Vous aimerez peut-être aussi
- Cell Cycle Lesson PlanDocument4 pagesCell Cycle Lesson PlanJustine Pama94% (17)
- SyncopeDocument10 pagesSyncopeHNINPas encore d'évaluation
- ECG Rhythm Strip Interpretation Lesson 4Document5 pagesECG Rhythm Strip Interpretation Lesson 4phoebjaetanPas encore d'évaluation
- Principles of Endocrinology and Hormone PDFDocument794 pagesPrinciples of Endocrinology and Hormone PDFleogmail100% (4)
- A New Furileusaurian Abelisaurid From La Invernada Upper Cretaceous Santonian Bajo de La Carpa Formation Northern Patagonia ArgentinaDocument29 pagesA New Furileusaurian Abelisaurid From La Invernada Upper Cretaceous Santonian Bajo de La Carpa Formation Northern Patagonia ArgentinaStuff NewsroomPas encore d'évaluation
- Blue Bio V DoH and HFMADocument21 pagesBlue Bio V DoH and HFMAShane StarlingPas encore d'évaluation
- Stroke: Clinical Presentation and Anatomical LocalizationDocument36 pagesStroke: Clinical Presentation and Anatomical LocalizationYusuf JoganPas encore d'évaluation
- Cerebrovascular Disorders: Causes, Types, Symptoms & Treatment of StrokesDocument4 pagesCerebrovascular Disorders: Causes, Types, Symptoms & Treatment of StrokesMhae De GuzmanPas encore d'évaluation
- 2 Dyphasia DysarthriaDocument4 pages2 Dyphasia DysarthriamuhammadridhwanPas encore d'évaluation
- Dysarthria and DysphasiaDocument8 pagesDysarthria and DysphasiaNazirah AlanPas encore d'évaluation
- StrokeDocument55 pagesStrokeOgechi Grace OkoliPas encore d'évaluation
- Diagnosis and Management of Acute StrokeDocument74 pagesDiagnosis and Management of Acute StrokeDonnaBells Hermo Labaniego100% (2)
- Manage Stroke with Tests, Treatments & PreventionDocument27 pagesManage Stroke with Tests, Treatments & PreventionHanif SumonPas encore d'évaluation
- Acute CNS Infections Diagnosis GuideDocument53 pagesAcute CNS Infections Diagnosis GuideEhab KhiryPas encore d'évaluation
- Cerebrovascular AccidentDocument62 pagesCerebrovascular AccidentJaydee DalayPas encore d'évaluation
- A Clinical Approach To SyncopeDocument8 pagesA Clinical Approach To Syncopepuskesmas tarik100% (1)
- Neck Trauma LecDocument49 pagesNeck Trauma Lecapi-3743483100% (2)
- Internal Medicine Sample Osce Examination Component Questions eDocument2 pagesInternal Medicine Sample Osce Examination Component Questions eFajar ChampionPas encore d'évaluation
- NIH Aids Info HIV Treatment Guidelines AdultandadolescentglDocument267 pagesNIH Aids Info HIV Treatment Guidelines Adultandadolescentglbmartindoyle6396Pas encore d'évaluation
- Thyroid DisordersDocument21 pagesThyroid DisordersSuliman GarallehPas encore d'évaluation
- AtaxiaDocument23 pagesAtaxiakara_korumPas encore d'évaluation
- Cerebrovascular Accident (Stroke)Document15 pagesCerebrovascular Accident (Stroke)mesdejen100% (1)
- Traumatic Brain Injury Tbi Overview of Diagnosis and Treatment 2155 9562-5-182Document10 pagesTraumatic Brain Injury Tbi Overview of Diagnosis and Treatment 2155 9562-5-182Rence PieterszPas encore d'évaluation
- Systemic Lupus ErythematosusDocument51 pagesSystemic Lupus ErythematosusEmma AndayaPas encore d'évaluation
- Cns ExaminationDocument17 pagesCns ExaminationJuana Maria Garcia Espinoza100% (1)
- 09 - Congenital SyndromesDocument76 pages09 - Congenital SyndromesROHIT100% (1)
- Causes, Symptoms & Types of Cerebral InfarctionDocument2 pagesCauses, Symptoms & Types of Cerebral InfarctionMarie Aurora Gielbert MarianoPas encore d'évaluation
- Localizing The LesionDocument30 pagesLocalizing The LesionTracy NwannePas encore d'évaluation
- Assesment Chest PainDocument9 pagesAssesment Chest PainIpar Day100% (2)
- StrokeDocument19 pagesStrokesridhar100% (4)
- VALVULAR HEART DISEASE GUIDEDocument69 pagesVALVULAR HEART DISEASE GUIDEAbanoub AwadallaPas encore d'évaluation
- Traumatic Brain Injury: Dan Sprando Andres TabaresDocument31 pagesTraumatic Brain Injury: Dan Sprando Andres Tabaresanony7546 pop100% (1)
- MenorrhagiaDocument4 pagesMenorrhagiaFlloyd_Martin__1259Pas encore d'évaluation
- ST-Elevation Myocardial Infarction (Stemi) : Present byDocument29 pagesST-Elevation Myocardial Infarction (Stemi) : Present byReema AlamriPas encore d'évaluation
- Aortic Stenosis, Mitral Regurgitation, Pulmonary Stenosis, and Tricuspid Regurgitation: Causes, Symptoms, Signs, and TreatmentDocument7 pagesAortic Stenosis, Mitral Regurgitation, Pulmonary Stenosis, and Tricuspid Regurgitation: Causes, Symptoms, Signs, and TreatmentChuu Suen TayPas encore d'évaluation
- Masterclass in Internal MedicineDocument4 pagesMasterclass in Internal MedicineLydia IsaacPas encore d'évaluation
- CardiomyopathyDocument23 pagesCardiomyopathyDefyna Dwi LestariPas encore d'évaluation
- HEMOLYSISDocument2 pagesHEMOLYSISchandra-vinnakotaPas encore d'évaluation
- Neuroradiology Case PresentationDocument13 pagesNeuroradiology Case PresentationIsraelVimos100% (1)
- Acute Stroke Management by Carlos L Chua PDFDocument61 pagesAcute Stroke Management by Carlos L Chua PDFHynne Jhea EchavezPas encore d'évaluation
- Surgery 2012Document28 pagesSurgery 2012max_21ruPas encore d'évaluation
- Gullian BarreDocument3 pagesGullian Barreapi-38224330% (1)
- Movement Disorders BabcockDocument19 pagesMovement Disorders BabcockBaiq Trisna SatrianaPas encore d'évaluation
- ICP Waveform Analysis: Understanding Intracranial Physiology & MonitoringDocument55 pagesICP Waveform Analysis: Understanding Intracranial Physiology & MonitoringMaddox EdeyajPas encore d'évaluation
- EVDDocument2 pagesEVDLidya ZhuangPas encore d'évaluation
- ASCITESDocument25 pagesASCITESGanesh BabuPas encore d'évaluation
- #9 Ie 8 PDFDocument8 pages#9 Ie 8 PDFOmar BasimPas encore d'évaluation
- Headache, CithaDocument20 pagesHeadache, CithaCitha TallesangPas encore d'évaluation
- Pediatric Hematology LectureDocument84 pagesPediatric Hematology LectureloitaPas encore d'évaluation
- Abdominal Swelling + AscitesDocument29 pagesAbdominal Swelling + AscitesDevina CiayadiPas encore d'évaluation
- Notes On History Taking in The Cardiovascular SystemDocument9 pagesNotes On History Taking in The Cardiovascular Systemmdjohar72100% (1)
- Neurology Part 1Document155 pagesNeurology Part 1nursereview100% (10)
- Patent Ductus ArteriosusDocument31 pagesPatent Ductus ArteriosussuderiPas encore d'évaluation
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- Alarm Bells in Medicine: Danger Symptoms in Medicine, Surgery and Clinical SpecialtiesD'EverandAlarm Bells in Medicine: Danger Symptoms in Medicine, Surgery and Clinical SpecialtiesNadeem AliPas encore d'évaluation
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- Cerebrovascular Ultrasound in Stroke Prevention and TreatmentD'EverandCerebrovascular Ultrasound in Stroke Prevention and TreatmentÉvaluation : 5 sur 5 étoiles5/5 (1)
- The Science of HHDocument3 pagesThe Science of HHPAK DHEPas encore d'évaluation
- UnitedDocument1 pageUnitedPAK DHEPas encore d'évaluation
- Data RahasiaDocument1 pageData RahasiaPAK DHEPas encore d'évaluation
- SecuredDocument1 pageSecuredPAK DHEPas encore d'évaluation
- Mechanisms of Cardiac Arrhythmias From Automatici+Document24 pagesMechanisms of Cardiac Arrhythmias From Automatici+Malar MannanPas encore d'évaluation
- The Normal Anterior Inferior Cerebellar ArteryDocument19 pagesThe Normal Anterior Inferior Cerebellar Artery16fernandoPas encore d'évaluation
- Uji Aktivitas Antioksidan Ekstrak Etanol 70% Bunga Telang (Clitoria TernateaL) Dari Daerah Sleman Dengan Metode DPPHDocument7 pagesUji Aktivitas Antioksidan Ekstrak Etanol 70% Bunga Telang (Clitoria TernateaL) Dari Daerah Sleman Dengan Metode DPPHAnastasia FebruestiPas encore d'évaluation
- Exam 3 NotesDocument3 pagesExam 3 NotesStanley ChuPas encore d'évaluation
- 3.03 Understand Structures, Functions and Disorders of The Nervous SystemDocument38 pages3.03 Understand Structures, Functions and Disorders of The Nervous SystemLoriwinchesterPas encore d'évaluation
- Auxin Controls Seed Dormacy in Arabidopsis (Liu, Et Al.)Document6 pagesAuxin Controls Seed Dormacy in Arabidopsis (Liu, Et Al.)Jet Lee OlimberioPas encore d'évaluation
- SGD Physiology Endocrine and MetabolismDocument7 pagesSGD Physiology Endocrine and MetabolismTinesh RajahPas encore d'évaluation
- L.D..Occlusion in FPDDocument138 pagesL.D..Occlusion in FPDApurva Deshmukh67% (3)
- Phylum Arthropoda - Why such abundance and diversityDocument4 pagesPhylum Arthropoda - Why such abundance and diversitySHILPas encore d'évaluation
- January 2016 (IAL) QP - Unit 1 Edexcel Biology A-LevelDocument24 pagesJanuary 2016 (IAL) QP - Unit 1 Edexcel Biology A-LevelkirthikaPas encore d'évaluation
- T2DMDocument24 pagesT2DMXyra BadangayonPas encore d'évaluation
- Blood Buffer SystemDocument10 pagesBlood Buffer Systemmd hasib munsiPas encore d'évaluation
- Assignment Lec 4Document3 pagesAssignment Lec 4morriganPas encore d'évaluation
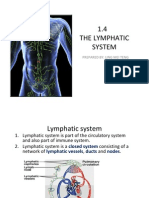
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDocument15 pages1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingPas encore d'évaluation
- Pathogenesis of AtherosclerosisDocument21 pagesPathogenesis of Atherosclerosishakky gamyPas encore d'évaluation
- Focusing Instruction ManualDocument15 pagesFocusing Instruction Manualplan2222100% (1)
- Biology PDFDocument1 447 pagesBiology PDFPrincess Ethel Atillo100% (2)
- Chronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsDocument7 pagesChronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsAnonymous FgT04krgymPas encore d'évaluation
- 2016 - 13 - Fleming - Lagged Syndesmotic Fixation - Our Clinical ExperienceDocument8 pages2016 - 13 - Fleming - Lagged Syndesmotic Fixation - Our Clinical ExperienceJacob DoughertyPas encore d'évaluation
- Nicotrol InhalerDocument19 pagesNicotrol InhalerdebysiskaPas encore d'évaluation
- MRCP 2 Nephrology NOTESDocument74 pagesMRCP 2 Nephrology NOTESMuhammad HaneefPas encore d'évaluation
- Six Elements and Chinese MedicineDocument182 pagesSix Elements and Chinese MedicinePedro Maia67% (3)
- 8Document6 pages8rajanPas encore d'évaluation
- Upper Limb MCQsDocument50 pagesUpper Limb MCQsstephen victory100% (1)
- Paragraph Development ExerciseDocument6 pagesParagraph Development ExerciseSYAFINAS SALAM100% (1)