Vous aimerez peut-être aussi
- B. Pathophysiology: Clinical Aspects of Cancer DiagnosisDocument10 pagesB. Pathophysiology: Clinical Aspects of Cancer DiagnosisAbigael Patricia GutierrezPas encore d'évaluation
- WEEK 4 - MEDSURG - Cellular AberrationDocument10 pagesWEEK 4 - MEDSURG - Cellular AberrationLeslie CruzPas encore d'évaluation
- Disaster Preparedness - Leadership and Coordination in Disaster in Health Care System With LectureDocument29 pagesDisaster Preparedness - Leadership and Coordination in Disaster in Health Care System With LectureArvie ReyesPas encore d'évaluation
- Cellular AberrationDocument71 pagesCellular AberrationKris TejereroPas encore d'évaluation
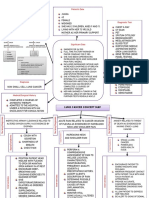
- Breast Cancer Concept MapDocument1 pageBreast Cancer Concept MapKeepItSecret100% (1)
- Types of ShocksDocument33 pagesTypes of Shocksmark OrpillaPas encore d'évaluation
- Transcultural Perspective in The Nursing Care of Adults Physiologic Development During AdulthoodDocument5 pagesTranscultural Perspective in The Nursing Care of Adults Physiologic Development During AdulthoodeuLa-mayzellPas encore d'évaluation
- NCM 112 Lecture Module 4 Cellular AberrationDocument16 pagesNCM 112 Lecture Module 4 Cellular AberrationMeryville JacildoPas encore d'évaluation
- Cellular AberrationDocument14 pagesCellular AberrationjinahyangPas encore d'évaluation
- NCP Cancer of StomachDocument2 pagesNCP Cancer of StomachBien Sawali100% (1)
- Soapie, Assessment and NCP On PAINDocument7 pagesSoapie, Assessment and NCP On PAINAna100% (2)
- Cardiovascular HealthDocument20 pagesCardiovascular HealthChrriePas encore d'évaluation
- Community Diagnosis (2) RLEDocument25 pagesCommunity Diagnosis (2) RLEAnon NimosPas encore d'évaluation
- CHNDocument49 pagesCHNAlbert Remollo Jr100% (2)
- NCM 116 Lecture ENDOCRINE Pituitary Gland Thyroid Gland DisordersDocument4 pagesNCM 116 Lecture ENDOCRINE Pituitary Gland Thyroid Gland DisordersMeryville JacildoPas encore d'évaluation
- MEDSURG MERGED (Cellular Abber + Cancer Manage)Document34 pagesMEDSURG MERGED (Cellular Abber + Cancer Manage)Leslie CruzPas encore d'évaluation
- PUCAN, Julienne BSN III-D - SGD - HYPO&HYPERCHLOREMIADocument10 pagesPUCAN, Julienne BSN III-D - SGD - HYPO&HYPERCHLOREMIAJulienne PucanPas encore d'évaluation
- NCM 107 NCM 109 Case Study FormatDocument7 pagesNCM 107 NCM 109 Case Study FormatCharme Jean RaygonPas encore d'évaluation
- Unit 1: Introduction To Community Health Nursing Chapter 1: Fundamental Concepts of Community Health NursingDocument134 pagesUnit 1: Introduction To Community Health Nursing Chapter 1: Fundamental Concepts of Community Health NursingMille Kaia100% (2)
- Nursing Care Plan For Inguinal HerniaDocument1 pageNursing Care Plan For Inguinal HerniaYvonne Joyce Gayagoy GomezPas encore d'évaluation
- Nursing Care Plan For Myasthenia Gravis Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan For Myasthenia Gravis Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle AcenaPas encore d'évaluation
- KetorolacDocument5 pagesKetorolacMichelle Ann P. NacuaPas encore d'évaluation
- NCM 116 W1 Reading HandoutDocument13 pagesNCM 116 W1 Reading Handoutriza sarmientoPas encore d'évaluation
- Virtual Hospital Practice Case Analysis-Ob Ward 2 SEM. SY: 2019-2020Document2 pagesVirtual Hospital Practice Case Analysis-Ob Ward 2 SEM. SY: 2019-2020Soleil MaxwellPas encore d'évaluation
- NCM 106 Cellular AberrasionDocument11 pagesNCM 106 Cellular AberrasionArika Vista-Mamigo100% (3)
- Chron's Disease 2Document3 pagesChron's Disease 2TarantadoPas encore d'évaluation
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationTimothy Joseph F. RosalesPas encore d'évaluation
- Psychosocial Care of Older Adults: Cognition and Perception: Ma. Concepcion A. Maico, RN, MAN, Ed.DDocument35 pagesPsychosocial Care of Older Adults: Cognition and Perception: Ma. Concepcion A. Maico, RN, MAN, Ed.DMEJIE MARL RAVEN INSTRELLAPas encore d'évaluation
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument1 pageAssessment Diagnosis Planning Intervention Rationale EvaluationFranz RolfPas encore d'évaluation
- September 13 - NCM 112 (Mam G)Document2 pagesSeptember 13 - NCM 112 (Mam G)Aaron DayloPas encore d'évaluation
- Chapter 1 (Historical Perspective of Nursing Informatics)Document49 pagesChapter 1 (Historical Perspective of Nursing Informatics)Janelle Cabida SupnadPas encore d'évaluation
- Causative Agents Causative Agents: Headache, Myalgia, & Nausea Are Added S/SX For Streptococcal PharyngitisDocument21 pagesCausative Agents Causative Agents: Headache, Myalgia, & Nausea Are Added S/SX For Streptococcal PharyngitisDon Chiaw Manongdo100% (1)
- JRMMC - Patho of Ruptured AppendicitisDocument3 pagesJRMMC - Patho of Ruptured Appendicitis9632141475963Pas encore d'évaluation
- Lung Cancer Concept Map-Group 2Document2 pagesLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- MEDSURG - Cellular AberrationDocument10 pagesMEDSURG - Cellular AberrationLeslie CruzPas encore d'évaluation
- NCM 112 E LEARNING AutosavedDocument7 pagesNCM 112 E LEARNING AutosavedMikko McDonie VeloriaPas encore d'évaluation
- Cause of Death Rate/ 10,000 Pop (TB) 2. Swaroop's IndexDocument2 pagesCause of Death Rate/ 10,000 Pop (TB) 2. Swaroop's IndexLeslie CruzPas encore d'évaluation
- Oxygen Administration ProcedureDocument4 pagesOxygen Administration ProcedureJay Harold Cordero PanlilioPas encore d'évaluation
- NCP StrokeDocument2 pagesNCP StrokeEtienne NinxPas encore d'évaluation
- Drug StudiesDocument16 pagesDrug Studiesvitcloud23100% (2)
- Hepatobiliary SystemDocument35 pagesHepatobiliary Systemyoyo patoPas encore d'évaluation
- 5 Nursing Management TBDocument2 pages5 Nursing Management TBًPas encore d'évaluation
- Cellular AberrationDocument6 pagesCellular AberrationCheysser FerolinoPas encore d'évaluation
- Health Care Delivery System & COPARDocument52 pagesHealth Care Delivery System & COPARDharylle Cariño100% (1)
- Amoebiasis PathophysiologyDocument3 pagesAmoebiasis PathophysiologyApril CornejoPas encore d'évaluation
- Topic 3 NCM 112Document4 pagesTopic 3 NCM 112Marielle ChuaPas encore d'évaluation
- DP HyperthyroidismDocument6 pagesDP HyperthyroidismTracy May CandolitaPas encore d'évaluation
- Leadership Roles and Responsibilities of A Nurse in Disaster Risk and Reduction ManagementDocument13 pagesLeadership Roles and Responsibilities of A Nurse in Disaster Risk and Reduction ManagementIrish Jane GalloPas encore d'évaluation
- FNCP DiagnosisDocument5 pagesFNCP Diagnosisjaja0% (1)
- Concept Map (Aplastic Anemia) b1Document6 pagesConcept Map (Aplastic Anemia) b1Ran PioloPas encore d'évaluation
- Medical-Surgical Nursing 1: Pamantasan NG Lungsod NG MaynilaDocument3 pagesMedical-Surgical Nursing 1: Pamantasan NG Lungsod NG MaynilaAye DumpPas encore d'évaluation
- OB Gyne Ward PretestDocument3 pagesOB Gyne Ward PretestCHRISTIAN RAY ALPAS PASILIAOPas encore d'évaluation
- Name of Drug Dosage and Route Indications Contra-Indications Side Effects Nursing ResponsibilitiesDocument7 pagesName of Drug Dosage and Route Indications Contra-Indications Side Effects Nursing ResponsibilitiesTon AgustinPas encore d'évaluation
- Kidney CancerDocument31 pagesKidney CancerEfren Elico VenguaPas encore d'évaluation
- Case Study2Document11 pagesCase Study2Jainet Aira S. AmantePas encore d'évaluation
- Appendicitis (History & Examination)Document6 pagesAppendicitis (History & Examination)Doctor Saleem Rehman75% (4)
- NCM 106 Cellular-AberrationDocument6 pagesNCM 106 Cellular-AberrationJoanne TolopiaPas encore d'évaluation
- 1 - Intro OpathDocument5 pages1 - Intro Opathcath.rada17Pas encore d'évaluation
- NEOPLASIA ExpDocument17 pagesNEOPLASIA ExpYuris AriasPas encore d'évaluation
- Bla Bla Bla New 2014Document11 pagesBla Bla Bla New 2014Georgiana GeoPas encore d'évaluation
- INTEGUMENTARY SYsTEMDocument42 pagesINTEGUMENTARY SYsTEMGabPas encore d'évaluation
- Hiv Associated Hematological Malignasis - Marcus HentrichDocument239 pagesHiv Associated Hematological Malignasis - Marcus HentrichJaronjer1Pas encore d'évaluation
- Characteristics of Life UpdatedDocument12 pagesCharacteristics of Life UpdatedYla Mae Buo AcejoPas encore d'évaluation
- CHAPTER 16 MicroparaDocument46 pagesCHAPTER 16 MicroparaKathlyn LopeñaPas encore d'évaluation
- DLP - Tomatom. Science 10. q3 - DNA REPLICAtionDocument10 pagesDLP - Tomatom. Science 10. q3 - DNA REPLICAtionalchristian tomatomPas encore d'évaluation
- Orange Blue Shop Creative Trifold BrochureDocument1 pageOrange Blue Shop Creative Trifold BrochureBeverly PantohanPas encore d'évaluation
- Student Exploration: Building DNADocument4 pagesStudent Exploration: Building DNAShiper 33Pas encore d'évaluation
- Chapter 10 Kingdom Animalia MCQs PDF Class 11Document11 pagesChapter 10 Kingdom Animalia MCQs PDF Class 11Rahi HabibPas encore d'évaluation
- Upcoming Diagnostic and Therapeutic Developments in Classical Hodgkin's LymphomaDocument8 pagesUpcoming Diagnostic and Therapeutic Developments in Classical Hodgkin's LymphomaNidhi JaisPas encore d'évaluation
- The Digestive System MODULEDocument3 pagesThe Digestive System MODULEBen Moldenhaur100% (2)
- Muscle and Nervous Tissues LabDocument4 pagesMuscle and Nervous Tissues LabSip BioPas encore d'évaluation
- Disinfectants: Exercise 4Document11 pagesDisinfectants: Exercise 4Jake GerolagaPas encore d'évaluation
- Siyavula Life Sciences Grade 10 3.1Document317 pagesSiyavula Life Sciences Grade 10 3.1Khodani Given MukhumuliPas encore d'évaluation
- Tuesday, August 18, 2009Document47 pagesTuesday, August 18, 2009zorbaxPas encore d'évaluation
- Module 6 Science 10Document20 pagesModule 6 Science 10bhrayancacheroPas encore d'évaluation
- What Is GM CornDocument2 pagesWhat Is GM CornjamilcuzzPas encore d'évaluation
- The Importance of Health Fitness and WellnessDocument3 pagesThe Importance of Health Fitness and Wellnessapi-25954769Pas encore d'évaluation
- Cmi CMBDocument7 pagesCmi CMBMary M. ToribioPas encore d'évaluation
- 2011 Fractal DNADocument7 pages2011 Fractal DNAAbby SweeneyPas encore d'évaluation
- Nucleic AcidsDocument12 pagesNucleic AcidsAntonette SolaresPas encore d'évaluation
- Teaching Biology and Science in The FieldDocument10 pagesTeaching Biology and Science in The FieldIvan IvanovicPas encore d'évaluation
- Luminescent ATP Detection Assay Kit Ab113849 Luminescent ATP Detection Assay Kit Ab113849Document4 pagesLuminescent ATP Detection Assay Kit Ab113849 Luminescent ATP Detection Assay Kit Ab113849carlosPas encore d'évaluation
- Chapter 1.3 Structures and Functions of OrganellesDocument35 pagesChapter 1.3 Structures and Functions of OrganellesFairview PenangPas encore d'évaluation
- CV Aeman 2018 NewDocument4 pagesCV Aeman 2018 NewAeman KhalidPas encore d'évaluation
- Sbi4u1-Cell Bio-Cell Transport 4Document15 pagesSbi4u1-Cell Bio-Cell Transport 4alathena alathenaPas encore d'évaluation
- A2 Edexcel Biology Session 4 1 PhotosyntDocument22 pagesA2 Edexcel Biology Session 4 1 PhotosyntRick WuPas encore d'évaluation
- Physioex 1.1Document5 pagesPhysioex 1.1Tj MordeckiPas encore d'évaluation
- Humrep 1Document2 pagesHumrep 1Danakey CentenoPas encore d'évaluation
- S.Y. B.SC - III (Old) & Ivexam Oct - Nov - 2016Document5 pagesS.Y. B.SC - III (Old) & Ivexam Oct - Nov - 2016Amol DesalePas encore d'évaluation