Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Angiography Basics and Seldinger TechniqueDocument33 pagesAngiography Basics and Seldinger TechniqueTsz Him James WongPas encore d'évaluation
- About Lung Cancer: Overview and TypesDocument13 pagesAbout Lung Cancer: Overview and TypesGordana PuzovicPas encore d'évaluation
- Computed Tomography in The Diagnosis of Subcapsular and Perirenal HematomaDocument6 pagesComputed Tomography in The Diagnosis of Subcapsular and Perirenal HematomaGordana PuzovicPas encore d'évaluation
- Risk Adjustment Coding PDFDocument38 pagesRisk Adjustment Coding PDFGordana Puzovic100% (2)
- Primary Tracheal Tumors: Review of 37 CasesDocument4 pagesPrimary Tracheal Tumors: Review of 37 CasesGordana PuzovicPas encore d'évaluation
- PIIS1556086416335158Document12 pagesPIIS1556086416335158Gordana PuzovicPas encore d'évaluation
- Recurrent Pyogenic Cholangitis: From Imaging To InterventionDocument8 pagesRecurrent Pyogenic Cholangitis: From Imaging To InterventionGordana PuzovicPas encore d'évaluation
- Prevalence of Solid Tumors in Incidentally Detected Homogeneous Renal Masses Measuring 20 HU On Portal Venous Phase CTDocument5 pagesPrevalence of Solid Tumors in Incidentally Detected Homogeneous Renal Masses Measuring 20 HU On Portal Venous Phase CTGordana PuzovicPas encore d'évaluation
- InTech-Advances Bone MetastasesDocument16 pagesInTech-Advances Bone MetastasesGordana PuzovicPas encore d'évaluation
- Transient Hepatic Perfusion Differences (THAD/THID) - What? When? Where?Document35 pagesTransient Hepatic Perfusion Differences (THAD/THID) - What? When? Where?Gordana PuzovicPas encore d'évaluation
- Sjogren's Syndrome, Vasculitis, and Cryoglobulinaemia Associated With (Kappa) Paraprotein With Rheumatoid ActivityDocument3 pagesSjogren's Syndrome, Vasculitis, and Cryoglobulinaemia Associated With (Kappa) Paraprotein With Rheumatoid ActivityGordana PuzovicPas encore d'évaluation
- Review On Pancreatic Steatosis Detection by Imaging ModalitiesDocument10 pagesReview On Pancreatic Steatosis Detection by Imaging ModalitiesGordana PuzovicPas encore d'évaluation
- 01 Cir 9 1 1Document16 pages01 Cir 9 1 1Gordana PuzovicPas encore d'évaluation
- Infection and Immunity-1971-Eudy-269.fullDocument5 pagesInfection and Immunity-1971-Eudy-269.fullGordana PuzovicPas encore d'évaluation
- Imaging in Acute Renal Infection: BJU International (2000), 86 Suppl. 1, 70 79Document10 pagesImaging in Acute Renal Infection: BJU International (2000), 86 Suppl. 1, 70 79Gordana PuzovicPas encore d'évaluation
- Role of Triple Phase Computed Tomography Findings For Evaluation of Hepatic LesionsDocument8 pagesRole of Triple Phase Computed Tomography Findings For Evaluation of Hepatic LesionsGordana PuzovicPas encore d'évaluation
- Spontaneous Ruptured Intercostal and Lumber Artery in Type 1 NeurofibromatosisDocument15 pagesSpontaneous Ruptured Intercostal and Lumber Artery in Type 1 NeurofibromatosisGordana PuzovicPas encore d'évaluation
- Early Onset Pneumonia Following Pulmonary Contusion: The Case of Stonewall JacksonDocument3 pagesEarly Onset Pneumonia Following Pulmonary Contusion: The Case of Stonewall JacksonGordana PuzovicPas encore d'évaluation
- Primary Aortoduodenal Fistula Caused by Aortitis: SalmonellaDocument4 pagesPrimary Aortoduodenal Fistula Caused by Aortitis: SalmonellaGordana PuzovicPas encore d'évaluation
- PIIS1201971220301016Document6 pagesPIIS1201971220301016Gordana PuzovicPas encore d'évaluation
- Focal Confluent Fibrosis in Cirrhotic Liver: Natural History Studied With Serial CTDocument7 pagesFocal Confluent Fibrosis in Cirrhotic Liver: Natural History Studied With Serial CTGordana PuzovicPas encore d'évaluation
- Intercostal Artery Injury Manifested by A Sentinel Pleural ClotDocument2 pagesIntercostal Artery Injury Manifested by A Sentinel Pleural ClotGordana PuzovicPas encore d'évaluation
- Organizing Pneumonia: The Many Morphological Faces: European Radiology July 2002Document12 pagesOrganizing Pneumonia: The Many Morphological Faces: European Radiology July 2002Gordana PuzovicPas encore d'évaluation
- Ajr 07 2491Document6 pagesAjr 07 2491Khalvia KhairinPas encore d'évaluation
- Glossopharyngeal NeuralgiaDocument36 pagesGlossopharyngeal NeuralgiaGeetha SoundaryaPas encore d'évaluation
- 118 Skills Lab-Week 1-Responses To Altered Ventilatory FunctionsDocument8 pages118 Skills Lab-Week 1-Responses To Altered Ventilatory FunctionsKeisha BartolataPas encore d'évaluation
- ROTABLATORDocument20 pagesROTABLATORArtemisPas encore d'évaluation
- QuickCat BrochureDocument3 pagesQuickCat Brochurebiomedical_com_brPas encore d'évaluation
- Fluorescein AngiographyDocument81 pagesFluorescein Angiographyeng_25122147100% (4)
- Vascular Note by Joel ArudchelvamDocument52 pagesVascular Note by Joel ArudchelvamJoel Arudchelvam100% (1)
- ERS-Imaging BodyDocument280 pagesERS-Imaging BodyOctavian Andrei MaliiaPas encore d'évaluation
- Emergency Radiology: The BasicsDocument68 pagesEmergency Radiology: The BasicsArya Vandy Eka PradanaPas encore d'évaluation
- Lesson Plan On Cerebro Vascular Accident 1Document13 pagesLesson Plan On Cerebro Vascular Accident 1simonjosan67% (3)
- Case Study For Acute Coronary SyndromeDocument7 pagesCase Study For Acute Coronary SyndromeGabbii CincoPas encore d'évaluation
- ch3 1Document15 pagesch3 1Harshit SinghPas encore d'évaluation
- Pulmonary EmbolismDocument20 pagesPulmonary Embolismdyah sekar ayuPas encore d'évaluation
- Chapter 16 - Dyes - 2008 - Clinical Ocular PharmacologyDocument12 pagesChapter 16 - Dyes - 2008 - Clinical Ocular PharmacologysPas encore d'évaluation
- Uterine Arteriovenous Malformation: Hilwati H, Ouzreiah NDocument5 pagesUterine Arteriovenous Malformation: Hilwati H, Ouzreiah NM Iqbal EffendiPas encore d'évaluation
- Resume of MonirDocument6 pagesResume of Monirmhossaink8856Pas encore d'évaluation
- DRT I & II Year SyllabusDocument11 pagesDRT I & II Year SyllabusSÚPÈR ÑØVÅ100% (1)
- Journal Reading Radiologi EllaDocument44 pagesJournal Reading Radiologi EllaElla Putri SaptariPas encore d'évaluation
- Computer Methods and Programs in Biomedicine: Xiliang Zhu, Zhaoyun Cheng, Sheng Wang, Xianjie Chen, Guoqing LuDocument8 pagesComputer Methods and Programs in Biomedicine: Xiliang Zhu, Zhaoyun Cheng, Sheng Wang, Xianjie Chen, Guoqing LuTuan PhanPas encore d'évaluation
- Faustin Kabwe and Another V The PeopleDocument9 pagesFaustin Kabwe and Another V The Peopletalk2marvin70Pas encore d'évaluation
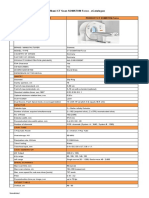
- Spesifikasi CT SOMATOM ForceDocument2 pagesSpesifikasi CT SOMATOM ForceYohanes Riung100% (1)
- Assessment of NeurologyDocument33 pagesAssessment of NeurologyDR. KUMARASWAMI HEALTH CENTRE COLLEGE OF NURSING KANYAKUMARIPas encore d'évaluation
- Buerger's DiseaseDocument4 pagesBuerger's DiseaseCharles Avevrahamme M. AmlogPas encore d'évaluation
- RadiologyDocument54 pagesRadiologyDark LordPas encore d'évaluation
- Extracranial Carotid Artery Aneurysm - UpToDateDocument25 pagesExtracranial Carotid Artery Aneurysm - UpToDateDiego RodriguesPas encore d'évaluation
- Scalamogna Et Al. 2022 - CRM - IsAR-CALC-2 DesignDocument6 pagesScalamogna Et Al. 2022 - CRM - IsAR-CALC-2 DesignPraveenVeeraPas encore d'évaluation
- Brochure Optima IGS 330 2016Document7 pagesBrochure Optima IGS 330 2016Mauricio Ernesto Andrade MaquilónPas encore d'évaluation
- Neurological AssessmentDocument82 pagesNeurological AssessmentSan Shine100% (1)
- ALL May 2018 RecallsDocument168 pagesALL May 2018 RecallsSaja Hussein95100% (2)