Vous aimerez peut-être aussi
- Dok Baru 2019-02-25 16.54.03 - 3Document1 pageDok Baru 2019-02-25 16.54.03 - 3RatutiYetsiBiancaPas encore d'évaluation
- Expanded Dengue Syndrome - A Lesson Learnt: January 2018Document9 pagesExpanded Dengue Syndrome - A Lesson Learnt: January 2018RatutiYetsiBiancaPas encore d'évaluation
- Email MAMAHDocument1 pageEmail MAMAHRatutiYetsiBiancaPas encore d'évaluation
- PL Arun. Pediatric Glasgow Coma Scale. Bone and Spine. (Avaiable: Acssesed 12 Agustus 2018)Document1 pagePL Arun. Pediatric Glasgow Coma Scale. Bone and Spine. (Avaiable: Acssesed 12 Agustus 2018)RatutiYetsiBiancaPas encore d'évaluation
- Ricka, Board MatiDocument33 pagesRicka, Board MatiRatutiYetsiBiancaPas encore d'évaluation
- Email MAMAHDocument1 pageEmail MAMAHRatutiYetsiBiancaPas encore d'évaluation
- Kementerian Pendidikan Nasional Universitas Palangka Raya: Fe/Fkip/Faperta/Ft/Fh/Fisipol/ FKDocument1 pageKementerian Pendidikan Nasional Universitas Palangka Raya: Fe/Fkip/Faperta/Ft/Fh/Fisipol/ FKRatutiYetsiBiancaPas encore d'évaluation
- Gynec ExamDocument46 pagesGynec ExamWidiya Perwita SariPas encore d'évaluation
- Pediatricneurology 1 1002Document8 pagesPediatricneurology 1 1002RatutiYetsiBiancaPas encore d'évaluation
- Daftar Member Card ISMKIDocument2 pagesDaftar Member Card ISMKIRatutiYetsiBiancaPas encore d'évaluation
- Pediatricneurology 1 1002Document8 pagesPediatricneurology 1 1002RatutiYetsiBiancaPas encore d'évaluation
- Nama: Ratuti Yetsi Bianca NIM: FAA 114 040 Pembimbing 1: Dr. Francisca Diana Alexandra, M.SC Pembimbing 2: Dr. Donna Novina Kahanjak, M. BiomedDocument1 pageNama: Ratuti Yetsi Bianca NIM: FAA 114 040 Pembimbing 1: Dr. Francisca Diana Alexandra, M.SC Pembimbing 2: Dr. Donna Novina Kahanjak, M. BiomedRatutiYetsiBiancaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- How To Eat WellDocument68 pagesHow To Eat WelleledidiPas encore d'évaluation
- A Textual Introduction To Acarya Vasuvan PDFDocument3 pagesA Textual Introduction To Acarya Vasuvan PDFJim LeePas encore d'évaluation
- Earth Science (Metamorphic Rocks)Document8 pagesEarth Science (Metamorphic Rocks)MA. ALEXIS LAURENPas encore d'évaluation
- 412 X 7 Va CJ CSDocument1 page412 X 7 Va CJ CSRajesh KumarPas encore d'évaluation
- Updating - MTO I - Unit 2 ProblemsDocument3 pagesUpdating - MTO I - Unit 2 ProblemsmaheshPas encore d'évaluation
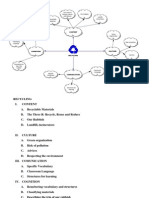
- Recycling Mind MapDocument2 pagesRecycling Mind Mapmsole124100% (1)
- SP 73Document105 pagesSP 73Rodrigo Vilanova100% (3)
- Module in Pe 103Document79 pagesModule in Pe 103Kym Dacudao100% (1)
- Mpfic54 PDFDocument201 pagesMpfic54 PDFAmy100% (1)
- Mini Project 1 - 1Document9 pagesMini Project 1 - 1Sameer BaraPas encore d'évaluation
- Vehicle Intercom Systems (VIS)Document4 pagesVehicle Intercom Systems (VIS)bbeisslerPas encore d'évaluation
- Me8072 Renewable Sources of EnergyDocument13 pagesMe8072 Renewable Sources of EnergyNallappan Rajj APas encore d'évaluation
- Clinical Case StudyDocument20 pagesClinical Case Studyapi-252004748Pas encore d'évaluation
- DNA Mutation and Its Effect To An Individual (w5)Document6 pagesDNA Mutation and Its Effect To An Individual (w5)Cold CoockiesPas encore d'évaluation
- Natural Disasters Vocabulary Exercises Fun Activities Games Icebreakers Oneonone Activiti 42747Document2 pagesNatural Disasters Vocabulary Exercises Fun Activities Games Icebreakers Oneonone Activiti 42747Andrea Tercero VillarroelPas encore d'évaluation
- Science Involved in Floating Paper Clip Science Experiment GuidelinesDocument4 pagesScience Involved in Floating Paper Clip Science Experiment GuidelinesSHIELA RUBIOPas encore d'évaluation
- iPQ-Center Webvideo Star TTB MA R1 42 en PDFDocument32 pagesiPQ-Center Webvideo Star TTB MA R1 42 en PDFHamid KharazmiPas encore d'évaluation
- Manual 35S EnglishDocument41 pagesManual 35S EnglishgugiPas encore d'évaluation
- Comparative Performance of Some Cattle Breeds Under Barani Conditions of PakistanDocument4 pagesComparative Performance of Some Cattle Breeds Under Barani Conditions of PakistanMasood HassanPas encore d'évaluation
- Disectie AnatomieDocument908 pagesDisectie AnatomieMircea SimionPas encore d'évaluation
- Donna Hay Magazine 2014-10-11 PDFDocument172 pagesDonna Hay Magazine 2014-10-11 PDFlekovic_tanjaPas encore d'évaluation
- Fret Position Calculator - StewmacDocument1 pageFret Position Calculator - StewmacJuan Pablo Sepulveda SierraPas encore d'évaluation
- Pharmd CurriculumDocument18 pagesPharmd Curriculum5377773Pas encore d'évaluation
- SPM 1449 2006 Mathematics p2 BerjawapanDocument18 pagesSPM 1449 2006 Mathematics p2 Berjawapanpss smk selandar71% (7)
- Manual Nice9000v A04Document151 pagesManual Nice9000v A04hoang tamPas encore d'évaluation
- Convection Concentric Annulus Vertical Cylinders Filling Porous MediaDocument17 pagesConvection Concentric Annulus Vertical Cylinders Filling Porous MediakarthikeyanPas encore d'évaluation
- Math 202 Syllabus-Spring18 PDFDocument2 pagesMath 202 Syllabus-Spring18 PDFvonacoc49Pas encore d'évaluation
- Plato: Epistemology: Nicholas WhiteDocument2 pagesPlato: Epistemology: Nicholas WhiteAnonymous HCqIYNvPas encore d'évaluation
- Tran-Effects of Assisted JumpingDocument5 pagesTran-Effects of Assisted JumpingyoungjessPas encore d'évaluation