Vous aimerez peut-être aussi
- A Case of Umbilical Endometriosis: Villar's NoduleDocument5 pagesA Case of Umbilical Endometriosis: Villar's Noduleari naPas encore d'évaluation
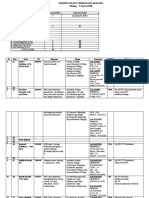
- 304638-MAPING ARAFAH 3 Minggu 5 Januari 2020) .FileDocument4 pages304638-MAPING ARAFAH 3 Minggu 5 Januari 2020) .Fileari naPas encore d'évaluation
- 1 s2.0 S0959804911009336 MainDocument11 pages1 s2.0 S0959804911009336 Mainari naPas encore d'évaluation
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument13 pagesBest Practice & Research Clinical Obstetrics and Gynaecologyari naPas encore d'évaluation
- Omphalocele and Gastroschisis: Wendy Nguyen and Kumar BelaniDocument8 pagesOmphalocele and Gastroschisis: Wendy Nguyen and Kumar Belaniari naPas encore d'évaluation
- Congenital MalformationsDocument9 pagesCongenital MalformationsibnuPas encore d'évaluation
- Primary Umbilical Endometriosis. Case Report and Discussion On Management OptionsDocument7 pagesPrimary Umbilical Endometriosis. Case Report and Discussion On Management Optionsari naPas encore d'évaluation
- Mechanisms For Lysophosphatidic Acid-Induced Cytokine Production in Ovarian Cancer CellsDocument9 pagesMechanisms For Lysophosphatidic Acid-Induced Cytokine Production in Ovarian Cancer Cellsari naPas encore d'évaluation
- 10 1016@j Ijscr 2020 01 020Document4 pages10 1016@j Ijscr 2020 01 020ari naPas encore d'évaluation
- 1 s2.0 S0959804911009336 MainDocument11 pages1 s2.0 S0959804911009336 Mainari naPas encore d'évaluation
- Diagnosis and Management Primary AmenoreaDocument18 pagesDiagnosis and Management Primary AmenoreaUray Dimas AnandhaPas encore d'évaluation
- Omphalocele and Gastroschisis: Wendy Nguyen and Kumar BelaniDocument8 pagesOmphalocele and Gastroschisis: Wendy Nguyen and Kumar Belaniari naPas encore d'évaluation
- S S I L I: Eptic Hock After Ntracervical Aminaria NsertionDocument3 pagesS S I L I: Eptic Hock After Ntracervical Aminaria Nsertionari naPas encore d'évaluation
- S S I L I: Eptic Hock After Ntracervical Aminaria NsertionDocument3 pagesS S I L I: Eptic Hock After Ntracervical Aminaria Nsertionari naPas encore d'évaluation
- S S I L I: Eptic Hock After Ntracervical Aminaria NsertionDocument3 pagesS S I L I: Eptic Hock After Ntracervical Aminaria Nsertionari naPas encore d'évaluation
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument13 pagesBest Practice & Research Clinical Obstetrics and Gynaecologyari naPas encore d'évaluation
- S S I L I: Eptic Hock After Ntracervical Aminaria NsertionDocument3 pagesS S I L I: Eptic Hock After Ntracervical Aminaria Nsertionari naPas encore d'évaluation
- The Efficacy of Crown Rump Length Measurement by Ultrasound in Estimating The Gestational AgeDocument7 pagesThe Efficacy of Crown Rump Length Measurement by Ultrasound in Estimating The Gestational Ageari naPas encore d'évaluation
- DR 20 September Shift IDocument7 pagesDR 20 September Shift Iari naPas encore d'évaluation
- Hang Tuah Medical Journal: Wardani, HTMJ Volume 15 No 1 2017Document10 pagesHang Tuah Medical Journal: Wardani, HTMJ Volume 15 No 1 2017Gufron MustofaPas encore d'évaluation
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument13 pagesBest Practice & Research Clinical Obstetrics and Gynaecologyari naPas encore d'évaluation
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument13 pagesBest Practice & Research Clinical Obstetrics and Gynaecologyari naPas encore d'évaluation
- 304638-MAPING ARAFAH 3 Minggu 5 Januari 2020) .FileDocument4 pages304638-MAPING ARAFAH 3 Minggu 5 Januari 2020) .Fileari naPas encore d'évaluation
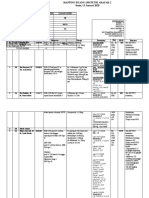
- Mapping Ruang Obstetri Arafah 2 Sabtu, 11 Januari 2020Document5 pagesMapping Ruang Obstetri Arafah 2 Sabtu, 11 Januari 2020ari naPas encore d'évaluation
- DR 20 September Shift IDocument7 pagesDR 20 September Shift Iari naPas encore d'évaluation
- Gestational Diabetes: By: Fatima ChoudaryDocument26 pagesGestational Diabetes: By: Fatima Choudaryari naPas encore d'évaluation
- Keterangan Hamil: 0 Post Sc:5 Post Pv:0 Post Vakum ILO:0 Post Manual Plasenta:0 Pasien Ginekologi:0 Post Kuretase: 1Document3 pagesKeterangan Hamil: 0 Post Sc:5 Post Pv:0 Post Vakum ILO:0 Post Manual Plasenta:0 Pasien Ginekologi:0 Post Kuretase: 1ari naPas encore d'évaluation
- Keterangan Hamil: 0 Post Sc:5 Post Pv:0 Post Vakum ILO:0 Post Manual Plasenta:0 Pasien Ginekologi:0 Post Kuretase: 1Document3 pagesKeterangan Hamil: 0 Post Sc:5 Post Pv:0 Post Vakum ILO:0 Post Manual Plasenta:0 Pasien Ginekologi:0 Post Kuretase: 1ari naPas encore d'évaluation
- MATERNAL DISEASE-PEB-EclampsiaDocument10 pagesMATERNAL DISEASE-PEB-Eclampsiaari naPas encore d'évaluation
- Acog 2019-Pregnancy N Heart DiseaseDocument37 pagesAcog 2019-Pregnancy N Heart Diseaseari naPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- 00.docii 2020 Renal - UrogenitalDocument13 pages00.docii 2020 Renal - Urogenitalanderson ndabishakaPas encore d'évaluation
- Volcke 2021Document6 pagesVolcke 2021Spica RegulusPas encore d'évaluation
- ALZENTALDocument2 pagesALZENTALmahgadPas encore d'évaluation
- MS.K.49.Pituitary DisordersDocument36 pagesMS.K.49.Pituitary DisordersJuliana Sari HarahapPas encore d'évaluation
- Pathophysiology: Lipomas LiposarcomasDocument3 pagesPathophysiology: Lipomas LiposarcomasRizki KhairPas encore d'évaluation
- Differentiation of Pityriasis Rubra Pilaris From Plaque Psoriasis by DermosDocument4 pagesDifferentiation of Pityriasis Rubra Pilaris From Plaque Psoriasis by DermoscharoitePas encore d'évaluation
- OBGYN History FormDocument2 pagesOBGYN History FormSandeep GhosthPas encore d'évaluation
- Intl J Gynecology Obste - 2018 - Berek - Cancer of The Ovary Fallopian Tube and PeritoneumDocument20 pagesIntl J Gynecology Obste - 2018 - Berek - Cancer of The Ovary Fallopian Tube and PeritoneumHưng Nguyễn - Yola T.A.Pas encore d'évaluation
- Acute Pain - Mastectomy - Breast CADocument2 pagesAcute Pain - Mastectomy - Breast CAAngie MandeoyaPas encore d'évaluation
- The Amazing BrainDocument13 pagesThe Amazing BrainhaveanicedayPas encore d'évaluation
- Hematologic ManagementDocument17 pagesHematologic ManagementAlyssa MontimorPas encore d'évaluation
- Kim 2015Document10 pagesKim 2015cekPas encore d'évaluation
- Osce Book 3rdDocument39 pagesOsce Book 3rdأحمد الكندي100% (1)
- Association of Facial Exercise With The AppearanceDocument4 pagesAssociation of Facial Exercise With The AppearanceintenselightPas encore d'évaluation
- Feature and Sports WritingDocument27 pagesFeature and Sports WritingJoemar Furigay100% (1)
- Fluid Volume ExcessDocument4 pagesFluid Volume ExcessChristine Quirona100% (1)
- Feline Mesenteric Form of Multinodal Lymphoma: A Case ReportDocument7 pagesFeline Mesenteric Form of Multinodal Lymphoma: A Case ReportfirdousPas encore d'évaluation
- Hematologic MS Nclex QuestionsDocument36 pagesHematologic MS Nclex QuestionsSophia Rose Delos Santos100% (2)
- SXDocument126 pagesSXpalak32Pas encore d'évaluation
- December 2012 Pnle Pearls of Success Part 6: Medical and Surgical Health Nursing (A)Document11 pagesDecember 2012 Pnle Pearls of Success Part 6: Medical and Surgical Health Nursing (A)Haifi HunPas encore d'évaluation
- Diagnostic Testing-Student Review Diagnostic Testing-Student ReviewDocument10 pagesDiagnostic Testing-Student Review Diagnostic Testing-Student ReviewVin Lorenzo CampbellPas encore d'évaluation
- Safe Operation of Kilns, Furnaces & Driers: A Tool Kit For BusinessDocument23 pagesSafe Operation of Kilns, Furnaces & Driers: A Tool Kit For BusinessAdewalePas encore d'évaluation
- Junior Surgery Exam MCQSDocument14 pagesJunior Surgery Exam MCQSJohn M. Hemsworth89% (9)
- IKD5 - Interventional Uro-Radiology - Current Practices and Aspirations in MauritiusDocument81 pagesIKD5 - Interventional Uro-Radiology - Current Practices and Aspirations in MauritiusRenal Association MauritiusPas encore d'évaluation
- Slide Preparation of Cerebrospinal Fluid For Cytological ExaminationDocument3 pagesSlide Preparation of Cerebrospinal Fluid For Cytological ExaminationMurshed HaidarPas encore d'évaluation
- Kyle LiDocument12 pagesKyle Liapi-407846283Pas encore d'évaluation
- Aspergillus NomiusDocument7 pagesAspergillus NomiusMuh. Ade ArtasastaPas encore d'évaluation
- Housing Letter PDFDocument1 pageHousing Letter PDFLaxmi AbundancePas encore d'évaluation
- Barriers To Cervical Cancer Among Hispanic WomenDocument8 pagesBarriers To Cervical Cancer Among Hispanic WomenSana ShoaibPas encore d'évaluation
- Preporuke Za Hrqol GR: Vodiči Za Karcinom ProstateDocument12 pagesPreporuke Za Hrqol GR: Vodiči Za Karcinom ProstateAndjela KosticPas encore d'évaluation