Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Advancing Mutual Commitment: Joint Statement Following The 21st EU-Ukraine Summit Kyiv, 8 July 2019Document4 pagesAdvancing Mutual Commitment: Joint Statement Following The 21st EU-Ukraine Summit Kyiv, 8 July 2019La la landPas encore d'évaluation
- Ukraine: Economy ProfileDocument69 pagesUkraine: Economy ProfileLa la landPas encore d'évaluation
- Karin Cao Glu 2008Document3 pagesKarin Cao Glu 2008La la landPas encore d'évaluation
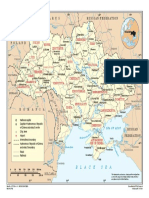
- Ukraine PDFDocument1 pageUkraine PDFLa la landPas encore d'évaluation
- Local Life Eindhoven - PDF Guide: Intro OnlineDocument5 pagesLocal Life Eindhoven - PDF Guide: Intro OnlineLa la landPas encore d'évaluation
- GIRL by Jamaica KincaidDocument2 pagesGIRL by Jamaica KincaidLa la landPas encore d'évaluation
- Selling Basics Selling Basics: TutorialDocument17 pagesSelling Basics Selling Basics: TutorialLa la landPas encore d'évaluation
- Icter FainDocument3 pagesIcter FainLa la landPas encore d'évaluation
- HTCE Visitors Map Bezoekers PlattegrondDocument2 pagesHTCE Visitors Map Bezoekers PlattegrondLa la landPas encore d'évaluation
- Floating Sauna Rosendal Norge 2003Document1 pageFloating Sauna Rosendal Norge 2003La la landPas encore d'évaluation
- Andronic LuminitaDocument7 pagesAndronic LuminitaLa la landPas encore d'évaluation
- Grigore Angelica 6Document4 pagesGrigore Angelica 6La la landPas encore d'évaluation
- 798Document1 page798La la landPas encore d'évaluation
- VGVGDocument1 pageVGVGLa la landPas encore d'évaluation
- B IBLIOGRAFIEDocument1 pageB IBLIOGRAFIELa la landPas encore d'évaluation
- National Collaborating Centre For Women's and Children's Health (UK) - London: RCOG Press 2010 May. (NICE Clinical Guidelines, No. 98.)Document1 pageNational Collaborating Centre For Women's and Children's Health (UK) - London: RCOG Press 2010 May. (NICE Clinical Guidelines, No. 98.)La la landPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- BLOODDocument175 pagesBLOODJohn JimsPas encore d'évaluation
- Blood Type Punnett Square PracticeDocument3 pagesBlood Type Punnett Square PracticeGary Garlan100% (1)
- Anatomy Module 17Document23 pagesAnatomy Module 17JayR MendonesPas encore d'évaluation
- Erythroblastosis Fetalis PDFDocument8 pagesErythroblastosis Fetalis PDFKathe Deanielle DayonPas encore d'évaluation
- Blood Group Test ProcedureDocument5 pagesBlood Group Test ProcedureNIRANJANA SHALINIPas encore d'évaluation
- BB - Detection and Identification of AntibodiesDocument10 pagesBB - Detection and Identification of AntibodiesWayne VillalunaPas encore d'évaluation
- RH Incompatibility Resource UnitDocument6 pagesRH Incompatibility Resource UnitJannah Marie A. DimaporoPas encore d'évaluation
- p1 Exam FinalDocument21 pagesp1 Exam FinalLeevine DelimaPas encore d'évaluation
- Quizlet BB CiullaDocument37 pagesQuizlet BB Ciullarollenas61Pas encore d'évaluation
- ImmunologyDocument5 pagesImmunologyKymi TanPas encore d'évaluation
- ABO and RH Blood Typing: AB ActsDocument4 pagesABO and RH Blood Typing: AB ActsRaja SharmaPas encore d'évaluation
- Genotype and Blood Group CompatibilityDocument5 pagesGenotype and Blood Group CompatibilityajayranjithPas encore d'évaluation
- Blood Transfusion in Clinical PracticeDocument284 pagesBlood Transfusion in Clinical PracticeshoneNNNPas encore d'évaluation
- هياDocument82 pagesهياrubayassir160Pas encore d'évaluation
- Table of Blood Group Systems v. 9.0 03-FEB-2021Document3 pagesTable of Blood Group Systems v. 9.0 03-FEB-2021AnthonyPas encore d'évaluation
- Krok 1 - 2018 (General Medicine) - EneutronDocument57 pagesKrok 1 - 2018 (General Medicine) - EneutronHarsh NimavatPas encore d'évaluation
- Scifed: PublishersDocument6 pagesScifed: PublishersNadiarosmaliaPas encore d'évaluation
- Chapter 40: Drugs Used in Obstetrics Test Bank: Multiple ChoiceDocument10 pagesChapter 40: Drugs Used in Obstetrics Test Bank: Multiple ChoiceNurse UtopiaPas encore d'évaluation
- Rhesus FactorDocument2 pagesRhesus FactormoneechoPas encore d'évaluation
- Transfusion Medicine - 2019Document126 pagesTransfusion Medicine - 2019Aria Jean MostajoPas encore d'évaluation
- Hardy Weinberg Problem SetDocument5 pagesHardy Weinberg Problem SetNur Syakira IsmailPas encore d'évaluation
- Molecular Biology of The RH Antigens: Use Only. For PersonalDocument14 pagesMolecular Biology of The RH Antigens: Use Only. For PersonaldeviPas encore d'évaluation
- Transfusion Support of Autoimmune Hemolytic AnemiaDocument7 pagesTransfusion Support of Autoimmune Hemolytic AnemiaMohamed ElmasryPas encore d'évaluation
- The Hazards: OF Blood TransfusionDocument7 pagesThe Hazards: OF Blood TransfusionPranjal Kr SahariaPas encore d'évaluation
- Forensic Chemistry ActivityDocument22 pagesForensic Chemistry ActivityStefanie Puguon Nipahoy100% (1)
- Anth SI 03 25 Bhasin M K TTDocument52 pagesAnth SI 03 25 Bhasin M K TTElma Silajdzic PertefPas encore d'évaluation
- Immuno HematologyDocument35 pagesImmuno HematologyAlan McLeanPas encore d'évaluation
- Blood Bank: Abo and RHDocument3 pagesBlood Bank: Abo and RHGwynne VelasquezPas encore d'évaluation
- Markscheme SL Paper1Document40 pagesMarkscheme SL Paper1Chintya Aurelyaa100% (1)