Vous aimerez peut-être aussi
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- PUCAN, Julienne BSN III-D - SGD - HYPO&HYPERCHLOREMIADocument10 pagesPUCAN, Julienne BSN III-D - SGD - HYPO&HYPERCHLOREMIAJulienne PucanPas encore d'évaluation
- Albendazole - Drug Information PDFDocument7 pagesAlbendazole - Drug Information PDFjjjkkPas encore d'évaluation
- A Case Study On Uterine MyomaDocument39 pagesA Case Study On Uterine MyomaAj GoPas encore d'évaluation
- Biliary AtresiaDocument8 pagesBiliary AtresiaBrooke MauriPas encore d'évaluation
- A Case Analysis OnDocument27 pagesA Case Analysis Onbunso padillaPas encore d'évaluation
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarPas encore d'évaluation
- Drug Study Case 1Document37 pagesDrug Study Case 1Maria Charis Anne IndananPas encore d'évaluation
- Thromboangiitis Obliterans (Buerger's Disease): A Case PresentationDocument16 pagesThromboangiitis Obliterans (Buerger's Disease): A Case PresentationYan VencerPas encore d'évaluation
- Case Study Benign Tumors of The Uterus: MyomaDocument3 pagesCase Study Benign Tumors of The Uterus: MyomaToto RyanPas encore d'évaluation
- Case StudyDocument49 pagesCase StudyLennie Marie B Pelaez100% (1)
- Normal Spontaneous DeliveryDocument64 pagesNormal Spontaneous DeliveryMichellin Andres MarianoPas encore d'évaluation
- Drug Study on CelecoxibDocument11 pagesDrug Study on CelecoxibPrincess Brigitte R. PATE�APas encore d'évaluation
- ICS Pedia WardDocument8 pagesICS Pedia Wardsweet061991Pas encore d'évaluation
- Appendicitis Signs and Symptoms GuideDocument40 pagesAppendicitis Signs and Symptoms GuideHeart TolenadaPas encore d'évaluation
- Pathophysiology of AGEDocument1 pagePathophysiology of AGEYum CPas encore d'évaluation
- Post C-Section Delivery Care PlanDocument5 pagesPost C-Section Delivery Care Planᒙᕧᖇᕦᙏᖻ ᗴᔛᓦᗩᖆᗩPas encore d'évaluation
- Drug Study SummaryDocument7 pagesDrug Study SummaryKateLayaogPas encore d'évaluation
- Case Study - Dengue Fever V - S UtiDocument12 pagesCase Study - Dengue Fever V - S UtiHarlene Joyce ReyPas encore d'évaluation
- Gestational DiabetesDocument3 pagesGestational DiabetesCortex Pluss0% (1)
- Module 12 ContempoDocument5 pagesModule 12 ContempoJericho CunananPas encore d'évaluation
- Nursing Care Plan for Hypertension ManagementDocument5 pagesNursing Care Plan for Hypertension Managementbhavana100% (1)
- Drug StudyDocument5 pagesDrug Studyjanelle123 toribioPas encore d'évaluation
- Drug StudyDocument2 pagesDrug StudyJanina Patricia BuddlePas encore d'évaluation
- VI. Laboratory ResultsDocument5 pagesVI. Laboratory ResultsCendaña LorelynPas encore d'évaluation
- PathophysiologyDocument9 pagesPathophysiologySuzette PipoPas encore d'évaluation
- Cholecystitis Litiasis EctomyDocument23 pagesCholecystitis Litiasis EctomyTimothy WilliamsPas encore d'évaluation
- Physician's Orders for Admission and Treatment of Epigastric PainDocument4 pagesPhysician's Orders for Admission and Treatment of Epigastric PainJerremy LuquePas encore d'évaluation
- Vaginal CancerDocument11 pagesVaginal CancerAiko TokunagaPas encore d'évaluation
- Generic Name & Brand Name Mechanism of Action Indications and Drug Rationale Contraindications Common Side Effects Nursing ConsiderationsDocument2 pagesGeneric Name & Brand Name Mechanism of Action Indications and Drug Rationale Contraindications Common Side Effects Nursing ConsiderationsMary Shine GonidaPas encore d'évaluation
- Ambulatoty CareDocument18 pagesAmbulatoty CareVhince PiscoPas encore d'évaluation
- Care of The Mother, Child and Adolescent (Well Client) Related Learning ExperienceDocument7 pagesCare of The Mother, Child and Adolescent (Well Client) Related Learning ExperienceIvy VillalobosPas encore d'évaluation
- Pathophysiology Cholelithiasis 2Document2 pagesPathophysiology Cholelithiasis 2Jamie HaravataPas encore d'évaluation
- Ethical Principles for StewardsDocument7 pagesEthical Principles for StewardsElla EllaPas encore d'évaluation
- TAHBSO ReportDocument4 pagesTAHBSO ReportsachiiMePas encore d'évaluation
- Ovarian New GrowthDocument1 pageOvarian New GrowthZhy CaluzaPas encore d'évaluation
- RLE 109 Group 4 Case Analysis in MastitisDocument20 pagesRLE 109 Group 4 Case Analysis in MastitisEugene MananganPas encore d'évaluation
- PANCREATIC CANCER NURSING CAREDocument71 pagesPANCREATIC CANCER NURSING CAREMavy CantonPas encore d'évaluation
- Group-5 NCM-107 NCPDocument4 pagesGroup-5 NCM-107 NCPbulok netflakes100% (1)
- Bladder Cancer Types, Symptoms, Tests & TreatmentDocument1 pageBladder Cancer Types, Symptoms, Tests & TreatmentCarmina AguilarPas encore d'évaluation
- Final Case StudyDocument18 pagesFinal Case Studyapi-487702467100% (1)
- Casestudy Makato 2nd Pre EclampsiaDocument7 pagesCasestudy Makato 2nd Pre EclampsiaRainier IbarretaPas encore d'évaluation
- Drug StudyDocument8 pagesDrug StudyzenPas encore d'évaluation
- Acute Cholecystitis SeminarDocument42 pagesAcute Cholecystitis SeminarNatnaelPas encore d'évaluation
- I.intrODUCTION Hypertension (High Blood Pressure) Is ADocument19 pagesI.intrODUCTION Hypertension (High Blood Pressure) Is Aoril04Pas encore d'évaluation
- Bacillary DysenteryDocument32 pagesBacillary Dysenteryapi-199163990% (1)
- Lovastatin Drug GuideDocument2 pagesLovastatin Drug GuideAngel CatalanPas encore d'évaluation
- Procreative Health Is The Moral Obligation of Parents To Have The Healthiest Children Through All Natural and Artificial Means AvailableDocument9 pagesProcreative Health Is The Moral Obligation of Parents To Have The Healthiest Children Through All Natural and Artificial Means AvailableShiela Mae GalisaPas encore d'évaluation
- Grand Case PresentationDocument50 pagesGrand Case PresentationJean Michelle100% (1)
- Drug StudyDocument10 pagesDrug Studyjho_26100% (2)
- Tetracycline Drug StudyDocument5 pagesTetracycline Drug StudyEmagra AzilPas encore d'évaluation
- Liver CancerDocument1 pageLiver CancerTarantado67% (3)
- Hypertensive UrgencyDocument8 pagesHypertensive UrgencyTony A.Pas encore d'évaluation
- Amoxicillin Nursing ConsiderationsDocument3 pagesAmoxicillin Nursing ConsiderationsNico DonatoPas encore d'évaluation
- Soapie, Assessment and NCP On PAINDocument7 pagesSoapie, Assessment and NCP On PAINAna100% (2)
- Management of Tuberculosis: A guide for clinicians (eBook edition)D'EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Pas encore d'évaluation
- UROLITHIASISDocument84 pagesUROLITHIASISJheanAlphonsineT.MeansPas encore d'évaluation
- New Case Study Group 4Document9 pagesNew Case Study Group 4chankatrina011Pas encore d'évaluation
- Nephrolithiasis CPDocument54 pagesNephrolithiasis CPSheena VallesPas encore d'évaluation
- Assignment 1.2Document1 pageAssignment 1.2Jhean MeansPas encore d'évaluation
- Mathematical WorksheetDocument1 pageMathematical WorksheetJhean MeansPas encore d'évaluation
- DifferenceofTwoCubes Worksheet 3Document1 pageDifferenceofTwoCubes Worksheet 3Jhean MeansPas encore d'évaluation
- Student report card templateDocument1 pageStudent report card templateJhean MeansPas encore d'évaluation
- Anaphylactic Shock NCLEX ReviewDocument4 pagesAnaphylactic Shock NCLEX ReviewJhean MeansPas encore d'évaluation
- Name: Date: Grade/Section: ScoreDocument1 pageName: Date: Grade/Section: ScoreJhean MeansPas encore d'évaluation
- Student report card summaryDocument1 pageStudent report card summaryJhean MeansPas encore d'évaluation
- Acute Kidney Injury NCLEX ReviewDocument5 pagesAcute Kidney Injury NCLEX ReviewJhean Means100% (1)
- Acute Glomerulonephritis Poststreptococcal NCLEX ReviewDocument4 pagesAcute Glomerulonephritis Poststreptococcal NCLEX ReviewJhean MeansPas encore d'évaluation
- Nursing-Care-Plan WorksheetDocument2 pagesNursing-Care-Plan WorksheetJhean MeansPas encore d'évaluation
- Digestion in Stomach and Intestines Grade 4Document24 pagesDigestion in Stomach and Intestines Grade 4jaydalene saga macay100% (1)
- Your Amazing Body Level 6 PDFDocument30 pagesYour Amazing Body Level 6 PDFmiltrans100% (1)
- Pituitary Blok Endokrin 2019Document40 pagesPituitary Blok Endokrin 2019ratihPas encore d'évaluation
- Anatomy and Physiology of The Male and Female Reproductive System Female Reproductive Anatomy and PhysiologyDocument6 pagesAnatomy and Physiology of The Male and Female Reproductive System Female Reproductive Anatomy and PhysiologyJustJ ThingsPas encore d'évaluation
- Dr. Asif Mian Ansari DNB Resident Dept. of General Surgery Max Hospital, MohaliDocument25 pagesDr. Asif Mian Ansari DNB Resident Dept. of General Surgery Max Hospital, MohaliKarem Maali100% (1)
- 2018 Dental Fee Guide PDFDocument1 page2018 Dental Fee Guide PDFLarryPas encore d'évaluation
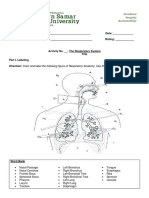
- The Respiratory System ActivityDocument4 pagesThe Respiratory System ActivityVina DiscarPas encore d'évaluation
- Class II Division 2 MalocclusionDocument8 pagesClass II Division 2 MalocclusionIddi IddiPas encore d'évaluation
- MODULE 2 Disorders of The Pituitary GlandDocument24 pagesMODULE 2 Disorders of The Pituitary GlandLorraine GambitoPas encore d'évaluation
- Medical Terminology Blood Lymph SystemsDocument29 pagesMedical Terminology Blood Lymph Systemsapi-268199514100% (1)
- Rosenzweig, Bennet & Diamond Study - SummaryDocument2 pagesRosenzweig, Bennet & Diamond Study - SummaryThhu BhoPas encore d'évaluation
- Absen Pembacaan Refarat Dan Lapsus Suci RamadhaniDocument2 pagesAbsen Pembacaan Refarat Dan Lapsus Suci Ramadhanisuci ramadhaniPas encore d'évaluation
- Pengaruh Glutathione Terhadap Kualitas Semen Kambing Boer Post Thawing Dalam Pengencer Yang Mengandung DimetylsulfoxidE DMSODocument12 pagesPengaruh Glutathione Terhadap Kualitas Semen Kambing Boer Post Thawing Dalam Pengencer Yang Mengandung DimetylsulfoxidE DMSOJaka ShankalyanaPas encore d'évaluation
- Alek Gilley - Student - HeritageHS - Personal Narrative FINAL (Due 10 - 13)Document3 pagesAlek Gilley - Student - HeritageHS - Personal Narrative FINAL (Due 10 - 13)AlekPas encore d'évaluation
- Topic 8 Endocrine SystemDocument2 pagesTopic 8 Endocrine SystemAnnie LiPas encore d'évaluation
- Osce AbdomenDocument33 pagesOsce AbdomenistiPas encore d'évaluation
- Secretory Functions of GITDocument24 pagesSecretory Functions of GITDr.Nusrat TariqPas encore d'évaluation
- Chronic Hyperplastic PulpitisDocument30 pagesChronic Hyperplastic PulpitisGlory Pohan67% (3)
- NERVOUS SYSTEM (IB-DP BIOLOGY) - Multiple Choice Type QuestionsDocument5 pagesNERVOUS SYSTEM (IB-DP BIOLOGY) - Multiple Choice Type QuestionsVishnu SharmaPas encore d'évaluation
- The Integumentary System NotesDocument3 pagesThe Integumentary System NotesJose Enrico SumayaPas encore d'évaluation
- DCM Medical Secretary - Glossary - Medical Terms PDFDocument71 pagesDCM Medical Secretary - Glossary - Medical Terms PDFEoin O'Byrne100% (1)
- BIT1012 Human-Anatomy-And-Physiology ETH 1 AC37Document2 pagesBIT1012 Human-Anatomy-And-Physiology ETH 1 AC37Vignesh AiyerPas encore d'évaluation
- Heterotrophic Nutrition Final 2018Document37 pagesHeterotrophic Nutrition Final 2018Otole dickensPas encore d'évaluation
- FRCR Part 1 - Radiological Anatomy - New For 2013 - Set 02 PDFDocument109 pagesFRCR Part 1 - Radiological Anatomy - New For 2013 - Set 02 PDFmohamed100% (3)
- Iyengar Yoga For The Respiratory System-2020 PDFDocument13 pagesIyengar Yoga For The Respiratory System-2020 PDFSlice LePas encore d'évaluation
- Residency 1000 QuestionDocument599 pagesResidency 1000 QuestionTan 57Pas encore d'évaluation
- Hormonal RegulationDocument20 pagesHormonal Regulationel shilohPas encore d'évaluation
- Test Bank For Dental Instruments A Pocket Guide 4th Edition Boyd DownloadDocument5 pagesTest Bank For Dental Instruments A Pocket Guide 4th Edition Boyd Downloadstevenjohnsondcnpxgskyi100% (23)
- Study of Histopathological Pattern of Thyroid Lesions: International Journal of Biomedical and Advance ResearchDocument10 pagesStudy of Histopathological Pattern of Thyroid Lesions: International Journal of Biomedical and Advance ResearchAprilia Fani PPas encore d'évaluation
- Arab Board Exam April 2015Document3 pagesArab Board Exam April 2015Firyal Balushi50% (4)