Vous aimerez peut-être aussi
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalD'EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalPas encore d'évaluation
- Current Therapeutic Advances in Chronic Interstitial CystitisDocument8 pagesCurrent Therapeutic Advances in Chronic Interstitial CystitisYylfordt GranzPas encore d'évaluation
- Diarrhea During Critical Illness A Multicenter PDFDocument10 pagesDiarrhea During Critical Illness A Multicenter PDFRejanne OliveiraPas encore d'évaluation
- Etiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisDocument8 pagesEtiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisakhmadPas encore d'évaluation
- JJZ 203Document1 pageJJZ 203Juan DiegoPas encore d'évaluation
- 12076Document7 pages12076Muhammad ZiaPas encore d'évaluation
- Alkaline IBSDocument9 pagesAlkaline IBSAnh LevanPas encore d'évaluation
- Diarrea en Enfermedad CríticaDocument10 pagesDiarrea en Enfermedad CríticaVíctor Pérez RiveroPas encore d'évaluation
- Effect of Vitamin D Supplementation on Primary Dysmenorrhea A Systematic Reviewand Meta-Analysis of Randomized Clinical TrialsDocument15 pagesEffect of Vitamin D Supplementation on Primary Dysmenorrhea A Systematic Reviewand Meta-Analysis of Randomized Clinical TrialsFransiska FranshuidPas encore d'évaluation
- Efficacy of Early Immunomodulator Therapy On The Outcomes of Crohn 'S DiseaseDocument6 pagesEfficacy of Early Immunomodulator Therapy On The Outcomes of Crohn 'S Diseasehusni gunawanPas encore d'évaluation
- D Yspepsia and Helicobacter Pylori Infection: A Prospective Multicentre Observational StudyDocument8 pagesD Yspepsia and Helicobacter Pylori Infection: A Prospective Multicentre Observational StudynageshkamatPas encore d'évaluation
- Perri2003 PDFDocument8 pagesPerri2003 PDFnageshkamatPas encore d'évaluation
- zhu2017Document9 pageszhu2017Hải TrầnPas encore d'évaluation
- ContentServer - Asp 13Document7 pagesContentServer - Asp 13Fitria NurulfathPas encore d'évaluation
- A Study On Acute Surgical Abdomen in Paediatric Age Group: Original Research ArticleDocument5 pagesA Study On Acute Surgical Abdomen in Paediatric Age Group: Original Research ArticleApple IdeaPas encore d'évaluation
- Paper 26Document4 pagesPaper 26fundj22Pas encore d'évaluation
- Title An Audit of Microbiological Tests in A Primary Care ClinicDocument20 pagesTitle An Audit of Microbiological Tests in A Primary Care ClinicHam FGPas encore d'évaluation
- 2022_lingyu_Acupuncture for the Treatment of Diarrhea-Predominant_ecaDocument11 pages2022_lingyu_Acupuncture for the Treatment of Diarrhea-Predominant_ecaesmargarPas encore d'évaluation
- Sii ArtículoDocument5 pagesSii ArtículoMonserrat Garduño FonsecaPas encore d'évaluation
- Clinical Outcomes of Esophagogastroduodenoscopy In.27Document6 pagesClinical Outcomes of Esophagogastroduodenoscopy In.27Agung KaryawinaraPas encore d'évaluation
- 11111111Document7 pages11111111Nejc KovačPas encore d'évaluation
- Appendicitis Clinical Pathway Implementations Compliance Evaluation in HospitalDocument4 pagesAppendicitis Clinical Pathway Implementations Compliance Evaluation in HospitalsuriPas encore d'évaluation
- The Role of Drotaverine in IbsDocument5 pagesThe Role of Drotaverine in IbsAli Abd AlrezaqPas encore d'évaluation
- Madisch Treatment of Irritable Bowel Syndrome With Herbal PreparationsDocument9 pagesMadisch Treatment of Irritable Bowel Syndrome With Herbal Preparationsoliffasalma atthahirohPas encore d'évaluation
- Upadacitinib Treatment Improves Symptoms of Bowel Urgency and Abdominal Pain, and Correlates With Quality of Life Improvements in Patients With Moderate To Severe Ulcerative ColitisDocument9 pagesUpadacitinib Treatment Improves Symptoms of Bowel Urgency and Abdominal Pain, and Correlates With Quality of Life Improvements in Patients With Moderate To Severe Ulcerative Colitisslt.hi468Pas encore d'évaluation
- ITU Comparacion 7 - 14 Dias de TtoDocument9 pagesITU Comparacion 7 - 14 Dias de TtoJohana Zamudio RojasPas encore d'évaluation
- 10 1016@j Ejogrb 2015 09 020Document5 pages10 1016@j Ejogrb 2015 09 020samuel tapia pardoPas encore d'évaluation
- Acupuncture Treatment in Gastrointestinal Diseases: A Systematic ReviewDocument8 pagesAcupuncture Treatment in Gastrointestinal Diseases: A Systematic ReviewVicTör Manuel Apölo-ğPas encore d'évaluation
- Chen. M SR and Three Level MADocument17 pagesChen. M SR and Three Level MASreeja CherukuruPas encore d'évaluation
- A Randomized Controlled Trial of Probiotics For Clostridium Dif Cile Infection in AdultsDocument4 pagesA Randomized Controlled Trial of Probiotics For Clostridium Dif Cile Infection in Adults林新中Pas encore d'évaluation
- The Effects of Abdominal I LOV U Massage Along With Lifestyle Training On Constipation and Distension in The Elderly With StrokeDocument9 pagesThe Effects of Abdominal I LOV U Massage Along With Lifestyle Training On Constipation and Distension in The Elderly With StrokeSuci NudiPas encore d'évaluation
- Alvorado ComparingDocument8 pagesAlvorado ComparingHarun NasutionPas encore d'évaluation
- Leaflet Preeklamsia BeratDocument6 pagesLeaflet Preeklamsia BeratSafitriPas encore d'évaluation
- Acyclovir Treatment Efficacy in Pemphigus VulgarisDocument3 pagesAcyclovir Treatment Efficacy in Pemphigus Vulgarissuci sukmawatiPas encore d'évaluation
- SIBO EritromicinaDocument8 pagesSIBO EritromicinaKat HerreraPas encore d'évaluation
- 1,2,Document11 pages1,2,Nejc KovačPas encore d'évaluation
- Trial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionDocument10 pagesTrial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionMeygan CórdovaPas encore d'évaluation
- Fit and Fecal Calprotectin 2020Document6 pagesFit and Fecal Calprotectin 2020sashadilanPas encore d'évaluation
- Multiplex Gastrointestinal Pentru ClinicieniDocument2 pagesMultiplex Gastrointestinal Pentru ClinicieniNadiPas encore d'évaluation
- 2022 JastreboffDocument12 pages2022 JastreboffSinityPas encore d'évaluation
- 1471 230X 7 9 PDFDocument5 pages1471 230X 7 9 PDFivanhariachandraPas encore d'évaluation
- Chen 2021Document8 pagesChen 2021metha anandaPas encore d'évaluation
- Enteral Nutrition Therapy For The Surgical PatientDocument52 pagesEnteral Nutrition Therapy For The Surgical PatientelenPas encore d'évaluation
- Research Paper Effectiveness of Conservative Management of Uncomplicated Acute Appendicitis: A Single Hospital Based Prospective StudyDocument8 pagesResearch Paper Effectiveness of Conservative Management of Uncomplicated Acute Appendicitis: A Single Hospital Based Prospective StudyAnsoriPas encore d'évaluation
- Short-Course Intraabdominal InfectionDocument10 pagesShort-Course Intraabdominal Infectionnicolás idárragaPas encore d'évaluation
- Effectiveness of Acupuncture in The Treatment of Hyperemesis Gravidarum - A Systematic Review and Meta-AnalysisDocument14 pagesEffectiveness of Acupuncture in The Treatment of Hyperemesis Gravidarum - A Systematic Review and Meta-Analysiswiwit vitaniaPas encore d'évaluation
- Ramirez 2013Document10 pagesRamirez 2013Nadia Farah FadhilaPas encore d'évaluation
- A Double Blind, Randomised, Placebo-Controlled Trial of Lactobacillus Acute Watery Diarrhoea in Vietnamese ChildrenDocument26 pagesA Double Blind, Randomised, Placebo-Controlled Trial of Lactobacillus Acute Watery Diarrhoea in Vietnamese ChildrenSeftiyantiPas encore d'évaluation
- Art 21054Document10 pagesArt 21054Ndhy Pharm HabibiePas encore d'évaluation
- FDA Approves Lilly's Omvoh - (Mirikizumab-Mrkz), A First-in-Class Treatment For Adults With Moderately To Severely Active Ulcerative ColitisDocument4 pagesFDA Approves Lilly's Omvoh - (Mirikizumab-Mrkz), A First-in-Class Treatment For Adults With Moderately To Severely Active Ulcerative ColitisOscar OrtegaPas encore d'évaluation
- El Tratamiento de La Obstrucción Del Intestino Delgado Con Un Fisioterapia Manual - Un Estudio de Eficacia Prospectivo.Document10 pagesEl Tratamiento de La Obstrucción Del Intestino Delgado Con Un Fisioterapia Manual - Un Estudio de Eficacia Prospectivo.DanielaPas encore d'évaluation
- 1741 7015 8 30Document8 pages1741 7015 8 30Andres HernándezPas encore d'évaluation
- Jurnal Jaki Prof VeniDocument38 pagesJurnal Jaki Prof Veniiman prawiraPas encore d'évaluation
- Clinical Effect of Catgut Implantation at AcupointsDocument8 pagesClinical Effect of Catgut Implantation at AcupointsJuan Pablo MejíaPas encore d'évaluation
- Bet 6 300Document6 pagesBet 6 300Victor SanchezPas encore d'évaluation
- Pi Is 0016508520300184Document12 pagesPi Is 0016508520300184ntnquynhproPas encore d'évaluation
- Abcesele FicatuluiDocument4 pagesAbcesele FicatuluiMihaela AlinaPas encore d'évaluation
- 5 02 Acute Abdominal PainDocument17 pages5 02 Acute Abdominal PainNereida LechugaPas encore d'évaluation
- CosentyxDocument10 pagesCosentyxsamar RamadanPas encore d'évaluation
- Jour Red UrticariaDocument6 pagesJour Red UrticariaErianaSariPas encore d'évaluation
- Referat Asma AnakDocument26 pagesReferat Asma Anakcamelia musaadPas encore d'évaluation
- Jurnal MH PDFDocument12 pagesJurnal MH PDFcamelia musaadPas encore d'évaluation
- Resources Used in This Design Url: Background - 3956685.htmDocument1 pageResources Used in This Design Url: Background - 3956685.htmcamelia musaadPas encore d'évaluation
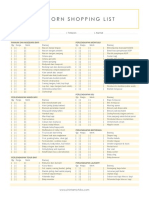
- Newborn Shopping List TemplateDocument1 pageNewborn Shopping List TemplateShellaCharismaAgryanandhaPas encore d'évaluation
- kjr-US For Benign and Maligna PDFDocument9 pageskjr-US For Benign and Maligna PDFLiaPas encore d'évaluation
- Ebm Jurnal PDFDocument198 pagesEbm Jurnal PDFcamelia musaadPas encore d'évaluation
- Jurnal Ebm KedkelDocument8 pagesJurnal Ebm Kedkelcamelia musaadPas encore d'évaluation
- Ebm JurnalDocument198 pagesEbm Jurnalcamelia musaadPas encore d'évaluation
- Surat Sponsor 1Document1 pageSurat Sponsor 1camelia musaadPas encore d'évaluation
- Epid, MK, ManagementDocument4 pagesEpid, MK, Managementcamelia musaadPas encore d'évaluation
- Surat Pernyataaan NPWPDocument1 pageSurat Pernyataaan NPWPcamelia musaadPas encore d'évaluation
- Management of Abcess CerebriDocument6 pagesManagement of Abcess Cerebricamelia musaadPas encore d'évaluation
- Brain Abscess in ChildrenDocument5 pagesBrain Abscess in Childrencamelia musaadPas encore d'évaluation
- Brain Abscess: H. R W, M.DDocument1 pageBrain Abscess: H. R W, M.Dcamelia musaadPas encore d'évaluation
- Plant Transport - IGCSE Biology Notes (2020)Document6 pagesPlant Transport - IGCSE Biology Notes (2020)Zhi En LeePas encore d'évaluation
- Sickle Cell AnemiaDocument7 pagesSickle Cell AnemiaJuma AwarPas encore d'évaluation
- 03 Chapter 3Document148 pages03 Chapter 3arghaPas encore d'évaluation
- Nervous Responses of EarthwormDocument27 pagesNervous Responses of EarthwormKayla JoezettePas encore d'évaluation
- Diencephalon PresentationDocument19 pagesDiencephalon Presentation300rPas encore d'évaluation
- Evolving Knowledge in Framing of Teratogenic Activity Towards Risk PerceptionDocument13 pagesEvolving Knowledge in Framing of Teratogenic Activity Towards Risk Perceptionsandy candyPas encore d'évaluation
- Effects of Different Fermentation Temperatures On Metabolites of KimchiDocument7 pagesEffects of Different Fermentation Temperatures On Metabolites of KimchiAngela ValdiviesoPas encore d'évaluation
- Physiology of Cerebellum Lec Foe 2nd Year by DR Sadia Uploaded by ZaighamDocument61 pagesPhysiology of Cerebellum Lec Foe 2nd Year by DR Sadia Uploaded by ZaighamZaigham HammadPas encore d'évaluation
- Comparison of the Fully Automated Urinalysis Analyzers UX-2000 and Cobas 6500Document10 pagesComparison of the Fully Automated Urinalysis Analyzers UX-2000 and Cobas 6500Sethulakshmi PharmacistPas encore d'évaluation
- Morphology of Flowering PlantsDocument13 pagesMorphology of Flowering Plantschiragbhaskar16Pas encore d'évaluation
- Management of PPHDocument1 pageManagement of PPH098 U.KARTHIK SARAVANA KANTHPas encore d'évaluation
- Part 8 Biological ScienceDocument5 pagesPart 8 Biological ScienceSteven CentenoPas encore d'évaluation
- Essay On Physical SelfDocument2 pagesEssay On Physical Selfcmestrada03Pas encore d'évaluation
- Biomimicry Avjeet SinghDocument21 pagesBiomimicry Avjeet SinghAvjeet SinghPas encore d'évaluation
- Protein Structure and Function Book ReviewDocument1 pageProtein Structure and Function Book ReviewBrunoPas encore d'évaluation
- Biology: Pearson EdexcelDocument24 pagesBiology: Pearson EdexcelAhmad MohdPas encore d'évaluation
- Starship Troopers Skinnies Army BookDocument66 pagesStarship Troopers Skinnies Army BookDougBirtles100% (5)
- Physiological Psychology ReviewerDocument13 pagesPhysiological Psychology ReviewerLeopando Rod CyrenzPas encore d'évaluation
- E-Portfolio Injection Study GuideDocument7 pagesE-Portfolio Injection Study Guideapi-366034042Pas encore d'évaluation
- Thesis Olof HerttingDocument57 pagesThesis Olof HerttingAjay IyerPas encore d'évaluation
- 2010 FulltextDocument410 pages2010 FulltextNajam Din SahitoPas encore d'évaluation
- Artigo Sobre Nutrigenômica e Nutrigenética PDFDocument18 pagesArtigo Sobre Nutrigenômica e Nutrigenética PDFDiogo JuniorPas encore d'évaluation
- The Antibacterial Properties of Isothiocyanates PDFDocument15 pagesThe Antibacterial Properties of Isothiocyanates PDFSasicha DoungsuwanPas encore d'évaluation
- Sample Lab ReportDocument7 pagesSample Lab ReportPutri Syalieyana0% (1)
- NSABB Final Report Recommendations Evaluation Oversight Proposed Gain of Function Research May 2016Document109 pagesNSABB Final Report Recommendations Evaluation Oversight Proposed Gain of Function Research May 2016Jim Hoft100% (1)
- Zoologija VrsteDocument16 pagesZoologija VrsteДушан МарковићPas encore d'évaluation
- Advt - R-09-2023 WT ResultDocument16 pagesAdvt - R-09-2023 WT ResultAvinash Kumar SinghPas encore d'évaluation
- Citric Acid Production Stirred TankDocument9 pagesCitric Acid Production Stirred TankKarliiux MedinaPas encore d'évaluation
- MDU Open Elective 3rd Sem Date Sheet May 2019Document1 pageMDU Open Elective 3rd Sem Date Sheet May 2019Ratan DeshPas encore d'évaluation
- Kingdom Protista: Diverse Eukaryotic MicroorganismsDocument79 pagesKingdom Protista: Diverse Eukaryotic MicroorganismsMeah PachecoPas encore d'évaluation
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (13)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Breaking the Habit of Being YourselfD'EverandBreaking the Habit of Being YourselfÉvaluation : 4.5 sur 5 étoiles4.5/5 (1455)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BePas encore d'évaluation
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 3.5 sur 5 étoiles3.5/5 (3)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipD'EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipÉvaluation : 4.5 sur 5 étoiles4.5/5 (1135)
- Techniques Exercises And Tricks For Memory ImprovementD'EverandTechniques Exercises And Tricks For Memory ImprovementÉvaluation : 4.5 sur 5 étoiles4.5/5 (40)
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 5 sur 5 étoiles5/5 (4)
- Deep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!D'EverandDeep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Évaluation : 4.5 sur 5 étoiles4.5/5 (10)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingD'EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingÉvaluation : 4.5 sur 5 étoiles4.5/5 (103)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsD'EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsÉvaluation : 4.5 sur 5 étoiles4.5/5 (169)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisD'EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingD'EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (33)
- The Happiness Trap: How to Stop Struggling and Start LivingD'EverandThe Happiness Trap: How to Stop Struggling and Start LivingÉvaluation : 4 sur 5 étoiles4/5 (1)
- The Ultimate Guide To Memory Improvement TechniquesD'EverandThe Ultimate Guide To Memory Improvement TechniquesÉvaluation : 5 sur 5 étoiles5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingD'EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingÉvaluation : 5 sur 5 étoiles5/5 (5)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeD'EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeÉvaluation : 4.5 sur 5 étoiles4.5/5 (253)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)