Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Craap Test WorksheetDocument5 pagesCraap Test Worksheetapi-272946391Pas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Take Off - Workbook PDFDocument108 pagesTake Off - Workbook PDFSam Love0% (1)
- Esl Lesson Plan For Ed EndingDocument6 pagesEsl Lesson Plan For Ed EndingMiriam Garcia RodriguezPas encore d'évaluation
- PRACTICAL RESEARCH PAPER 1111111 IiidoloDocument32 pagesPRACTICAL RESEARCH PAPER 1111111 Iiidoloskylark fannyPas encore d'évaluation
- Kota Krishna Chaitanya - ResumeDocument4 pagesKota Krishna Chaitanya - Resumexiaomi giaPas encore d'évaluation
- 2011 EngDocument15 pages2011 Eng비바525Pas encore d'évaluation
- Attendee Roster 1-23-14Document16 pagesAttendee Roster 1-23-14Kavitha IPas encore d'évaluation
- Ibm SW scm-2.20.0 Anyos I386Document52 pagesIbm SW scm-2.20.0 Anyos I386Denada Deni Deni SulkajPas encore d'évaluation
- Unit+5 5-5 6+Quiz+ReviewDocument6 pagesUnit+5 5-5 6+Quiz+ReviewTyler LongPas encore d'évaluation
- Buss40003 - Risk and Reward - Module DescriptorDocument2 pagesBuss40003 - Risk and Reward - Module DescriptorVishwa NirmalaPas encore d'évaluation
- Prof. Ed. 3 M1L1Document7 pagesProf. Ed. 3 M1L1Jason San PidroPas encore d'évaluation
- Training For Success: A Policy To Expand Apprenticeships in The United StatesDocument66 pagesTraining For Success: A Policy To Expand Apprenticeships in The United StatesCenter for American ProgressPas encore d'évaluation
- LESSON PLAN in COT1 - Q1 (2023-2024)Document4 pagesLESSON PLAN in COT1 - Q1 (2023-2024)MAY RACHEL NARRAGAPas encore d'évaluation
- Tracking Your Trades: ExampleDocument3 pagesTracking Your Trades: Examplequentin oliverPas encore d'évaluation
- Software Development Plan TemplateDocument5 pagesSoftware Development Plan TemplateArvada Solutions0% (1)
- Feminist Theoretical Frameworks: Gender StudiesDocument2 pagesFeminist Theoretical Frameworks: Gender StudiesMcdared GeneralaoPas encore d'évaluation
- Taru INTERNDocument32 pagesTaru INTERNMdrehan AhmedPas encore d'évaluation
- NCAC Letter: Curious Incident in TallahasseeDocument3 pagesNCAC Letter: Curious Incident in TallahasseencacensorshipPas encore d'évaluation
- Minutes of Meeting Class Schedule Parents Orientation LAC Plan and School Recovery Learning PLan August 17 2022Document5 pagesMinutes of Meeting Class Schedule Parents Orientation LAC Plan and School Recovery Learning PLan August 17 2022Janette BolantePas encore d'évaluation
- Olugbenga's CV EngineerDocument2 pagesOlugbenga's CV EngineerSanni Tajudeen OlugbengaPas encore d'évaluation
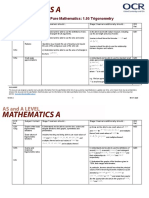
- Teacher Delivery Guide Pure Mathematics: 1.05 TrigonometryDocument16 pagesTeacher Delivery Guide Pure Mathematics: 1.05 TrigonometryHubert SelormeyPas encore d'évaluation
- Hi, Vladimir! Type: Turbulent Defender Code: Isfj-T Role: Sentinel Strategy: Constant ImprovementDocument14 pagesHi, Vladimir! Type: Turbulent Defender Code: Isfj-T Role: Sentinel Strategy: Constant ImprovementVladimir KostovskiPas encore d'évaluation
- Case 4Document3 pagesCase 4Pavan HegdePas encore d'évaluation
- Lesson Plan Modal Verbs 8Document9 pagesLesson Plan Modal Verbs 8Mary Craciun VasuicaPas encore d'évaluation
- Inverse Cube LawDocument2 pagesInverse Cube LawmissuedPas encore d'évaluation
- Cadaver Reaction PaperDocument1 pageCadaver Reaction PaperAelBartolome100% (1)
- English ProjectDocument15 pagesEnglish Projectpranit.saluja.ps.2324Pas encore d'évaluation
- Action Plan: Training of School Personnel On Psychological First AidDocument2 pagesAction Plan: Training of School Personnel On Psychological First AidJT SaguinPas encore d'évaluation
- Folleto Tríptico GA1-240202501-AA2-EV01Document2 pagesFolleto Tríptico GA1-240202501-AA2-EV01STELLA0% (1)
- Files/keplers - Laws - Es - PDF: Kepler Activity SourceDocument5 pagesFiles/keplers - Laws - Es - PDF: Kepler Activity SourceREGINA SANTIAGOPas encore d'évaluation