPas encore d'évaluation
- Obesity - 2022 - Aukan - Gastrointestinal Hormones and Appetite Ratings After Weight Loss Induced by Diet or BariatricDocument14 pagesObesity - 2022 - Aukan - Gastrointestinal Hormones and Appetite Ratings After Weight Loss Induced by Diet or BariatricIsabella María GantivarPas encore d'évaluation
- Long-Term Management of Patients After Weight Loss SurgeryDocument6 pagesLong-Term Management of Patients After Weight Loss SurgeryDina ShawkyPas encore d'évaluation
- Intermittent Fasting Explained – Benefits, Science, and Practical Tips to BeginD'EverandIntermittent Fasting Explained – Benefits, Science, and Practical Tips to BeginPas encore d'évaluation
- Dor LombarDocument27 pagesDor LombarLeonardoCampanelliPas encore d'évaluation
- Screening Cancer GinecológicoDocument18 pagesScreening Cancer GinecológicoLeonardoCampanelliPas encore d'évaluation
- Depressão ScreeningDocument8 pagesDepressão ScreeningLeonardoCampanelliPas encore d'évaluation
- Laceration Repair: A Practical Approach: Randall T. Forsch, MD, MPH Sahoko H. Little, MD, PHD and Christa Williams, MDDocument10 pagesLaceration Repair: A Practical Approach: Randall T. Forsch, MD, MPH Sahoko H. Little, MD, PHD and Christa Williams, MDLeonardoCampanelliPas encore d'évaluation
- Screening Cancer 2019Document4 pagesScreening Cancer 2019LeonardoCampanelliPas encore d'évaluation
- Bloqueadores Do Sraa Não Devem Ser A Primeira EscolhaDocument3 pagesBloqueadores Do Sraa Não Devem Ser A Primeira EscolhaLeonardoCampanelliPas encore d'évaluation
- Dac ScreeningDocument2 pagesDac ScreeningLeonardoCampanelliPas encore d'évaluation
- 2019 Nature Endo Exercício e Conversa Músculo CérebroDocument10 pages2019 Nature Endo Exercício e Conversa Músculo CérebroLeonardoCampanelliPas encore d'évaluation
- Use of "Bioglue" in Aortic Surgical RepairDocument3 pagesUse of "Bioglue" in Aortic Surgical RepairLeonardoCampanelliPas encore d'évaluation
- Primer: AtherosclerosisDocument18 pagesPrimer: AtherosclerosisLeonardoCampanelliPas encore d'évaluation
- Lesões de TornozeloDocument43 pagesLesões de TornozeloLeonardoCampanelliPas encore d'évaluation
- 2016 Gasto de Energia e ObesidadeDocument14 pages2016 Gasto de Energia e ObesidadeLeonardoCampanelliPas encore d'évaluation
- 2010 PHYS REV Microbiota Intestinal Na Saúde e Na DoençaDocument46 pages2010 PHYS REV Microbiota Intestinal Na Saúde e Na DoençaLeonardoCampanelliPas encore d'évaluation
- Mechanisms Underlying Nystagmus: Richard V AbadiDocument4 pagesMechanisms Underlying Nystagmus: Richard V AbadiLeonardoCampanelliPas encore d'évaluation
- Pyle Et Al 1995 - Rapid Direct Count E ColiDocument7 pagesPyle Et Al 1995 - Rapid Direct Count E ColiFabio SenaPas encore d'évaluation
- Ho Lester OlllDocument6 pagesHo Lester OlllVlad VladPas encore d'évaluation
- Inhibidores Naturales de La Acetil ColinesterasaDocument12 pagesInhibidores Naturales de La Acetil Colinesterasafsuarez113Pas encore d'évaluation
- Screenshot 2021-06-23 at 11.36.48 AMDocument116 pagesScreenshot 2021-06-23 at 11.36.48 AMSmitha ShekarPas encore d'évaluation
- DNA Replication Study Guide - Biology101Document4 pagesDNA Replication Study Guide - Biology101nandi_scrPas encore d'évaluation
- AP Psych SyllabusDocument140 pagesAP Psych SyllabusAlex JinPas encore d'évaluation
- Q.Paper Science Class IX (Moderated)Document8 pagesQ.Paper Science Class IX (Moderated)ShivangiPas encore d'évaluation
- Jurnal Reading Pembimbing: Dr. Iwan Sys Indrawanto, SP - KJDocument25 pagesJurnal Reading Pembimbing: Dr. Iwan Sys Indrawanto, SP - KJaribudiperdanaPas encore d'évaluation
- Ento 365 All Objective Qu.Document30 pagesEnto 365 All Objective Qu.Navneet KumarPas encore d'évaluation
- Derma OSCEDocument3 pagesDerma OSCEUsama El BazPas encore d'évaluation
- Discussion Question 1Document3 pagesDiscussion Question 1Brian RelsonPas encore d'évaluation
- (SGD) PathologyDocument6 pages(SGD) PathologyPaulene RiveraPas encore d'évaluation
- Acta Pediatrica Enero 2021 - Topicos NeonatalesDocument113 pagesActa Pediatrica Enero 2021 - Topicos NeonatalesalbertoPas encore d'évaluation
- AIIMS 2015 Solved PaperDocument436 pagesAIIMS 2015 Solved PaperSurya TejaPas encore d'évaluation
- Country Courier - 08/09/2013Document10 pagesCountry Courier - 08/09/2013bladepublishingPas encore d'évaluation
- Alternaria Species Causing Leaf Spot On Hemp (Cannabis Sativa) in Northern ChinaDocument14 pagesAlternaria Species Causing Leaf Spot On Hemp (Cannabis Sativa) in Northern ChinaEsa PaundraPas encore d'évaluation
- Speaking Part 3 Update 2022Document7 pagesSpeaking Part 3 Update 2022Nhi LêPas encore d'évaluation
- SAMPLE Outline PanicDocument3 pagesSAMPLE Outline PanicdexPas encore d'évaluation
- ICU MSC Logbook-FinalDocument101 pagesICU MSC Logbook-FinalCwali MohamedPas encore d'évaluation
- Atrial Fibrillation - Diagnosis and Treatment - AAFP PDFDocument8 pagesAtrial Fibrillation - Diagnosis and Treatment - AAFP PDFNaufal AmanullahPas encore d'évaluation
- Homescience f1-f4Document300 pagesHomescience f1-f4elizabethk1981Pas encore d'évaluation
- Life Expectancy Powerpoint PresentationDocument6 pagesLife Expectancy Powerpoint PresentationAlejandro MendozaPas encore d'évaluation
- GESPv2022 12 02Document61 pagesGESPv2022 12 02Ameraidah PatoraiPas encore d'évaluation