Vous aimerez peut-être aussi
- US and CT Findings in The Diagnosis of Tuberculous PeritonitisDocument5 pagesUS and CT Findings in The Diagnosis of Tuberculous PeritonitisGordana PuzovicPas encore d'évaluation
- Metanephric Adenoma in An 8-Year-Old Child: Case Report and Review of The LiteratureDocument4 pagesMetanephric Adenoma in An 8-Year-Old Child: Case Report and Review of The LiteratureNGUYEN QUYNHPas encore d'évaluation
- HydronephrosisDocument3 pagesHydronephrosisCarla AlmerolPas encore d'évaluation
- Testicular TorsionDocument9 pagesTesticular TorsionSyedKashifAliPas encore d'évaluation
- Canine InsulinomaDocument5 pagesCanine Insulinomasoff4ikaPas encore d'évaluation
- Laparoscopic Excision of A Renal Subcapsular Abscess Presenting As A Subcapsular HaematomaDocument3 pagesLaparoscopic Excision of A Renal Subcapsular Abscess Presenting As A Subcapsular HaematomaDavid MorgPas encore d'évaluation
- Journal 2Document3 pagesJournal 2Wahyu Pranata PardedePas encore d'évaluation
- Is Surveillance Necessary For Inverted Papilloma in The Urinary Bladder and Urethra?Document5 pagesIs Surveillance Necessary For Inverted Papilloma in The Urinary Bladder and Urethra?Денис КрахоткинPas encore d'évaluation
- Urology Case Reports: OncologyDocument3 pagesUrology Case Reports: OncologyDavids MarinPas encore d'évaluation
- Rare Cases of ChylothoraxDocument5 pagesRare Cases of ChylothoraxdrAlbertoVVPas encore d'évaluation
- Abdominopelvic Ectopic Spleen With A Comprehensive Imaging Examination: A Case ReportDocument6 pagesAbdominopelvic Ectopic Spleen With A Comprehensive Imaging Examination: A Case ReportceciliaPas encore d'évaluation
- Xanthogranulomatous Pyelonephritis: Radiologic Review.: Poster No.: Congress: Type: AuthorsDocument17 pagesXanthogranulomatous Pyelonephritis: Radiologic Review.: Poster No.: Congress: Type: AuthorsChavdarPas encore d'évaluation
- Suciu 2017Document3 pagesSuciu 2017Teja Laksana NukanaPas encore d'évaluation
- Subsidence of Hypertension in A Patient With GiantDocument4 pagesSubsidence of Hypertension in A Patient With GiantSinbijeo GinPas encore d'évaluation
- Rui 2007Document5 pagesRui 2007Radiologi RSPDPas encore d'évaluation
- The Peculiar Appearance of A Developing Pyog - 2013 - Journal of Pediatric SurgeDocument2 pagesThe Peculiar Appearance of A Developing Pyog - 2013 - Journal of Pediatric SurgeGunduz AgaPas encore d'évaluation
- Synchronous Renal Cancers: Case Report of TCC and PRCCDocument3 pagesSynchronous Renal Cancers: Case Report of TCC and PRCCDewa Made Sucipta PutraPas encore d'évaluation
- Mass Lesions in The Transplanted Kidney: Questions: Clinical QuizDocument2 pagesMass Lesions in The Transplanted Kidney: Questions: Clinical QuizSAhand HamzaPas encore d'évaluation
- Primary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportDocument6 pagesPrimary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportRais KhairuddinPas encore d'évaluation
- Beyond The Boundaries: Enigma of Distinguishing Exophytic Upper Pole Renal Cell Carcinoma From An Adrenal MassDocument4 pagesBeyond The Boundaries: Enigma of Distinguishing Exophytic Upper Pole Renal Cell Carcinoma From An Adrenal MassAyush JainPas encore d'évaluation
- Wunderlich Syndrome Spontaneous Atraumatic Rupture of The KidneyDocument5 pagesWunderlich Syndrome Spontaneous Atraumatic Rupture of The KidneyqalbiPas encore d'évaluation
- Prolonged Extreme Thrombocytosis in A Postsplenectomy Patient With Hereditary Spherocytosis PDFDocument6 pagesProlonged Extreme Thrombocytosis in A Postsplenectomy Patient With Hereditary Spherocytosis PDFSotir LakoPas encore d'évaluation
- C R Diagnosis, Treatment, and Long-Term Follow-Up of Bilateral, Upper Urinary Tract Infection (UTI) in A CatDocument8 pagesC R Diagnosis, Treatment, and Long-Term Follow-Up of Bilateral, Upper Urinary Tract Infection (UTI) in A CatguadasampaioPas encore d'évaluation
- Metastatic Spread of Primary Lung Adenocarcino - 2024 - International Journal ofDocument5 pagesMetastatic Spread of Primary Lung Adenocarcino - 2024 - International Journal ofRonald QuezadaPas encore d'évaluation
- Malignant Tumor Case Report in Horseshoe KidneyDocument3 pagesMalignant Tumor Case Report in Horseshoe KidneyNovita Elmy MufidaPas encore d'évaluation
- Obturator Hernia6Document3 pagesObturator Hernia6Ioana DumitraşcuPas encore d'évaluation
- 1 s2.0 S0929644112000057 MainDocument4 pages1 s2.0 S0929644112000057 MainAisahPas encore d'évaluation
- 10 TM Ca Celulas TransicionalesDocument19 pages10 TM Ca Celulas TransicionalesDonaldo ReleyPas encore d'évaluation
- Ijt 9 185Document5 pagesIjt 9 185Mia DangaPas encore d'évaluation
- CT YIELD FOR PELVIC IMAGINGDocument2 pagesCT YIELD FOR PELVIC IMAGINGSara CifuentesPas encore d'évaluation
- Custodio (1999)Document3 pagesCustodio (1999)Teodora TelecanPas encore d'évaluation
- Accepted Manuscript: World NeurosurgeryDocument17 pagesAccepted Manuscript: World NeurosurgeryAniydaPas encore d'évaluation
- Chung 2004Document4 pagesChung 2004raghad.bassalPas encore d'évaluation
- Cuaj 4 E60Document5 pagesCuaj 4 E60Irma Suriani DarwisPas encore d'évaluation
- Central Lucency of Pelvic Phleboliths - Comparison of Radiographs and Noncontrast Helical CTDocument4 pagesCentral Lucency of Pelvic Phleboliths - Comparison of Radiographs and Noncontrast Helical CTSara CifuentesPas encore d'évaluation
- Anatomo-Radioimaging Correlation in Atypical Ewing SarcomaDocument5 pagesAnatomo-Radioimaging Correlation in Atypical Ewing SarcomaIoana PelinPas encore d'évaluation
- Utility of Endoscopic Ultrasound in Symptomatic Cut Corners of A ClotDocument3 pagesUtility of Endoscopic Ultrasound in Symptomatic Cut Corners of A ClotDjabhi SpinzzPas encore d'évaluation
- 1987 Metastasis To The Larynx Revealing A Renal Cell CarcinomaDocument8 pages1987 Metastasis To The Larynx Revealing A Renal Cell CarcinomaAlfonsoSánchezPas encore d'évaluation
- Grade 4 Renal Injury: Current Trend of Management and Future DirectionsDocument3 pagesGrade 4 Renal Injury: Current Trend of Management and Future DirectionsputraPas encore d'évaluation
- Gross Hematuria of Uncommon Origin: The Nutcracker Syndrome: Case ReportDocument4 pagesGross Hematuria of Uncommon Origin: The Nutcracker Syndrome: Case ReportDiana AmpulembangPas encore d'évaluation
- A Rare Case of Chromophobe Renal Cell Carcinoma in A 55-Year-Old Female: A Case ReportDocument14 pagesA Rare Case of Chromophobe Renal Cell Carcinoma in A 55-Year-Old Female: A Case ReportdeborapkphnPas encore d'évaluation
- ArcuatoDocument7 pagesArcuatoDaniela PekePas encore d'évaluation
- Hepatolithiasis May Increase Risk of CholangiocarcinomaDocument4 pagesHepatolithiasis May Increase Risk of CholangiocarcinomaNurul RifqianiPas encore d'évaluation
- Gotto 2010Document3 pagesGotto 2010Wirda Elya SariPas encore d'évaluation
- Criem2015 868519Document4 pagesCriem2015 868519m.fahimsharifiPas encore d'évaluation
- La Importancia de La Urografía Por TC en El Diagnóstico Precoz de Variaciones Anatómicas Del Tracto Urogenital Presentación de CasoDocument5 pagesLa Importancia de La Urografía Por TC en El Diagnóstico Precoz de Variaciones Anatómicas Del Tracto Urogenital Presentación de Casojose luis ramirez espinosaPas encore d'évaluation
- Ultrasound Diagnosis: Phiwipha KamonratDocument3 pagesUltrasound Diagnosis: Phiwipha KamonratVanessa Hidalgo PincheiraPas encore d'évaluation
- Cancer - October 1976 - Fishkin - Cervical Lymph Node Metastasis As The First Manifestation of Localized ExtramedullaryDocument4 pagesCancer - October 1976 - Fishkin - Cervical Lymph Node Metastasis As The First Manifestation of Localized ExtramedullarymacklynmanuelPas encore d'évaluation
- An Infrequent Secondary Location of Renal Carcinoma About A CaseDocument7 pagesAn Infrequent Secondary Location of Renal Carcinoma About A CaseInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Dafpus LiverDocument2 pagesDafpus LiverMenda JangWooyoung SooyoungsterPas encore d'évaluation
- BRIEF CLINICAL OBSERVATIONS: Nondilated Obstructive Uropathy Due to a Ureteral CalculusDocument3 pagesBRIEF CLINICAL OBSERVATIONS: Nondilated Obstructive Uropathy Due to a Ureteral CalculusMuhammad Kholid FirdausPas encore d'évaluation
- Sang 2011Document8 pagesSang 2011Vlad IchimPas encore d'évaluation
- 2 5400160637227631067 PDFDocument7 pages2 5400160637227631067 PDFSiska HarapanPas encore d'évaluation
- 2016-Clin Nucl Med-Hu-4176787Document3 pages2016-Clin Nucl Med-Hu-4176787LH HuPas encore d'évaluation
- Spinal Epidural Abscess in Two CalvesDocument8 pagesSpinal Epidural Abscess in Two CalvesRachel AutranPas encore d'évaluation
- Mi TsuyamaDocument8 pagesMi TsuyamatnsourcePas encore d'évaluation
- Differentiating Appendicitis from Shunt Infection in Pediatric Patients with Ventriculo-Peritoneal ShuntsDocument4 pagesDifferentiating Appendicitis from Shunt Infection in Pediatric Patients with Ventriculo-Peritoneal ShuntsAngel OlartePas encore d'évaluation
- ChangDocument3 pagesChangAmirullah AbdiPas encore d'évaluation
- 175 700 1 PBDocument2 pages175 700 1 PBEva ParamithaPas encore d'évaluation
- Contrast-Enhanced Ultrasound Imaging of Hepatic NeoplasmsD'EverandContrast-Enhanced Ultrasound Imaging of Hepatic NeoplasmsWen-Ping WangPas encore d'évaluation
- Primary Tracheal Tumors: Review of 37 CasesDocument4 pagesPrimary Tracheal Tumors: Review of 37 CasesGordana PuzovicPas encore d'évaluation
- Gross Anatomy and Cell Biology of The Lower Urinary Tract: Committee 1Document66 pagesGross Anatomy and Cell Biology of The Lower Urinary Tract: Committee 1Gordana PuzovicPas encore d'évaluation
- The Spleen1Document49 pagesThe Spleen1786waqar786Pas encore d'évaluation
- Renal Cell CarcinomaDocument70 pagesRenal Cell CarcinomaIsabel ReyPas encore d'évaluation
- Prevalence of Solid Tumors in Incidentally Detected Homogeneous Renal Masses Measuring 20 HU On Portal Venous Phase CTDocument5 pagesPrevalence of Solid Tumors in Incidentally Detected Homogeneous Renal Masses Measuring 20 HU On Portal Venous Phase CTGordana PuzovicPas encore d'évaluation
- PIIS1556086416335158Document12 pagesPIIS1556086416335158Gordana PuzovicPas encore d'évaluation
- Computed Tomography in The Diagnosis of Subcapsular and Perirenal HematomaDocument6 pagesComputed Tomography in The Diagnosis of Subcapsular and Perirenal HematomaGordana PuzovicPas encore d'évaluation
- Risk Adjustment Coding PDFDocument38 pagesRisk Adjustment Coding PDFGordana Puzovic100% (1)
- Ho0113 Wu1Document6 pagesHo0113 Wu1Gordana PuzovicPas encore d'évaluation
- About Lung Cancer: Overview and TypesDocument13 pagesAbout Lung Cancer: Overview and TypesGordana PuzovicPas encore d'évaluation
- 1240approach To Pulmonary Nodules - 4Document18 pages1240approach To Pulmonary Nodules - 4Gordana PuzovicPas encore d'évaluation
- InTech-Advances Bone MetastasesDocument16 pagesInTech-Advances Bone MetastasesGordana PuzovicPas encore d'évaluation
- Accuracy of Computed Tomography in Small Bowel ObstructionDocument3 pagesAccuracy of Computed Tomography in Small Bowel ObstructionGordana PuzovicPas encore d'évaluation
- Transient Hepatic Perfusion Differences (THAD/THID) - What? When? Where?Document35 pagesTransient Hepatic Perfusion Differences (THAD/THID) - What? When? Where?Gordana PuzovicPas encore d'évaluation
- Recurrent Pyogenic Cholangitis: From Imaging To InterventionDocument8 pagesRecurrent Pyogenic Cholangitis: From Imaging To InterventionGordana PuzovicPas encore d'évaluation
- Spontaneous Ruptured Intercostal and Lumber Artery in Type 1 NeurofibromatosisDocument15 pagesSpontaneous Ruptured Intercostal and Lumber Artery in Type 1 NeurofibromatosisGordana PuzovicPas encore d'évaluation
- Early Onset Pneumonia Likely Caused Stonewall Jackson's DeathDocument3 pagesEarly Onset Pneumonia Likely Caused Stonewall Jackson's DeathGordana PuzovicPas encore d'évaluation
- Sjogren's Syndrome, Vasculitis, and Cryoglobulinaemia Associated With (Kappa) Paraprotein With Rheumatoid ActivityDocument3 pagesSjogren's Syndrome, Vasculitis, and Cryoglobulinaemia Associated With (Kappa) Paraprotein With Rheumatoid ActivityGordana PuzovicPas encore d'évaluation
- Review On Pancreatic Steatosis Detection by Imaging ModalitiesDocument10 pagesReview On Pancreatic Steatosis Detection by Imaging ModalitiesGordana PuzovicPas encore d'évaluation
- Infection and Immunity-1971-Eudy-269.fullDocument5 pagesInfection and Immunity-1971-Eudy-269.fullGordana PuzovicPas encore d'évaluation
- Acute Pancreatitis With Normal Amylase and LipaseDocument1 pageAcute Pancreatitis With Normal Amylase and LipaseGordana PuzovicPas encore d'évaluation
- Imaging in Acute Renal Infection: BJU International (2000), 86 Suppl. 1, 70 79Document10 pagesImaging in Acute Renal Infection: BJU International (2000), 86 Suppl. 1, 70 79Gordana PuzovicPas encore d'évaluation
- Guidance on Evaluating and Treating UTIs and ASBDocument14 pagesGuidance on Evaluating and Treating UTIs and ASBJohn Vincent Dy OcampoPas encore d'évaluation
- Early Onset Pneumonia Likely Caused Stonewall Jackson's DeathDocument3 pagesEarly Onset Pneumonia Likely Caused Stonewall Jackson's DeathGordana PuzovicPas encore d'évaluation
- Journal of Acute Disease: Study On The Relationship of Acute Ketosis Intoxication and Type 2 Diabetes MellitusDocument5 pagesJournal of Acute Disease: Study On The Relationship of Acute Ketosis Intoxication and Type 2 Diabetes MellitusGordana PuzovicPas encore d'évaluation
- Imaging in Acute Renal Infection: BJU International (2000), 86 Suppl. 1, 70 79Document10 pagesImaging in Acute Renal Infection: BJU International (2000), 86 Suppl. 1, 70 79Gordana PuzovicPas encore d'évaluation
- Role of Triple Phase Computed Tomography Findings For Evaluation of Hepatic LesionsDocument8 pagesRole of Triple Phase Computed Tomography Findings For Evaluation of Hepatic LesionsGordana PuzovicPas encore d'évaluation
- The Role of HRCT in Post-Traumatic Hypoxemia: Poster No.: Congress: Type: AuthorsDocument51 pagesThe Role of HRCT in Post-Traumatic Hypoxemia: Poster No.: Congress: Type: AuthorsGordana PuzovicPas encore d'évaluation
- PIIS000349751101188XDocument7 pagesPIIS000349751101188XGordana PuzovicPas encore d'évaluation
- Supreme Court Rules on Retirement Benefits ComputationDocument5 pagesSupreme Court Rules on Retirement Benefits Computationemman2g.2baccay100% (1)
- Diagnosis of Dieback Disease of The Nutmeg Tree in Aceh Selatan, IndonesiaDocument10 pagesDiagnosis of Dieback Disease of The Nutmeg Tree in Aceh Selatan, IndonesiaciptaPas encore d'évaluation
- Consolidation of AccountsDocument14 pagesConsolidation of Accountsram_alaways0% (1)
- Effectiveness of Laundry Detergents and Bars in Removing Common StainsDocument9 pagesEffectiveness of Laundry Detergents and Bars in Removing Common StainsCloudy ClaudPas encore d'évaluation
- Basic Principles of Social Stratification - Sociology 11 - A SY 2009-10Document9 pagesBasic Principles of Social Stratification - Sociology 11 - A SY 2009-10Ryan Shimojima67% (3)
- Reading and Writing Skills: Quarter 4 - Module 1Document16 pagesReading and Writing Skills: Quarter 4 - Module 1Ericka Marie AlmadoPas encore d'évaluation
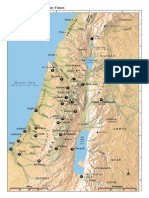
- Israel Bible MapDocument1 pageIsrael Bible MapMoses_JakkalaPas encore d'évaluation
- Class 9 Maths Olympiad Achievers Previous Years Papers With SolutionsDocument7 pagesClass 9 Maths Olympiad Achievers Previous Years Papers With Solutionskj100% (2)
- KARTONAN PRODUkDocument30 pagesKARTONAN PRODUkAde SeprialdiPas encore d'évaluation
- Philippine Association of Service Exporters vs Drilon Guidelines on Deployment BanDocument1 pagePhilippine Association of Service Exporters vs Drilon Guidelines on Deployment BanRhev Xandra AcuñaPas encore d'évaluation
- Life Pre-Intermediate Writing Worksheet Units 3&4Document4 pagesLife Pre-Intermediate Writing Worksheet Units 3&4SabrinaPas encore d'évaluation
- ACCOUNTING FOR SPECIAL EDUCATION FUNDSDocument12 pagesACCOUNTING FOR SPECIAL EDUCATION FUNDSIrdo KwanPas encore d'évaluation
- Case Study - Succession LawDocument2 pagesCase Study - Succession LawpablopoparamartinPas encore d'évaluation
- BSD ReviewerDocument17 pagesBSD ReviewerMagelle AgbalogPas encore d'évaluation
- Data Processing & Hosting Services in The US Industry Report PDFDocument34 pagesData Processing & Hosting Services in The US Industry Report PDFimobiwan4711Pas encore d'évaluation
- Relay Models Per Types Mdp38 EnuDocument618 pagesRelay Models Per Types Mdp38 Enuazer NadingaPas encore d'évaluation
- Miriam Garcia Resume 2 1Document2 pagesMiriam Garcia Resume 2 1api-548501562Pas encore d'évaluation
- HLT42707 Certificate IV in Aromatherapy: Packaging RulesDocument2 pagesHLT42707 Certificate IV in Aromatherapy: Packaging RulesNilamdeen Mohamed ZamilPas encore d'évaluation
- Adjusted School Reading Program of Buneg EsDocument7 pagesAdjusted School Reading Program of Buneg EsGener Taña AntonioPas encore d'évaluation
- BrianmayDocument4 pagesBrianmayapi-284933758Pas encore d'évaluation
- Infinitive Clauses PDFDocument3 pagesInfinitive Clauses PDFKatia LeliakhPas encore d'évaluation
- Feminism in Lucia SartoriDocument41 pagesFeminism in Lucia SartoriRaraPas encore d'évaluation
- Alsa Alsatom MB, MC - Service ManualDocument26 pagesAlsa Alsatom MB, MC - Service ManualJoão Francisco MontanhaniPas encore d'évaluation
- Whois contact details list with domainsDocument35 pagesWhois contact details list with domainsPrakash NPas encore d'évaluation
- Business Data Communications and Networking 13Th Edition Fitzgerald Test Bank Full Chapter PDFDocument40 pagesBusiness Data Communications and Networking 13Th Edition Fitzgerald Test Bank Full Chapter PDFthrongweightypfr100% (12)
- Strategic Planning and Program Budgeting in Romania RecentDocument6 pagesStrategic Planning and Program Budgeting in Romania RecentCarmina Ioana TomariuPas encore d'évaluation
- Torts and DamagesDocument63 pagesTorts and DamagesStevensonYuPas encore d'évaluation
- Industrial and Organizational PsychologyDocument21 pagesIndustrial and Organizational PsychologyCris Ben Bardoquillo100% (1)
- Aldecoa v. Insular GovtDocument1 pageAldecoa v. Insular Govtowenalan buenaventuraPas encore d'évaluation
- Bajaj Allianz General Insurance Company LimitedDocument9 pagesBajaj Allianz General Insurance Company LimitedNaresh ChanchadPas encore d'évaluation