Vous aimerez peut-être aussi
- Complaint For Damages SampleDocument4 pagesComplaint For Damages SampleJubelee Anne Patangan100% (2)
- Anatomy of The Urinary System: Patient's Name / Room No. - 1Document2 pagesAnatomy of The Urinary System: Patient's Name / Room No. - 1myer pasandalanPas encore d'évaluation
- Student Assignment LoadDocument2 pagesStudent Assignment Loadmyer pasandalanPas encore d'évaluation
- Student Assignment LoadDocument2 pagesStudent Assignment Loadmyer pasandalanPas encore d'évaluation
- Summary of Drugs and IVDocument2 pagesSummary of Drugs and IVmyer pasandalanPas encore d'évaluation
- Complaint For Damages SampleDocument4 pagesComplaint For Damages Samplemyer pasandalanPas encore d'évaluation
- Summary of Meds New FormatDocument2 pagesSummary of Meds New Formatmyer pasandalanPas encore d'évaluation
- Nursing Assessment IIDocument5 pagesNursing Assessment IImyer pasandalanPas encore d'évaluation
- Nursing Care Plan: Cues Nursing Diagnosis Objective Intervention Rationale EvaluationDocument3 pagesNursing Care Plan: Cues Nursing Diagnosis Objective Intervention Rationale Evaluationmyer pasandalanPas encore d'évaluation
- Risperidine: Disturbed Thought Process Related To Neurological DisturbancesDocument3 pagesRisperidine: Disturbed Thought Process Related To Neurological Disturbancesmyer pasandalanPas encore d'évaluation
- Nursing Care Plan: Cues Nursing Diagnosis Objective Intervention Rationale EvaluationDocument3 pagesNursing Care Plan: Cues Nursing Diagnosis Objective Intervention Rationale Evaluationmyer pasandalanPas encore d'évaluation
- Review of SystemDocument2 pagesReview of Systemmyer pasandalanPas encore d'évaluation
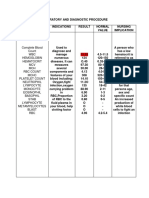
- Laboratory and Diagnostic ProcedureDocument5 pagesLaboratory and Diagnostic Proceduremyer pasandalanPas encore d'évaluation
- Diagnostic and Laboratory ProceduresDocument6 pagesDiagnostic and Laboratory Proceduresmyer pasandalanPas encore d'évaluation
- Nursing Care Plan: Cues Nursing Diagnosis Objective Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Nursing Diagnosis Objective Intervention Rationale Evaluationmyer pasandalanPas encore d'évaluation
- Group F DXDocument2 pagesGroup F DXmyer pasandalanPas encore d'évaluation
- Discharge Plan: Drug/S Indication/S Dosage Route FrequencyDocument3 pagesDischarge Plan: Drug/S Indication/S Dosage Route Frequencymyer pasandalanPas encore d'évaluation
- Case Management 1Document5 pagesCase Management 1myer pasandalanPas encore d'évaluation
- Narrative PathophysiologyDocument5 pagesNarrative Pathophysiologymyer pasandalanPas encore d'évaluation
- Hemorrhagic StrokeDocument4 pagesHemorrhagic Strokemyer pasandalanPas encore d'évaluation
- Drug StudyDocument2 pagesDrug Studymyer pasandalanPas encore d'évaluation
- DKKDNDDocument14 pagesDKKDNDmyer pasandalanPas encore d'évaluation
- ConstipationDocument3 pagesConstipationmyer pasandalanPas encore d'évaluation
- Schizophrenia: I. IdentificationDocument3 pagesSchizophrenia: I. Identificationmyer pasandalanPas encore d'évaluation
- Personality DisordersDocument2 pagesPersonality Disordersmyer pasandalanPas encore d'évaluation
- Anatomy and PhysioDocument2 pagesAnatomy and Physiomyer pasandalanPas encore d'évaluation
- Drug StudyDocument2 pagesDrug Studymyer pasandalanPas encore d'évaluation
- Somatoform Disorders: I. IdentificationDocument1 pageSomatoform Disorders: I. Identificationmyer pasandalanPas encore d'évaluation
- Eating DisordersDocument1 pageEating Disordersmyer pasandalanPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- KEMH Guidelines On Cardiac Disease in PregnancyDocument7 pagesKEMH Guidelines On Cardiac Disease in PregnancyAyesha RazaPas encore d'évaluation
- Target Heart Rate Lesson PlanDocument4 pagesTarget Heart Rate Lesson PlanEryn YeskePas encore d'évaluation
- Lecture in Geriatrics Physical Therapy 1Document27 pagesLecture in Geriatrics Physical Therapy 1S.APas encore d'évaluation
- Physiological Changes Postpartum PeriodDocument2 pagesPhysiological Changes Postpartum PeriodEurielle MiolePas encore d'évaluation
- Profile of Osteopathic Practice in Spain Results FDocument11 pagesProfile of Osteopathic Practice in Spain Results FBerenice LimarkPas encore d'évaluation
- ESI ER CompleteDocument45 pagesESI ER Completetammy2121Pas encore d'évaluation
- 2016 10 12 Members Letter-HHS OCR Organ Transplant DiscriminationDocument4 pages2016 10 12 Members Letter-HHS OCR Organ Transplant DiscriminationMike Honda100% (2)
- Feeds and Feedings - Margie EranDocument29 pagesFeeds and Feedings - Margie EranAlliah Dela RosaPas encore d'évaluation
- The Diagram Shows How A Company Called HB Office RDocument1 pageThe Diagram Shows How A Company Called HB Office RbugakPas encore d'évaluation
- Fasting and Low Carb InfoDocument4 pagesFasting and Low Carb InfoKatrin NovaPas encore d'évaluation
- Pres 2 PastpapersDocument190 pagesPres 2 PastpapersOdettePas encore d'évaluation
- Regional Victoria's RoadmapDocument12 pagesRegional Victoria's RoadmapTara CosoletoPas encore d'évaluation
- Coma ManagementDocument5 pagesComa ManagementElena DocPas encore d'évaluation
- Improving Lives of South Sudanese Communities Through Water and Sanitation: The Story of Salva DutDocument1 pageImproving Lives of South Sudanese Communities Through Water and Sanitation: The Story of Salva DutUNICEF South SudanPas encore d'évaluation
- Tcharestresumefinal 1009Document2 pagesTcharestresumefinal 1009tcharestPas encore d'évaluation
- Part 4abcDocument11 pagesPart 4abcMatthew Guevarra100% (1)
- Effects of Sprint Interval Training and Body.24Document8 pagesEffects of Sprint Interval Training and Body.24Maxwell MartinsPas encore d'évaluation
- Topic ListDocument6 pagesTopic ListEdwinPas encore d'évaluation
- Asthma Case StudyDocument39 pagesAsthma Case StudyDimitris TasiouPas encore d'évaluation
- Shaikh Sohail Shaikh KaleemDocument1 pageShaikh Sohail Shaikh KaleemMantra SriPas encore d'évaluation
- Safety Pocket Guide Web 061808Document534 pagesSafety Pocket Guide Web 061808hombre911100% (1)
- (Yabanci Dil Testi) : T.C. Millî Eğitim Bakanliği Ölçme, Değerlendirme Ve Sinav Hizmetleri Genel MüdürlüğüDocument22 pages(Yabanci Dil Testi) : T.C. Millî Eğitim Bakanliği Ölçme, Değerlendirme Ve Sinav Hizmetleri Genel Müdürlüğücem kayaPas encore d'évaluation
- Is Smartphone Addiction Really An AddictionDocument17 pagesIs Smartphone Addiction Really An AddictionHani HanoyyPas encore d'évaluation
- Antiinflammatorydrugs: Beatriz Monteiro,, Paulo V. SteagallDocument19 pagesAntiinflammatorydrugs: Beatriz Monteiro,, Paulo V. SteagallYohan Oropeza VergaraPas encore d'évaluation
- Test Bank For Pharmacology A Patient Centered Nursing Process Approach 9th EditionDocument16 pagesTest Bank For Pharmacology A Patient Centered Nursing Process Approach 9th EditionMichael Pupo73% (15)
- DebateDocument12 pagesDebate•Kai yiii•Pas encore d'évaluation
- DR Daniel Samadi MD PC - Pediatric ENT NJDocument7 pagesDR Daniel Samadi MD PC - Pediatric ENT NJPediatric ENT NJ by Dr Daniel SamadiPas encore d'évaluation
- Hazard Analysis in The WorkplaceDocument7 pagesHazard Analysis in The WorkplaceUghlahnPas encore d'évaluation
- The Impact of Longitudinal Studies On Understanding Development From Young Adulthood To Old AgeDocument11 pagesThe Impact of Longitudinal Studies On Understanding Development From Young Adulthood To Old AgeLana PeharPas encore d'évaluation
- Research Chapter 1 V Final Autosaved 2 1Document57 pagesResearch Chapter 1 V Final Autosaved 2 1Mirate JessPas encore d'évaluation