Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- 0001 CatDocument108 pages0001 CatJorge CabreraPas encore d'évaluation
- The Pentester BlueprintDocument27 pagesThe Pentester Blueprintjames smith100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- ADA Design Guide 2010Document7 pagesADA Design Guide 2010Jack BarkerPas encore d'évaluation
- ABS Part4 - Vessel Systems & Machinery - 2001Document710 pagesABS Part4 - Vessel Systems & Machinery - 2001AndréMenezesPas encore d'évaluation
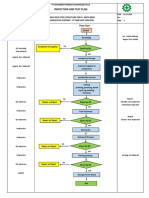
- Inspection and Test Plan: Flow Chart Start IncomingDocument1 pageInspection and Test Plan: Flow Chart Start IncomingSinden AyuPas encore d'évaluation
- DNV Rules For Electrical Instal at IonsDocument80 pagesDNV Rules For Electrical Instal at Ionsnzjohn100% (3)
- Self Ligating Brackets Smart Mechanics Article EcharriDocument12 pagesSelf Ligating Brackets Smart Mechanics Article EcharriOrtho OrganizersPas encore d'évaluation
- Torque Comparisons On 3d ModelsDocument6 pagesTorque Comparisons On 3d Modelsanon_768201406Pas encore d'évaluation
- Winter 2016Document88 pagesWinter 2016anon_768201406Pas encore d'évaluation
- Sarver PDFDocument8 pagesSarver PDFanon_768201406Pas encore d'évaluation
- Orofacialpain:: A PrimerDocument10 pagesOrofacialpain:: A Primeranon_768201406Pas encore d'évaluation
- 2013 Course Dates For Atlanta, Georgia : (G) Nathos Orthodontics 2013 The Clinical Modification of Dentofacial DevelopmentDocument6 pages2013 Course Dates For Atlanta, Georgia : (G) Nathos Orthodontics 2013 The Clinical Modification of Dentofacial Developmentanon_768201406Pas encore d'évaluation
- 3 Days Orthodontic Program For Denitsts Already Practicing Orthodontics. - DentistryUnitedDocument3 pages3 Days Orthodontic Program For Denitsts Already Practicing Orthodontics. - DentistryUnitedanon_768201406Pas encore d'évaluation
- Chapter5 PDFDocument23 pagesChapter5 PDFanon_768201406Pas encore d'évaluation
- 05 Chalet CDocument119 pages05 Chalet Canon_768201406Pas encore d'évaluation
- 3 Days Orthodontic Program For Denitsts Already Practicing Orthodontics. - DentistryUnitedDocument3 pages3 Days Orthodontic Program For Denitsts Already Practicing Orthodontics. - DentistryUnitedanon_768201406Pas encore d'évaluation
- Clinical StudyDocument6 pagesClinical Studyanon_768201406Pas encore d'évaluation
- 00 RWISO JOURNAL - Roth Williams International Society of PDFDocument61 pages00 RWISO JOURNAL - Roth Williams International Society of PDFanon_768201406Pas encore d'évaluation
- PK 010 Insulated Ceiling Construction With Wooden Flooring 1Document1 pagePK 010 Insulated Ceiling Construction With Wooden Flooring 1anon_768201406Pas encore d'évaluation
- 4th Annual 6E Meeting-Print2Document1 page4th Annual 6E Meeting-Print2anon_768201406Pas encore d'évaluation
- 00 RWISO JOURNAL - Roth Williams International Society of PDFDocument61 pages00 RWISO JOURNAL - Roth Williams International Society of PDFanon_768201406Pas encore d'évaluation
- 146b PDFDocument8 pages146b PDFanon_768201406Pas encore d'évaluation
- Rice Research: Open Access: Black Rice Cultivation and Forming Practices: Success Story of Indian FarmersDocument2 pagesRice Research: Open Access: Black Rice Cultivation and Forming Practices: Success Story of Indian Farmersapi-420356823Pas encore d'évaluation
- Schneider - Cptg010 en (Print)Document16 pagesSchneider - Cptg010 en (Print)el_koptan00857693Pas encore d'évaluation
- Informática Ejercicios IDocument10 pagesInformática Ejercicios IAlejandroMendezPas encore d'évaluation
- Grade 9 P.EDocument16 pagesGrade 9 P.EBrige SimeonPas encore d'évaluation
- Test Units and Accessories: Sinteso™Document22 pagesTest Units and Accessories: Sinteso™Imad QsnPas encore d'évaluation
- Lab 9-Measurement of Filtrate Loss and Mud Cake Thickness of Drilling Mud Sample Using Dead Weight Hydraulic Filter Press Considering API Standard.Document17 pagesLab 9-Measurement of Filtrate Loss and Mud Cake Thickness of Drilling Mud Sample Using Dead Weight Hydraulic Filter Press Considering API Standard.Sunny BbaPas encore d'évaluation
- Indian Boyhood PDFDocument316 pagesIndian Boyhood PDFHasanPas encore d'évaluation
- Refresher 2 (Pipe)Document12 pagesRefresher 2 (Pipe)Kira YagamiPas encore d'évaluation
- Personal Chiller 6-Can Mini Refrigerator, Pink K4Document1 pagePersonal Chiller 6-Can Mini Refrigerator, Pink K4Keyla SierraPas encore d'évaluation
- TESC CRC Office & Gym Roof Exterior PaintingDocument6 pagesTESC CRC Office & Gym Roof Exterior PaintinghuasPas encore d'évaluation
- INFORSHT Produktkatalog en Web 03.22Document13 pagesINFORSHT Produktkatalog en Web 03.22lolPas encore d'évaluation
- 21 - Effective Pages: Beechcraft CorporationDocument166 pages21 - Effective Pages: Beechcraft CorporationCristian PugaPas encore d'évaluation
- 6V Plush Ride-On: Owner'S ManualDocument26 pages6V Plush Ride-On: Owner'S ManualVisas LaredoPas encore d'évaluation
- Duty Roster Class IV JulyDocument2 pagesDuty Roster Class IV JulyTayyab HassanPas encore d'évaluation
- Steroids ActivityDocument1 pageSteroids Activityfaqed ilzakiraPas encore d'évaluation
- EDSP Quantitative and Qualitative FormDocument2 pagesEDSP Quantitative and Qualitative FormTalal SultanPas encore d'évaluation
- Rise School of Accountancy Test 08Document5 pagesRise School of Accountancy Test 08iamneonkingPas encore d'évaluation
- Somali Guideline of InvestorsDocument9 pagesSomali Guideline of InvestorsABDULLAHI HAGAR FARAH HERSI STUDENTPas encore d'évaluation
- 220/132 KV Sub-Station Bhilai-3: Training Report ONDocument24 pages220/132 KV Sub-Station Bhilai-3: Training Report ONKalyani ShuklaPas encore d'évaluation
- Lecture 1 Biochem 232 CellsDocument13 pagesLecture 1 Biochem 232 CellsaelmowafyPas encore d'évaluation
- Class9. CVD and PVDDocument30 pagesClass9. CVD and PVDiraPas encore d'évaluation
- Density of Aggregates: ObjectivesDocument4 pagesDensity of Aggregates: ObjectivesKit Gerald EliasPas encore d'évaluation
- Understanding Anxiety Disorders and Abnormal PsychologyDocument7 pagesUnderstanding Anxiety Disorders and Abnormal PsychologyLeonardo YsaiahPas encore d'évaluation
- Evolution Chart 3Document1 pageEvolution Chart 3sasupraPas encore d'évaluation