Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Nur 410 Final PaperDocument7 pagesNur 410 Final Paperapi-377091267Pas encore d'évaluation
- Community Final PaperDocument7 pagesCommunity Final Paperapi-377091267Pas encore d'évaluation
- Leadership Final PaperDocument6 pagesLeadership Final Paperapi-377091267Pas encore d'évaluation
- Plan of CareDocument6 pagesPlan of Careapi-377091267Pas encore d'évaluation
- Health Impact Framework Research PaperDocument11 pagesHealth Impact Framework Research Paperapi-377091267Pas encore d'évaluation
- Lindsays Nursing PhilosophyDocument7 pagesLindsays Nursing Philosophyapi-377091267Pas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Chap 1&3Document51 pagesChap 1&3Lady DaniellePas encore d'évaluation
- Clinical ResearchDocument15 pagesClinical ResearchafshanPas encore d'évaluation
- 30 - Contracted Pelvis and Cephalopelvic DisproportionDocument28 pages30 - Contracted Pelvis and Cephalopelvic Disproportiondr_asaleh93% (14)
- FDA Pre-Marketing Risk Assessment 04d-0187-gdl0002 PDFDocument28 pagesFDA Pre-Marketing Risk Assessment 04d-0187-gdl0002 PDFMorcosPas encore d'évaluation
- Benefits of Effective Lifting ProgramDocument30 pagesBenefits of Effective Lifting ProgramMoradeke OnasanyaPas encore d'évaluation
- CircumcisionDocument7 pagesCircumcisionChioma OkoPas encore d'évaluation
- Paronychia InfectionDocument6 pagesParonychia InfectionAngie Cabanting BañezPas encore d'évaluation
- ACRC 40k Surrogacy Program Fees Overview. (2305)Document4 pagesACRC 40k Surrogacy Program Fees Overview. (2305)jiawhu2008Pas encore d'évaluation
- Elder AbuseDocument10 pagesElder AbusemiguelalmenarezPas encore d'évaluation
- Fitness & Wellness Industry in IndiaDocument12 pagesFitness & Wellness Industry in IndiaPrince SinghPas encore d'évaluation
- Implant ArticleDocument20 pagesImplant ArticleArun PrasadPas encore d'évaluation
- Needle Stick InjuriesDocument1 pageNeedle Stick InjuriesAgnes BPas encore d'évaluation
- Can "Daniel's Diabetic Miracle" Naturally Heal Diabetes in As Little As 3 DaysDocument33 pagesCan "Daniel's Diabetic Miracle" Naturally Heal Diabetes in As Little As 3 Daysaz75% (4)
- Do Not Resuscitate Orders: Among Physicians, Nurses, Patients and RelativesDocument4 pagesDo Not Resuscitate Orders: Among Physicians, Nurses, Patients and RelativesSalman HabeebPas encore d'évaluation
- Introductory Report On GlenmarkDocument33 pagesIntroductory Report On GlenmarkSai Gautham50% (2)
- Group B-2 Operation Management ProjectDocument17 pagesGroup B-2 Operation Management Projectanksri07Pas encore d'évaluation
- FilariasisDocument23 pagesFilariasisPrincess Gutierrez RositaPas encore d'évaluation
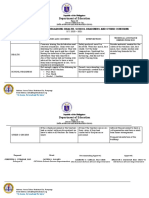
- Grade 5 - ISSUES-AND-CONCERNS-FOR-HEALTH-SCHOOL-READINESS-OTHER-CONCERNSDocument2 pagesGrade 5 - ISSUES-AND-CONCERNS-FOR-HEALTH-SCHOOL-READINESS-OTHER-CONCERNSDanny LinePas encore d'évaluation
- Communicable Disease SurveillanceDocument60 pagesCommunicable Disease SurveillanceAmeer MuhammadPas encore d'évaluation
- Polio A Shot in The DarkDocument11 pagesPolio A Shot in The DarkJohnathanSteinPas encore d'évaluation
- Running Head: Evidence-Based Practice: Pressure Ulcer RiskDocument5 pagesRunning Head: Evidence-Based Practice: Pressure Ulcer RiskElise HowardPas encore d'évaluation
- Reten Modern Dressing 2023 PKDMTDocument51 pagesReten Modern Dressing 2023 PKDMTMasros TukiranPas encore d'évaluation
- Somatization DisorderDocument3 pagesSomatization DisorderVincePas encore d'évaluation
- ARDSDocument26 pagesARDSDuratul FahliaPas encore d'évaluation
- Philippine Institute of Traditional and Alternative Health Care (PITAHC) Board of Trustees Government RepresentativesDocument3 pagesPhilippine Institute of Traditional and Alternative Health Care (PITAHC) Board of Trustees Government Representativesallen reyesPas encore d'évaluation
- Fhap Family Summary: Group MembersDocument5 pagesFhap Family Summary: Group MembersJacob JrPas encore d'évaluation
- Fasciolopsis BuskiDocument18 pagesFasciolopsis BuskiAmritesh KumarPas encore d'évaluation
- Nursing Education: Rating ScaleDocument5 pagesNursing Education: Rating Scalemerin sunil100% (2)
- Treatment Center PDFDocument120 pagesTreatment Center PDFShellyPas encore d'évaluation