Vous aimerez peut-être aussi
- CE (Vi) F (SK) PF1 (PS OM) PFA (SS) PN (SS) PDFDocument5 pagesCE (Vi) F (SK) PF1 (PS OM) PFA (SS) PN (SS) PDFrizqina ajraPas encore d'évaluation
- PIIS2210778916303701Document2 pagesPIIS2210778916303701Fatimah AssagafPas encore d'évaluation
- Jurnal Abrupsio PlasentaDocument13 pagesJurnal Abrupsio Plasentaperussi pranadiptaPas encore d'évaluation
- AbruptionDocument13 pagesAbruptionMauricio Lopez MejiaPas encore d'évaluation
- Pregnancy-Induced Hypertension Is An Independent Risk Factor For Meconium Aspiration Syndrome A Retrospective Population Based Cohort StudyDocument5 pagesPregnancy-Induced Hypertension Is An Independent Risk Factor For Meconium Aspiration Syndrome A Retrospective Population Based Cohort StudyRIECHELLE SEVILLAPas encore d'évaluation
- AbruptionDocument13 pagesAbruptionAnghelo Aldair Velásquez CarrilloPas encore d'évaluation
- Fonc 11 803994Document13 pagesFonc 11 803994zahra abdurrazakPas encore d'évaluation
- Kobayashi 2014Document7 pagesKobayashi 2014Mauricio Lopez MejiaPas encore d'évaluation
- An Uncommon Cause of Antepartum Haemorrhage: A Case Study: January 2019Document7 pagesAn Uncommon Cause of Antepartum Haemorrhage: A Case Study: January 2019SriMathi Kasi Malini ArmugamPas encore d'évaluation
- Jurnal Internasional 1Document5 pagesJurnal Internasional 1Ifni AngraeniPas encore d'évaluation
- Comparing the severity of second preeclampsia with first preeclampsia_ a multicenter retrospective longitudinal cohort studyDocument7 pagesComparing the severity of second preeclampsia with first preeclampsia_ a multicenter retrospective longitudinal cohort studyCARLOS MACHADOPas encore d'évaluation
- Risk Factors for Severe PPH After C-Section for Placenta PraeviaDocument7 pagesRisk Factors for Severe PPH After C-Section for Placenta PraeviaCorina PavalachePas encore d'évaluation
- 1 s2.0 S1028455919300178 Main PDFDocument5 pages1 s2.0 S1028455919300178 Main PDFRadinal PrayitnoPas encore d'évaluation
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument7 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySuis MionooPas encore d'évaluation
- Jsafog 13 137Document5 pagesJsafog 13 137Elizabeth Duprat GaxiolaPas encore d'évaluation
- Herrera 2017Document9 pagesHerrera 2017Bianca Maria PricopPas encore d'évaluation
- Threatened Abortion A Risk Factor For Poor PregnanDocument8 pagesThreatened Abortion A Risk Factor For Poor PregnanBaiiqDelaYulianingtyasPas encore d'évaluation
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsD'EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsPas encore d'évaluation
- E058068 FullDocument7 pagesE058068 FullJordan HutabaratPas encore d'évaluation
- Associated Risk Factors of Placenta Previa A Matched Case Control StudyDocument4 pagesAssociated Risk Factors of Placenta Previa A Matched Case Control StudyFitri Nur DiniPas encore d'évaluation
- Original ArticleDocument4 pagesOriginal ArticlefeyzarezarPas encore d'évaluation
- Aust NZ J Obst Gynaeco - 2022 - Silveira - Placenta Accreta Spectrum We Can Do BetterDocument7 pagesAust NZ J Obst Gynaeco - 2022 - Silveira - Placenta Accreta Spectrum We Can Do BetterDrFeelgood WolfslandPas encore d'évaluation
- Solutio Plasenta JournalDocument7 pagesSolutio Plasenta JournalAndi NatalonnaPas encore d'évaluation
- DMV 054Document12 pagesDMV 054priyaPas encore d'évaluation
- Anemia-1Document15 pagesAnemia-1Intan Wahyu CahyaniPas encore d'évaluation
- Tubalpregnancy DiagnosisandmanagementDocument12 pagesTubalpregnancy DiagnosisandmanagementAndreaAlexandraPas encore d'évaluation
- Modern Management of Recurrent Miscarriage: Hayden Anthony HomerDocument9 pagesModern Management of Recurrent Miscarriage: Hayden Anthony Homersutomo sutomoPas encore d'évaluation
- The Risk of Adverse Pregnancy Outcomes Following.11Document7 pagesThe Risk of Adverse Pregnancy Outcomes Following.11Mara MendozaPas encore d'évaluation
- Jurding 1Document8 pagesJurding 1Danis SharitaPas encore d'évaluation
- Supportive Management of Pregnancy-Associated Aplastic AnemiaDocument6 pagesSupportive Management of Pregnancy-Associated Aplastic AnemiaAs YuYu MustafaPas encore d'évaluation
- Abruptio Placenta and Its Maternal and Fetal Outcome: Ritu MishraDocument4 pagesAbruptio Placenta and Its Maternal and Fetal Outcome: Ritu MishraBella Dama ShintaPas encore d'évaluation
- Pregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninDocument5 pagesPregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninMentari SetiawatiPas encore d'évaluation
- 9 PDFDocument9 pages9 PDFAnggun SetiawatiPas encore d'évaluation
- vanderpol2016Document6 pagesvanderpol2016Andy esPas encore d'évaluation
- Antepartum Haemorrhage: Causes & Its Effects On Mother and Child: An EvaluationDocument5 pagesAntepartum Haemorrhage: Causes & Its Effects On Mother and Child: An EvaluationubayyumrPas encore d'évaluation
- Acta Obstet Gynecol Scand - 2011 - STJERNHOLM - Changed Indications For Cesarean SectionsDocument5 pagesActa Obstet Gynecol Scand - 2011 - STJERNHOLM - Changed Indications For Cesarean SectionsAli QuwarahPas encore d'évaluation
- Baru MDocument3 pagesBaru MRezky Wulandari RoniPas encore d'évaluation
- Aggressive Intervention of Previable Preterm Premature Rupture of MembranesDocument8 pagesAggressive Intervention of Previable Preterm Premature Rupture of MembranesVanessa Riaño GodoyPas encore d'évaluation
- Mother and Child: An Evaluation: Antepartum Haemorrhage: Causes & Its Effects OnDocument5 pagesMother and Child: An Evaluation: Antepartum Haemorrhage: Causes & Its Effects OnTya AgustinPas encore d'évaluation
- Arabin Pessary to Prevent Adverse Perinatal Outcomes in Twin Pregnancies With a Short Cervix, PESSARONE. Marion GroussollesDocument13 pagesArabin Pessary to Prevent Adverse Perinatal Outcomes in Twin Pregnancies With a Short Cervix, PESSARONE. Marion GroussollesqmfddnhdjmPas encore d'évaluation
- Acute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisDocument6 pagesAcute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisIntan Wahyu CahyaniPas encore d'évaluation
- The Prevalence of Thrombocytopenia and The Associated Factors Among Pregnant Women in Hoima Regional Referral Hospital, Western Uganda.Document11 pagesThe Prevalence of Thrombocytopenia and The Associated Factors Among Pregnant Women in Hoima Regional Referral Hospital, Western Uganda.KIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- Journal Atonia Uteri YuyunDocument6 pagesJournal Atonia Uteri YuyunMoh RamliPas encore d'évaluation
- 2020 - Maternal Inherited Thrombophilia and Pregnancy OutcomesDocument4 pages2020 - Maternal Inherited Thrombophilia and Pregnancy OutcomesIrina SerpiPas encore d'évaluation
- Jurnal Intern 2Document7 pagesJurnal Intern 2Annisaa AndrianaPas encore d'évaluation
- Objectives:: CorrespondenceDocument5 pagesObjectives:: Correspondenceraudatul jannahPas encore d'évaluation
- Ojog 2018080316254387 PDFDocument13 pagesOjog 2018080316254387 PDFyundrimartirazPas encore d'évaluation
- A Case Control Study of Risk Factors and Neonatal Outcomes of Preterm BirthDocument5 pagesA Case Control Study of Risk Factors and Neonatal Outcomes of Preterm BirthSarahí SosaPas encore d'évaluation
- Jurnal Reading ObygnDocument6 pagesJurnal Reading ObygnLimastani FebrianaPas encore d'évaluation
- MiscarriageDocument8 pagesMiscarriagejaimejosePas encore d'évaluation
- Breast Cancer in Young WomenD'EverandBreast Cancer in Young WomenOreste GentiliniPas encore d'évaluation
- Jurnal Obgyn AstiDocument5 pagesJurnal Obgyn AstiadelialuthfiPas encore d'évaluation
- Bakker 2012Document10 pagesBakker 2012ieoPas encore d'évaluation
- International Journal of Surgery: Humphrey G.M. Walker, Ahmad Al Samaraee, Sarah J. Mills, M. Reza KalbassiDocument7 pagesInternational Journal of Surgery: Humphrey G.M. Walker, Ahmad Al Samaraee, Sarah J. Mills, M. Reza KalbassiJason CalvinPas encore d'évaluation
- Original Article The Association of Bacterial Vaginosis and Preterm LaborDocument3 pagesOriginal Article The Association of Bacterial Vaginosis and Preterm LaborHarry ManuhutuPas encore d'évaluation
- Prolonged Latency of Preterm Premature Rupture of Membranes and Risk of Neonatal SepsisDocument6 pagesProlonged Latency of Preterm Premature Rupture of Membranes and Risk of Neonatal SepsisYudhi AuliaPas encore d'évaluation
- BR J Haematol - 2014 - Oteng Ntim - Pregnancy Outcome in Patients With Sickle Cell Disease in The UK A National CohortDocument9 pagesBR J Haematol - 2014 - Oteng Ntim - Pregnancy Outcome in Patients With Sickle Cell Disease in The UK A National CohortJustine ObedPas encore d'évaluation
- Clinical Risk Factor For Preeclamsia in Twin PregnanciesDocument8 pagesClinical Risk Factor For Preeclamsia in Twin PregnanciesLouis HadiyantoPas encore d'évaluation
- Biomarker 2Document8 pagesBiomarker 2Devianti TandialloPas encore d'évaluation
- Obstetrics Outcomes of Pregnancy With Uterine Fibroids in Tertiary Care HospitalDocument4 pagesObstetrics Outcomes of Pregnancy With Uterine Fibroids in Tertiary Care HospitalMohan Kumar DPas encore d'évaluation
- JurnalDocument6 pagesJurnalkiranaPas encore d'évaluation
- Hipertrofi Ventrikel Kiri PDFDocument11 pagesHipertrofi Ventrikel Kiri PDFdini kingkinPas encore d'évaluation
- 562 Full PDFDocument7 pages562 Full PDFkiranaPas encore d'évaluation
- KeperawatanDocument9 pagesKeperawatankiranaPas encore d'évaluation
- 281017Document9 pages281017kiranaPas encore d'évaluation
- Daftar PustakaDocument1 pageDaftar PustakakiranaPas encore d'évaluation
- Ilmu KeperawatanDocument1 pageIlmu KeperawatankiranaPas encore d'évaluation
- Abstract Book 2015-Web PDFDocument593 pagesAbstract Book 2015-Web PDFJulia Dwi ErayniPas encore d'évaluation
- 1 SM PDFDocument10 pages1 SM PDFkiranaPas encore d'évaluation
- Listening Journals For Extensive and Intensive Listening PracticeDocument10 pagesListening Journals For Extensive and Intensive Listening PracticeJoost ArxPas encore d'évaluation
- JurnalDocument6 pagesJurnalkiranaPas encore d'évaluation
- 5647 10976 1 SM PDFDocument7 pages5647 10976 1 SM PDFephaPas encore d'évaluation
- Music Therapy Benefits for Medical ConditionsDocument8 pagesMusic Therapy Benefits for Medical ConditionskiranaPas encore d'évaluation
- 1 s2.0 S1110569018300839 MainDocument4 pages1 s2.0 S1110569018300839 MainkiranaPas encore d'évaluation
- Pembelajaran Penyakit Terkait Perilaku Merokok Dan Edukasi Untuk Berhenti Merokok Di Pendidikan Dokter Fakultas Kedokteran UgmDocument16 pagesPembelajaran Penyakit Terkait Perilaku Merokok Dan Edukasi Untuk Berhenti Merokok Di Pendidikan Dokter Fakultas Kedokteran UgmkiranaPas encore d'évaluation
- Publikasi Llmiah: Fakultas Kedokteran Universitas SriwijayaDocument9 pagesPublikasi Llmiah: Fakultas Kedokteran Universitas SriwijayakiranaPas encore d'évaluation
- Terapi Origami Ank Sakit PDFDocument7 pagesTerapi Origami Ank Sakit PDFAnFi FaithfulPas encore d'évaluation
- THERACOM: A Systematic Review of The Evidence Base For Interventions To Improve Therapeutic Communications Between Black and Minority Ethnic Populations and Staff in Specialist Mental Health ServicesDocument11 pagesTHERACOM: A Systematic Review of The Evidence Base For Interventions To Improve Therapeutic Communications Between Black and Minority Ethnic Populations and Staff in Specialist Mental Health ServiceskiranaPas encore d'évaluation
- 4Document19 pages4kiranaPas encore d'évaluation
- Pengaruh Tarif Cukai Tembakau Dan Pesan Bergambar Bahaya Rokok Terhadap Konsumsi Rokok Di Banda AcehDocument15 pagesPengaruh Tarif Cukai Tembakau Dan Pesan Bergambar Bahaya Rokok Terhadap Konsumsi Rokok Di Banda AcehkiranaPas encore d'évaluation
- 1 s2.0 S1110569018300839 MainDocument4 pages1 s2.0 S1110569018300839 MainkiranaPas encore d'évaluation
- Bayi PrematureDocument4 pagesBayi PrematurekiranaPas encore d'évaluation
- JamuDocument8 pagesJamukiranaPas encore d'évaluation
- Using Standardized Patients To Teach Therapeutic Communication in Psychiatric NursingDocument20 pagesUsing Standardized Patients To Teach Therapeutic Communication in Psychiatric NursingkiranaPas encore d'évaluation
- 5Document19 pages5kiranaPas encore d'évaluation
- jh08003 PDFDocument8 pagesjh08003 PDFkiranaPas encore d'évaluation
- ID Analisis Pelaksanaan Tujuh Langkah Menuj PDFDocument8 pagesID Analisis Pelaksanaan Tujuh Langkah Menuj PDFheru joko santosoPas encore d'évaluation
- Computers & Education: Alan Gleaves, Caroline WalkerDocument13 pagesComputers & Education: Alan Gleaves, Caroline WalkerkiranaPas encore d'évaluation
- Aural 5Document13 pagesAural 5kiranaPas encore d'évaluation
- Science Checkpoint WorkbookDocument130 pagesScience Checkpoint WorkbookAgung PambudionoPas encore d'évaluation
- EFFECTS OF FEED FORMSDocument5 pagesEFFECTS OF FEED FORMSKhaeraniMahdinurAwliaPas encore d'évaluation
- An Introduction To Animal Diversity: Powerpoint Lectures ForDocument42 pagesAn Introduction To Animal Diversity: Powerpoint Lectures ForMonica AndrewsPas encore d'évaluation
- Illustrated Thesauru - Dorling KindersleyDocument258 pagesIllustrated Thesauru - Dorling KindersleyMarie98% (46)
- Taiji 24 Form - KellyDocument18 pagesTaiji 24 Form - Kellyanattā100% (3)
- Cats in Ancient Egypt Reading Comprehension Exercises - 28335Document2 pagesCats in Ancient Egypt Reading Comprehension Exercises - 28335RobinMagnus100% (2)
- Animal Farm by George Orwell Chapter 8Document13 pagesAnimal Farm by George Orwell Chapter 8TioLoloPas encore d'évaluation
- Isolation and Identification Ort From ChickenDocument14 pagesIsolation and Identification Ort From Chickenthanh ba matPas encore d'évaluation
- Endocrine SystemDocument8 pagesEndocrine SystemYenny AcostaPas encore d'évaluation
- 2 IcebreakerDocument1 page2 Icebreakerapi-248961865Pas encore d'évaluation
- 30.1 Organization of The Human BodyDocument30 pages30.1 Organization of The Human Bodymoniaguayo98Pas encore d'évaluation
- f3 Chapter 1Document33 pagesf3 Chapter 1ROSMA287Pas encore d'évaluation
- Countable Nouns & Uncountable Nouns: Norsarihan AhmadDocument21 pagesCountable Nouns & Uncountable Nouns: Norsarihan AhmadNoor AmizaPas encore d'évaluation
- Government Dental College ProspectusDocument27 pagesGovernment Dental College ProspectusManan PopatPas encore d'évaluation
- Bazaar Bargains Persona Peddling Peculiar Products with ProblemsDocument10 pagesBazaar Bargains Persona Peddling Peculiar Products with ProblemsSekcerPas encore d'évaluation
- Collection of business case studiesDocument2 pagesCollection of business case studiesJadiel AriasPas encore d'évaluation
- Sport in The Eastern Sudan - 1912Document308 pagesSport in The Eastern Sudan - 1912nevada desert ratPas encore d'évaluation
- Human A-Amylase and Starch Digestion: An Interesting MarriageDocument11 pagesHuman A-Amylase and Starch Digestion: An Interesting MarriagePratiksha RajpootPas encore d'évaluation
- 2 - The Five Temples of The Earthmother Part 1 - Life and MoonDocument22 pages2 - The Five Temples of The Earthmother Part 1 - Life and MoonMichael French100% (1)
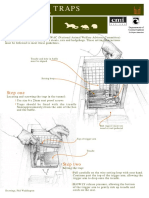
- Humane Stoat and Rodent Trap InstructionsDocument4 pagesHumane Stoat and Rodent Trap InstructionsGina FelyaPas encore d'évaluation
- Zodiac Academy Endocrine MCQDocument5 pagesZodiac Academy Endocrine MCQMourian AmanPas encore d'évaluation
- Q2 G3 Science M1Document40 pagesQ2 G3 Science M1Maricar AtienzaPas encore d'évaluation
- Singapore Zoo Magazine - 201103Document19 pagesSingapore Zoo Magazine - 201103The Real Shadow ReaverPas encore d'évaluation
- Nerve and Spinal Cord BiomechanicsDocument65 pagesNerve and Spinal Cord BiomechanicsZinneRah RahManPas encore d'évaluation
- MER-KA-BA MeditationDocument10 pagesMER-KA-BA MeditationmutationxPas encore d'évaluation
- Nunes, Et Al 2019Document8 pagesNunes, Et Al 2019Nathalia SantosPas encore d'évaluation
- DCRV PPT NowDocument22 pagesDCRV PPT NowKarthik RamanPas encore d'évaluation
- DolphinsDocument2 pagesDolphinsdeepPas encore d'évaluation
- List of Recent Land Mammals of Mexico, Ramírez-Pulido 2014Document76 pagesList of Recent Land Mammals of Mexico, Ramírez-Pulido 2014JhoancxdPas encore d'évaluation