Vous aimerez peut-être aussi
- 2021 - Elbokl - Severe Caffeine Intoxication Treated With HemodialysisDocument4 pages2021 - Elbokl - Severe Caffeine Intoxication Treated With Hemodialysisamanda lssPas encore d'évaluation
- Trauma EGS MEGA Electrolyte ProtocolDocument4 pagesTrauma EGS MEGA Electrolyte ProtocolKevin Mathews TharakanPas encore d'évaluation
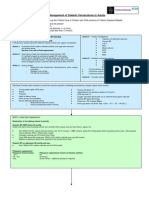
- How Is Hypokalaemia Treated in Adults?: Medicines Q&AsDocument6 pagesHow Is Hypokalaemia Treated in Adults?: Medicines Q&AsNotForAbusePas encore d'évaluation
- Hyperkalaemia FormularyDocument3 pagesHyperkalaemia FormularyMiguel SanJuanPas encore d'évaluation
- Potassium Chloride GuidelinesDocument25 pagesPotassium Chloride GuidelinesYasser Gebril86% (7)
- Journal of Translational Medicine: Practical Aspects in The Management of Hypokalemic Periodic ParalysisDocument8 pagesJournal of Translational Medicine: Practical Aspects in The Management of Hypokalemic Periodic ParalysisAndi Besse Ummu AmalyahPas encore d'évaluation
- Acute Hyperkalaemia in AdultsDocument12 pagesAcute Hyperkalaemia in AdultsMeilina FitrianiPas encore d'évaluation
- Hemodialysis Treatment in Patients With Severe Electrolyte DisordersDocument8 pagesHemodialysis Treatment in Patients With Severe Electrolyte DisordersRESIDENTES MEDICINA INTERNAPas encore d'évaluation
- Pass Critical Care Endocrine Frcem ResourcesDocument41 pagesPass Critical Care Endocrine Frcem ResourcesYoussef SaadPas encore d'évaluation
- Vidence FOR Management OF Hypokalemia IN THE ED CKD AND Dialysis PatientsDocument41 pagesVidence FOR Management OF Hypokalemia IN THE ED CKD AND Dialysis Patientsadri20121989Pas encore d'évaluation
- Clinical Nephrology and Renal Care: ClinmedDocument4 pagesClinical Nephrology and Renal Care: ClinmedkhorikPas encore d'évaluation
- The Influence of Blood Storage Time On The Potassium Level of Patients Receiving Packed Red Cell (PRC) Transfusion in Adam Malik General Hospital, MedanDocument6 pagesThe Influence of Blood Storage Time On The Potassium Level of Patients Receiving Packed Red Cell (PRC) Transfusion in Adam Malik General Hospital, MedanInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Guideline Fluido 2013Document11 pagesGuideline Fluido 2013larissa0semeaoPas encore d'évaluation
- Bmjopen 2016 March 6 3 Inline Supplementary Material 1Document2 pagesBmjopen 2016 March 6 3 Inline Supplementary Material 1thefuserPas encore d'évaluation
- Adult Diabetic Emergencies Care ProtocolDocument4 pagesAdult Diabetic Emergencies Care ProtocolvladhdPas encore d'évaluation
- Electrolyte ReplacementDocument5 pagesElectrolyte Replacementtwo.risk100% (1)
- Tumour Lysis SyndromeDocument15 pagesTumour Lysis SyndromeziggyshahdustPas encore d'évaluation
- Perioperative Fluid Therapy: Department of Anesthesiology &ICU KKUH. King Saud UniversityDocument47 pagesPerioperative Fluid Therapy: Department of Anesthesiology &ICU KKUH. King Saud Universityarifjo7999Pas encore d'évaluation
- Sodium Chloride (NaCl 0.9%) IVDocument3 pagesSodium Chloride (NaCl 0.9%) IVeaaemily13Pas encore d'évaluation
- Hypokalemia & Lethargy in Cat Due to Adrenal TumorDocument3 pagesHypokalemia & Lethargy in Cat Due to Adrenal TumorCabinet VeterinarPas encore d'évaluation
- Diabetic Ketoacidosis (DKA)Document33 pagesDiabetic Ketoacidosis (DKA)Eric Chye Teck100% (1)
- 2013 AAHA/AAFP Fluid Therapy Guidelines For Dogs and CatsDocument15 pages2013 AAHA/AAFP Fluid Therapy Guidelines For Dogs and CatsTatiana Amaya GomezPas encore d'évaluation
- Bmjcred00509 0023aDocument1 pageBmjcred00509 0023aBilly SandyPas encore d'évaluation
- The Effect of Storage Conditions On Sample Stability in The Routine Clinical LaboratoryDocument5 pagesThe Effect of Storage Conditions On Sample Stability in The Routine Clinical LaboratorysidomoyoPas encore d'évaluation
- DKA Guidelines Version 4.0 28 Dec 2016FINALDocument4 pagesDKA Guidelines Version 4.0 28 Dec 2016FINALbenPas encore d'évaluation
- 205 Management of Hypo Kala Emi ADocument11 pages205 Management of Hypo Kala Emi AGresonPas encore d'évaluation
- Pediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not DiagnosedDocument2 pagesPediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not Diagnosedrolland_arrizaPas encore d'évaluation
- Paed Parenteral Fluid ThyDocument1 pagePaed Parenteral Fluid ThyZulia Ahmad BurhaniPas encore d'évaluation
- Acute Hemodialysis PrescriptionDocument18 pagesAcute Hemodialysis PrescriptionOlga BabiiPas encore d'évaluation
- Hyperkalaemia - Management of Acute Hyperkalaemia in Adults - Canberra Health ServicesDocument6 pagesHyperkalaemia - Management of Acute Hyperkalaemia in Adults - Canberra Health ServicesIrina Cabac-PogoreviciPas encore d'évaluation
- Perioperative Fluid and Transfusion ManagementDocument52 pagesPerioperative Fluid and Transfusion ManagementIndah Fitri Okta100% (2)
- Terapi Cairan PD AnakDocument50 pagesTerapi Cairan PD AnakRaisa ArlizaPas encore d'évaluation
- Calculating Fluid Therapy for Burn PatientsDocument11 pagesCalculating Fluid Therapy for Burn PatientsAnusha Verghese100% (2)
- 6-Pharm Care Pada Terapi CairanDocument34 pages6-Pharm Care Pada Terapi CairanApt RatnaningrumPas encore d'évaluation
- Fluid Management & Shock Resuscitation KGD SMT 7 PDFDocument34 pagesFluid Management & Shock Resuscitation KGD SMT 7 PDFTikuqNyukUnyukUnyuk100% (1)
- IV Fluids: Understanding Daily Requirements and ComplicationsDocument17 pagesIV Fluids: Understanding Daily Requirements and ComplicationsBima BaikuniPas encore d'évaluation
- Potassium Chloride and Patient Safety: Yasser GebrilDocument21 pagesPotassium Chloride and Patient Safety: Yasser GebrilYasser GebrilPas encore d'évaluation
- NCM 109 Skills Lab Day 13.1 Arterial Blood Gas Abg22Document38 pagesNCM 109 Skills Lab Day 13.1 Arterial Blood Gas Abg22Sheena Patricia ArasulaPas encore d'évaluation
- Fluid Therapy GlsDocument11 pagesFluid Therapy GlsDavid PGPas encore d'évaluation
- Fluidtherapy Guidelines PDFDocument11 pagesFluidtherapy Guidelines PDFJoão Pedro PereiraPas encore d'évaluation
- Fluidtherapy GuidelinesDocument11 pagesFluidtherapy Guidelineshamida fillahPas encore d'évaluation
- Diabetic Ketoacidosis PathwayDocument22 pagesDiabetic Ketoacidosis PathwaySri Nath100% (1)
- Electrolyte Disturbance-1Document22 pagesElectrolyte Disturbance-1Doaa Abd El-WahabPas encore d'évaluation
- Revised DKA 2015 PDFDocument6 pagesRevised DKA 2015 PDFDr AhmedPas encore d'évaluation
- 3-Management of DF-DHF2018Document36 pages3-Management of DF-DHF2018koengphearom9Pas encore d'évaluation
- 555-Article Text-4693-2-10-20201212Document7 pages555-Article Text-4693-2-10-20201212bboyhelyPas encore d'évaluation
- BWH Hyperglycemia GuidelinesDocument7 pagesBWH Hyperglycemia Guidelinespmahesh107100% (1)
- Managing Hyperkalemia in CKD PatientsDocument8 pagesManaging Hyperkalemia in CKD PatientsPratik TripathiPas encore d'évaluation
- Acute Diabetic Ketoacidosis (DKA)Document21 pagesAcute Diabetic Ketoacidosis (DKA)Madhu Sudhan Pandeya0% (1)
- 2014 NEJM A New Era For The Treatment of HyperkDocument3 pages2014 NEJM A New Era For The Treatment of HyperkAndreea TudurachiPas encore d'évaluation
- Body EssentialselectrolytesDocument21 pagesBody EssentialselectrolytesAli HassanPas encore d'évaluation
- Iv Fluids: Beneficial or More Harm?Document20 pagesIv Fluids: Beneficial or More Harm?NinaPas encore d'évaluation
- Schypcal ProtocolDocument5 pagesSchypcal Protocolsuperiorsambrial examcellPas encore d'évaluation
- Dka Guidelines - 2012Document4 pagesDka Guidelines - 2012djizhieePas encore d'évaluation
- Terapi Cairan dan Transfusi dalam PerioperatifDocument47 pagesTerapi Cairan dan Transfusi dalam PerioperatifHelend ChildDjPas encore d'évaluation
- IvfDocument16 pagesIvfJohnRev Fundal Lopez LorenzoPas encore d'évaluation
- Hiperk PDFDocument26 pagesHiperk PDFmasranraisaPas encore d'évaluation
- Drug Study: Antacid GI: Belching, GastricDocument3 pagesDrug Study: Antacid GI: Belching, GastricJhon Jade PalagtiwPas encore d'évaluation
- Hypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandHypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Intracranial Pressure (Icp)Document41 pagesIntracranial Pressure (Icp)Roadtogot 2023Pas encore d'évaluation
- Ashly Schuyler CV Updated 04092023Document8 pagesAshly Schuyler CV Updated 04092023api-646057316Pas encore d'évaluation
- Cardiogenic Shock HandoutsDocument2 pagesCardiogenic Shock HandoutsAileenPas encore d'évaluation
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuPas encore d'évaluation
- 2016 UMEM ECG CompetitionDocument7 pages2016 UMEM ECG CompetitionCatherine MorrisPas encore d'évaluation
- Down SyndromeDocument9 pagesDown SyndromeJonnah100% (1)
- Chest X-Ray AnnaDocument51 pagesChest X-Ray Annaapi-26159412100% (1)
- Kami Export - Cardiovascular System Lecture Outline 1st PeriodDocument16 pagesKami Export - Cardiovascular System Lecture Outline 1st PeriodJada NovakPas encore d'évaluation
- AnginaDocument16 pagesAnginaMc_Lopez_1761Pas encore d'évaluation
- Complete Medical AbbreviationsDocument15 pagesComplete Medical AbbreviationsDiana Joy Cabote100% (1)
- JMDN en PDFDocument359 pagesJMDN en PDFFebiana Rima DiputriPas encore d'évaluation
- Comprehensive Guide To Understanding and Managing Leaky Heart SyndromeDocument15 pagesComprehensive Guide To Understanding and Managing Leaky Heart SyndromeshivaPas encore d'évaluation
- Facial Fillers ComplicationsDocument12 pagesFacial Fillers ComplicationsLewis PiersPas encore d'évaluation
- Part 1 of Cvs Anatomy and PhysiologyDocument11 pagesPart 1 of Cvs Anatomy and PhysiologyZacharia muraciaPas encore d'évaluation
- (GERIA) Quiz 1Document11 pages(GERIA) Quiz 1Charmaine AmagoPas encore d'évaluation
- AIIMS NORCET 2022 Memory Based Paper 11th September 2022 EnglishDocument20 pagesAIIMS NORCET 2022 Memory Based Paper 11th September 2022 EnglishMata BharatPas encore d'évaluation
- Adi Bestara EKG at A Glance NewestDocument113 pagesAdi Bestara EKG at A Glance Newestkarpax21100% (1)
- PP000266 60195174a M9753131Document5 pagesPP000266 60195174a M9753131dhrmendraPas encore d'évaluation
- Oet Simplified Medical Vocabulary Book SpeakingDocument72 pagesOet Simplified Medical Vocabulary Book SpeakingmyatPas encore d'évaluation
- By: Vismin Prince Magno: Liver CancerDocument17 pagesBy: Vismin Prince Magno: Liver Cancerhedokido100% (1)
- FCPS Pretest Golden File 1Document450 pagesFCPS Pretest Golden File 1Khadija AurangzebPas encore d'évaluation
- Cardiology - The Study and Treatment of Heart DisordersDocument7 pagesCardiology - The Study and Treatment of Heart Disorderssalam08Pas encore d'évaluation
- Burn Injury PathophysiologyDocument1 pageBurn Injury PathophysiologyMonique Ann DanoyPas encore d'évaluation
- MCQ HemodynamicsDocument2 pagesMCQ HemodynamicsKehkashan Khan80% (5)
- Cardiac CTDocument7 pagesCardiac CTdaniel7pintiliiPas encore d'évaluation
- Lbybio4 Label 00Document12 pagesLbybio4 Label 00Joanna Michelle AlmedaPas encore d'évaluation
- Erythrocyte Sedimentation RateDocument57 pagesErythrocyte Sedimentation Ratehirendra patelPas encore d'évaluation
- Basinger Abraham - ConsultationDocument80 pagesBasinger Abraham - ConsultationVikas NairPas encore d'évaluation
- Pleural EffusionDocument49 pagesPleural EffusionLyra Lorca86% (7)
- The Circulatory SystemDocument30 pagesThe Circulatory Systemapi-309893409Pas encore d'évaluation