Vous aimerez peut-être aussi
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeD'EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengePas encore d'évaluation
- Clinical Management of TB and HIVDocument154 pagesClinical Management of TB and HIVapi-3781623100% (3)
- Smear Negative TBDocument53 pagesSmear Negative TBsyuhaida deqsuPas encore d'évaluation
- Crypto C CocusDocument26 pagesCrypto C CocusBrinna Anindita SatriaPas encore d'évaluation
- MENINGITIS DR Syad Akram Ali 01-12-2014Document95 pagesMENINGITIS DR Syad Akram Ali 01-12-2014Gopireddy Sivakarthik ReddyPas encore d'évaluation
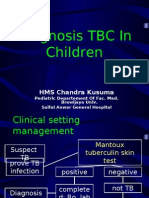
- Diagnosis TBDocument44 pagesDiagnosis TBGede Eka Putra NugrahaPas encore d'évaluation
- Morning Report Case: October 27 2010Document33 pagesMorning Report Case: October 27 2010Felicia adeline ChristianPas encore d'évaluation
- HIV Neurology: Graeme MeintjesDocument75 pagesHIV Neurology: Graeme MeintjesPrincess MiraPas encore d'évaluation
- Tos-Disnea: Dr. Eduardo GotuzzoDocument24 pagesTos-Disnea: Dr. Eduardo GotuzzoJuan AlbújarPas encore d'évaluation
- Cap DR YuvaDocument169 pagesCap DR YuvaYuvarajan SivaPas encore d'évaluation
- An Interesting Case of Unresolved PneumoniaDocument40 pagesAn Interesting Case of Unresolved PneumoniaJeevankumar DommarajuPas encore d'évaluation
- 2.2 TB DiagnosisDocument19 pages2.2 TB Diagnosisdwisuci91Pas encore d'évaluation
- Pozniak Tuberculosis & OI EACS 2008Document88 pagesPozniak Tuberculosis & OI EACS 2008ovidiuroscaPas encore d'évaluation
- PBL #3 Pulmonary Tuberculosis Group (A)Document77 pagesPBL #3 Pulmonary Tuberculosis Group (A)mohammedPas encore d'évaluation
- Tubercular MeningitisDocument60 pagesTubercular MeningitisVRUSHAB PARAPPANAVARPas encore d'évaluation
- Febrile Neutropenia Final 7-29Document74 pagesFebrile Neutropenia Final 7-29Juliyanti FuPas encore d'évaluation
- Cursuri TBDocument52 pagesCursuri TBDumitru ChesovPas encore d'évaluation
- Pneumonia PDFDocument68 pagesPneumonia PDFfatiniPas encore d'évaluation
- Lapkas Selasa-1Document23 pagesLapkas Selasa-1----Pas encore d'évaluation
- Oncologic EmergenciesDocument43 pagesOncologic Emergencieshernandez2812Pas encore d'évaluation
- 13-Community Acquired PneumoniaDocument50 pages13-Community Acquired PneumoniaRubina MasihPas encore d'évaluation
- Shamim Reza CPD Pneumonea Near FinalDocument50 pagesShamim Reza CPD Pneumonea Near FinalMinhajul IslamPas encore d'évaluation
- Clinical Presentation and Diagnosis of Tuberculosis: International Standards 1-5Document51 pagesClinical Presentation and Diagnosis of Tuberculosis: International Standards 1-5Restu MegantaraPas encore d'évaluation
- Pneumonia Panel GuidelineDocument8 pagesPneumonia Panel Guidelineilham perdiansyahPas encore d'évaluation
- Penatalaksanaan TB Pada OdhaDocument80 pagesPenatalaksanaan TB Pada Odhasuho exoPas encore d'évaluation
- Clinical Diagnosis Nov2009 (Autosaved)Document51 pagesClinical Diagnosis Nov2009 (Autosaved)SantiFaridKalukuPas encore d'évaluation
- TB-HIV Private PhysiciansDocument66 pagesTB-HIV Private PhysiciansZulhelmiPas encore d'évaluation
- 8.11.08 Davis-Hovda. TB PleurisyDocument13 pages8.11.08 Davis-Hovda. TB Pleurisycecilia casandraPas encore d'évaluation
- 05 Investigations For PneumoniaDocument4 pages05 Investigations For Pneumoniause4mePas encore d'évaluation
- DR Oea KhairsyafDocument30 pagesDR Oea KhairsyafErdyPas encore d'évaluation
- DR As TuberculosisDocument59 pagesDR As TuberculosisAchhar SinghPas encore d'évaluation
- BP: HR: RR: Temp:: CBC Count Pulse Oximetry (Oxygen Saturation) CreatinineDocument2 pagesBP: HR: RR: Temp:: CBC Count Pulse Oximetry (Oxygen Saturation) CreatinineroshmaePas encore d'évaluation
- JurDing TB RadiologiDocument29 pagesJurDing TB Radiologiradiologi2018Pas encore d'évaluation
- Pleural Diseases: Farhad Mazdisnian, MD, FCCP Pulmonary and Critical Care Medicine Va Long Beach Medical CenterDocument46 pagesPleural Diseases: Farhad Mazdisnian, MD, FCCP Pulmonary and Critical Care Medicine Va Long Beach Medical CenterderereyPas encore d'évaluation
- 8.11.08 Davis-Hovda. TB PleurisyDocument13 pages8.11.08 Davis-Hovda. TB Pleurisyrisda aulia putriPas encore d'évaluation
- Acute Pulmonary Infections: Zen Ahmad Medical Faculty, Sriwijaya UniversityDocument38 pagesAcute Pulmonary Infections: Zen Ahmad Medical Faculty, Sriwijaya UniversitymayaPas encore d'évaluation
- Q&A Oslo Revisi 61023Document10 pagesQ&A Oslo Revisi 61023syukriPas encore d'évaluation
- Pneumonia - Taking Your Breath Away: Dr. S. BalamuruganDocument85 pagesPneumonia - Taking Your Breath Away: Dr. S. BalamuruganBalamurugan SanthalingamPas encore d'évaluation
- Pneumonia: Dr. Tjatur Winarsanto SPPDDocument46 pagesPneumonia: Dr. Tjatur Winarsanto SPPDanisamayaPas encore d'évaluation
- PK - Aspek Laboratorium Respirasi - Dr. AnnaDocument48 pagesPK - Aspek Laboratorium Respirasi - Dr. AnnaMUHAMMAD ILHAM PRATAMAPas encore d'évaluation
- Bronchopneumonia PP 2003Document31 pagesBronchopneumonia PP 2003Rizky FadhilaPas encore d'évaluation
- Gambaran Radiologi TuberkulosisDocument36 pagesGambaran Radiologi TuberkulosisNathania PutriPas encore d'évaluation
- Grand Round July 2019Document61 pagesGrand Round July 2019Arslan Rahat UllahPas encore d'évaluation
- Tuberculosis or TBDocument8 pagesTuberculosis or TBJ Russel DichosoPas encore d'évaluation
- Adult Meningitis in A Setting in High Hiv and TB Prevalence: Finding From 4961 Suspected CasesDocument26 pagesAdult Meningitis in A Setting in High Hiv and TB Prevalence: Finding From 4961 Suspected CasesFastiati RAPas encore d'évaluation
- Current Management of Fungal Urinary Tract Infection and FunguriaDocument47 pagesCurrent Management of Fungal Urinary Tract Infection and FunguriaFeysel JemalPas encore d'évaluation
- CAP by DR SarmaDocument76 pagesCAP by DR SarmaTina ReisaPas encore d'évaluation
- 3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualDocument28 pages3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualjimmyneumologiaPas encore d'évaluation
- Tuberculosis PowerpointDocument69 pagesTuberculosis PowerpointCeline Villo100% (1)
- 8.11.08 Davis-Hovda. TB PleurisyDocument13 pages8.11.08 Davis-Hovda. TB Pleurisyawaniedream8391Pas encore d'évaluation
- Meningitis 2005Document87 pagesMeningitis 2005nafisyarifahPas encore d'évaluation
- Tuberculosis in Otorhinolaryngology: Clinical Presentation and Diagnostic ChallengesDocument18 pagesTuberculosis in Otorhinolaryngology: Clinical Presentation and Diagnostic ChallengestrznaTN1922Pas encore d'évaluation
- Progressive Primary Pulmonary TB in A 15-Month Old ChildDocument1 pageProgressive Primary Pulmonary TB in A 15-Month Old ChildRenierose AgujetasPas encore d'évaluation
- Lung MycosisDocument80 pagesLung MycosisWisnu Omadi100% (2)
- Neutropenic SepsisDocument38 pagesNeutropenic SepsisYS NatePas encore d'évaluation
- Evaluation of In-Patients With FeverDocument125 pagesEvaluation of In-Patients With FeverStangPongritPas encore d'évaluation
- Dr. R V S N Sarma., MD., MSC., (Canada) Consultant Physician & Chest Specialist Visit Us At: WWW - Drsarma.InDocument76 pagesDr. R V S N Sarma., MD., MSC., (Canada) Consultant Physician & Chest Specialist Visit Us At: WWW - Drsarma.InAndry Wahyudi AgusPas encore d'évaluation
- Review Afb Neg CultureDocument7 pagesReview Afb Neg Cultureธิรดา สายสตรอง สายจำปาPas encore d'évaluation
- Infectious MononucleosisDocument35 pagesInfectious MononucleosisShv Naga100% (1)
- Al-Azhar Assiut Medical Journal Aamj, Vol 13, No 4, October 2015 Suppl-2Document6 pagesAl-Azhar Assiut Medical Journal Aamj, Vol 13, No 4, October 2015 Suppl-2Vincentius Michael WilliantoPas encore d'évaluation
- Bcs3214 Practical 4Document8 pagesBcs3214 Practical 4Ahmad Farhan Ahmad MisbahPas encore d'évaluation
- Pathogen Safety Data SheetsDocument9 pagesPathogen Safety Data Sheetsmike rezekiPas encore d'évaluation
- MPH Comprreehensive Examination 2016 Recall Questions: RationaleDocument6 pagesMPH Comprreehensive Examination 2016 Recall Questions: RationaleReg LagartejaPas encore d'évaluation
- Sepsis Nursing OutlineDocument6 pagesSepsis Nursing OutlineSavannah Hayden100% (1)
- Zoonotic DiseasesDocument11 pagesZoonotic Diseasesapi-422995346Pas encore d'évaluation
- Hes 032 Lec Long Quiz 1 BSN 2 A11Document24 pagesHes 032 Lec Long Quiz 1 BSN 2 A11Sabrina MascardoPas encore d'évaluation
- Chapter 8 - Transport in MammalsDocument119 pagesChapter 8 - Transport in Mammalsapi-3728508100% (1)
- 9.2-Epidemiology of Infectious DiseasesDocument67 pages9.2-Epidemiology of Infectious DiseasesMarin Jr., Reynaldo J.Pas encore d'évaluation
- Cough, Hemoptysis, Dyspnea, WheezingDocument43 pagesCough, Hemoptysis, Dyspnea, WheezingMelissa SalayogPas encore d'évaluation
- Case Report Bacterial MeningitisDocument13 pagesCase Report Bacterial Meningitisbonziebuddy100% (1)
- CURS - ENGLEZA - Boli Infectioase PDFDocument246 pagesCURS - ENGLEZA - Boli Infectioase PDFLesan IulianaPas encore d'évaluation
- Daftar PustakaDocument2 pagesDaftar PustakaLucky Arie SandiPas encore d'évaluation
- Etiology, Clinical Manifestations, and Diagnosis of Nephrotic Syndrome in Children - UpToDateDocument18 pagesEtiology, Clinical Manifestations, and Diagnosis of Nephrotic Syndrome in Children - UpToDateAngga Julyananda PradanaPas encore d'évaluation
- Auspar Efmoroctocog Alfa Rhu 150317Document51 pagesAuspar Efmoroctocog Alfa Rhu 150317Tatiana MirendaPas encore d'évaluation
- Blood Fluid Examination StrasingerDocument4 pagesBlood Fluid Examination StrasingerChristin SchlittPas encore d'évaluation
- Algae, Fungi and ProtozoaDocument53 pagesAlgae, Fungi and ProtozoaMirza Salman BaigPas encore d'évaluation
- 1 s2.0 S1201971210000354 Main PDFDocument189 pages1 s2.0 S1201971210000354 Main PDFSABA YOUNASPas encore d'évaluation
- Biology HSC Questions ARC 2006Document28 pagesBiology HSC Questions ARC 2006timeflies23Pas encore d'évaluation
- Flu and The Flu VaccineDocument3 pagesFlu and The Flu VaccinenursunbPas encore d'évaluation
- Leach Et Al 2021 - Post-Pandemic Transformations How and Why COVID-19 Requires Us To Rethink DevelopmentDocument12 pagesLeach Et Al 2021 - Post-Pandemic Transformations How and Why COVID-19 Requires Us To Rethink DevelopmentArlindo FortesPas encore d'évaluation
- RRB NTPC 2016 All Shift Ques With AnsDocument13 pagesRRB NTPC 2016 All Shift Ques With AnsAnkitRajGhoshPas encore d'évaluation
- Food Safety Issues in Asia, SEAFAST PDFDocument35 pagesFood Safety Issues in Asia, SEAFAST PDFRezaAbdifiPas encore d'évaluation
- Autoimmune Hemolytic AnemiaDocument7 pagesAutoimmune Hemolytic AnemiaHoopmen SilaenPas encore d'évaluation
- Mikrobiologi Klinik FK UNUD: Use of Colony Morphology For The Presumptive Identification of MicroorganismsDocument12 pagesMikrobiologi Klinik FK UNUD: Use of Colony Morphology For The Presumptive Identification of Microorganismssgd2josPas encore d'évaluation
- Session 1 Introduction To ParasitologyDocument33 pagesSession 1 Introduction To Parasitologyannelle0219Pas encore d'évaluation
- Hernandez, Et Al.Document11 pagesHernandez, Et Al.Yet Barreda BasbasPas encore d'évaluation
- Serological TestsDocument2 pagesSerological TestsKimberly EspaldonPas encore d'évaluation
- Ipm Fruit Crops 23022015 PDFDocument92 pagesIpm Fruit Crops 23022015 PDFprudhvi_hyd100% (1)
- Prof. Saman WimalasunderaDocument68 pagesProf. Saman Wimalasunderainam khanPas encore d'évaluation
- RUQ MassDocument20 pagesRUQ MassCathy CepedaPas encore d'évaluation