Vous aimerez peut-être aussi
- Andrews Diseases of The Skin Clinical Dermatology, 12th Ed - James, Berger, Elston, - NeuhausDocument1 083 pagesAndrews Diseases of The Skin Clinical Dermatology, 12th Ed - James, Berger, Elston, - NeuhausToni De Guzman Laluna100% (2)
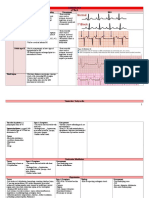
- A Visual Guide To ECG Interpretation 2e 40 Jan 1 2017 41 40 1496321537 41 40 LWW 41Document1 578 pagesA Visual Guide To ECG Interpretation 2e 40 Jan 1 2017 41 40 1496321537 41 40 LWW 41xtinePas encore d'évaluation
- Case Study of Children With Special NeedsDocument21 pagesCase Study of Children With Special NeedsGrf Trust83% (69)
- Advanced Medicine Recall A Must For MRCP PDFDocument712 pagesAdvanced Medicine Recall A Must For MRCP PDFKai Xin100% (2)
- 101 Clinical Cases in Emergency Room Book PDFDocument1 page101 Clinical Cases in Emergency Room Book PDFHhaPas encore d'évaluation
- Saint-Frances Guide To Inpatient MedicineDocument281 pagesSaint-Frances Guide To Inpatient Medicineorijinal100% (2)
- 978190medicine5635856 PDFDocument18 pages978190medicine5635856 PDFMuhammad TariqPas encore d'évaluation
- PEAC OphthalmologyDocument45 pagesPEAC OphthalmologySdPas encore d'évaluation
- (Ruth Ballweg, MPA, PA-C, Edward M. Sullivan, MS, (B-Ok - Xyz) PDFDocument939 pages(Ruth Ballweg, MPA, PA-C, Edward M. Sullivan, MS, (B-Ok - Xyz) PDFJim Velasquez100% (1)
- Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, Updated Edition - Periocular Infections PDFDocument10 pagesMandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, Updated Edition - Periocular Infections PDFCarimaGhaliePas encore d'évaluation
- First Aid PsychiatryDocument156 pagesFirst Aid PsychiatryMae Matira AbeladorPas encore d'évaluation
- The Heart Manual: Post Myocardial Infarction (Post MI) EditionDocument18 pagesThe Heart Manual: Post Myocardial Infarction (Post MI) EditionPablo L RodriguezPas encore d'évaluation
- Robin Bhatia, Ian Sabin-Challenging Concepts in Neurosurgery - Cases With Expert Commentary-Oxford University Press (2015)Document253 pagesRobin Bhatia, Ian Sabin-Challenging Concepts in Neurosurgery - Cases With Expert Commentary-Oxford University Press (2015)rogeriotorres13100% (1)
- Primary CareDocument184 pagesPrimary Carehaneefmdf100% (1)
- Family Centred CareDocument20 pagesFamily Centred CareMiftakhul KhoeryPas encore d'évaluation
- Nbme 6Document14 pagesNbme 6Amber MerrittPas encore d'évaluation
- Cautionary Tales PDFDocument32 pagesCautionary Tales PDFAfreenZaraPas encore d'évaluation
- Case Files Emergency MedicineDocument480 pagesCase Files Emergency MedicinestarrnewmanpaPas encore d'évaluation
- Neurology Study Guide Oral Board Exam ReviewDocument1 pageNeurology Study Guide Oral Board Exam Reviewxmc5505Pas encore d'évaluation
- Neuroanatomy Through Clinical Cases, 2E PDFDocument3 pagesNeuroanatomy Through Clinical Cases, 2E PDFjwongggg55140% (6)
- Ophelia'S Case: Oleh: Anggun Fitri Utami, S, Ked PembimbingDocument20 pagesOphelia'S Case: Oleh: Anggun Fitri Utami, S, Ked PembimbingAnggun Cimey UtamiPas encore d'évaluation
- Lanka Hospitals ReportDocument25 pagesLanka Hospitals ReportRickyRikzPas encore d'évaluation
- Antibiotic Prescribing in Primary Care - Therapeutic Guidelines Summary Table 2019Document2 pagesAntibiotic Prescribing in Primary Care - Therapeutic Guidelines Summary Table 2019RL100% (1)
- 000-Intro To Internal MedicineDocument6 pages000-Intro To Internal MedicineRizky KykyPas encore d'évaluation
- Lista Carti Accesibile Online PDFDocument21 pagesLista Carti Accesibile Online PDFSabrina MoraruPas encore d'évaluation
- Dermatology Slides - Introduction To Clinical DermatologyDocument34 pagesDermatology Slides - Introduction To Clinical DermatologyAzry Mustapa100% (1)
- Neurosurgery Ward TopicsDocument10 pagesNeurosurgery Ward TopicsMaroofAliPas encore d'évaluation
- Cabo H. Color Atlas of Dermoscopy 2018Document354 pagesCabo H. Color Atlas of Dermoscopy 2018Esther ParvuPas encore d'évaluation
- 2021 Nelson AntibioticDocument377 pages2021 Nelson AntibioticlatifahPas encore d'évaluation
- Gates Sample Chapter Neurology PDFDocument50 pagesGates Sample Chapter Neurology PDFpartha9sarathi9ain100% (1)
- Geriatric PharmacologyDocument77 pagesGeriatric PharmacologyKhirsna PasajolPas encore d'évaluation
- Stage 1: Dorsal Induction: Pediatric NeuroradiologyDocument8 pagesStage 1: Dorsal Induction: Pediatric Neuroradiologysarguss14100% (1)
- SinusitisDocument402 pagesSinusitisIsidro Roberto Santana Gonzalez100% (1)
- Rational Laboratory and Diagnostic TestsDocument26 pagesRational Laboratory and Diagnostic TestsCeline dela cruzPas encore d'évaluation
- Evidence Based Emergency Care PDFDocument2 pagesEvidence Based Emergency Care PDFMelissa0% (1)
- Plastic and Orbital SurgeryDocument201 pagesPlastic and Orbital Surgeryaboujis100% (1)
- Orthopedic Essentials in Emergency MedicineDocument35 pagesOrthopedic Essentials in Emergency MedicineMohd Tarmizi100% (1)
- Casebook Book: Famil yDocument24 pagesCasebook Book: Famil ylentini@maltanet.net100% (1)
- Pain Management in The Emergency DepartmentDocument28 pagesPain Management in The Emergency DepartmentJuan Carlos CostaPas encore d'évaluation
- Case History and Data Interpretation in Medical PracticeDocument563 pagesCase History and Data Interpretation in Medical PracticesaifabaasPas encore d'évaluation
- June 2021 MCQ Psychiatry at DAMSDocument61 pagesJune 2021 MCQ Psychiatry at DAMSAli HusseinPas encore d'évaluation
- Family Medicine Exam Manual 2011Document72 pagesFamily Medicine Exam Manual 2011SultanAlam50% (2)
- Eye Emergency ManualDocument56 pagesEye Emergency Manualgraci91031462296100% (1)
- (Libribook - Com) Graber and Wilburs Family Medicine Examination and Board Review 5th EditionDocument882 pages(Libribook - Com) Graber and Wilburs Family Medicine Examination and Board Review 5th EditionPunnaphat Tinnaphop DaraswangPas encore d'évaluation
- Trim Labiaplasty.8Document2 pagesTrim Labiaplasty.8Afif MansorPas encore d'évaluation
- Internal Medicine - DermatologyDocument125 pagesInternal Medicine - DermatologySoleil DaddouPas encore d'évaluation
- Pocket Primary Care (Pocket Notebook... by Curtis ChongDocument7 312 pagesPocket Primary Care (Pocket Notebook... by Curtis ChongPaolo A. Cabeza Martinez10% (10)
- Textbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyD'EverandTextbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyPas encore d'évaluation
- Emergency Medicine Primer (Geiselmed - Dartmouth)Document108 pagesEmergency Medicine Primer (Geiselmed - Dartmouth)Irene Franz100% (1)
- And&Dis&Ski&Cli&Atl&Jam&Els&Mcm&1 STDocument580 pagesAnd&Dis&Ski&Cli&Atl&Jam&Els&Mcm&1 STelliealderseyPas encore d'évaluation
- Paediatric Surgery For GPDocument58 pagesPaediatric Surgery For GPAbid Hasan ZiKon100% (1)
- Family Medicine Case FilesDocument44 pagesFamily Medicine Case FilesTazan VoPas encore d'évaluation
- Ear, Nose, and Throat EmergenciesDocument23 pagesEar, Nose, and Throat EmergenciesRajesh SharmaPas encore d'évaluation
- Medico Notes PediatricsDocument40 pagesMedico Notes PediatricsTrisPas encore d'évaluation
- ED Study GuideDocument59 pagesED Study Guidemmmmz100% (1)
- A Short Guide To Preparing For The Fellowship Examination: Australian Board in General SurgeryDocument9 pagesA Short Guide To Preparing For The Fellowship Examination: Australian Board in General SurgeryDronacharya RouthPas encore d'évaluation
- North Carolina Children’s Global Health Handbook: A Pediatrician’s Guide to Integrating IMCI Guidelines in Sub-Saharan AfricaD'EverandNorth Carolina Children’s Global Health Handbook: A Pediatrician’s Guide to Integrating IMCI Guidelines in Sub-Saharan AfricaErica C. BjornstadPas encore d'évaluation
- Chalazion and Hordeolum (Stye) - Eye Disorders - MSD Manual Professional EditionDocument4 pagesChalazion and Hordeolum (Stye) - Eye Disorders - MSD Manual Professional EditionCarimaGhaliePas encore d'évaluation
- 8-Visual Cues Ophthalmology PDFDocument64 pages8-Visual Cues Ophthalmology PDFCarimaGhaliePas encore d'évaluation
- Hordeolum and ChalazionDocument13 pagesHordeolum and ChalazionCarimaGhaliePas encore d'évaluation
- Constipation Guideline PDFDocument13 pagesConstipation Guideline PDFCarimaGhaliePas encore d'évaluation
- Bezold AbscessDocument5 pagesBezold AbscessCarimaGhaliePas encore d'évaluation
- Complications of Otitis MediaDocument6 pagesComplications of Otitis MediaCarimaGhaliePas encore d'évaluation
- Case Bezold AbscessDocument3 pagesCase Bezold AbscessCarimaGhaliePas encore d'évaluation
- Anatomy and Physiology of The HeartDocument22 pagesAnatomy and Physiology of The HeartCarimaGhalie100% (2)
- British Guideline On The Management of AsthmaDocument98 pagesBritish Guideline On The Management of AsthmaCarimaGhaliePas encore d'évaluation
- Panic Disorder:: When Fear OverwhelmsDocument8 pagesPanic Disorder:: When Fear OverwhelmsCarimaGhalie100% (1)
- Eisenmenger SyndromeDocument6 pagesEisenmenger SyndromeCarimaGhaliePas encore d'évaluation
- Nephrotic Syndrome: DR Thuvaraka WareDocument5 pagesNephrotic Syndrome: DR Thuvaraka Warechloe1411Pas encore d'évaluation
- Mindfulness Literature ReviewDocument7 pagesMindfulness Literature Reviewjquail3Pas encore d'évaluation
- Anima: Beyond Fantasy Character SheetDocument4 pagesAnima: Beyond Fantasy Character SheetTristan TaksonPas encore d'évaluation
- Shako, Kay. Sociodemographic Factors Culture and Suicide in GuyanaDocument93 pagesShako, Kay. Sociodemographic Factors Culture and Suicide in GuyanaMarcela FranzenPas encore d'évaluation
- Organic Anti-Aging Blend Essential Oil (100 Pure - USDA Certified Organic) Best Therapeutic Grade Essential Oil - 1Document1 pageOrganic Anti-Aging Blend Essential Oil (100 Pure - USDA Certified Organic) Best Therapeutic Grade Essential Oil - 1Leandro LucatoPas encore d'évaluation
- Anesthesia April 2020 PDFDocument130 pagesAnesthesia April 2020 PDFFA KhanPas encore d'évaluation
- CNA Body Mechanics Bed Making Comfort CareDocument32 pagesCNA Body Mechanics Bed Making Comfort CareFaith VaughnPas encore d'évaluation
- Rebeccas Resume Updated 7-2016Document1 pageRebeccas Resume Updated 7-2016api-498987425Pas encore d'évaluation
- DRRM Toolkit Book - Final PDFDocument379 pagesDRRM Toolkit Book - Final PDFAnonymous JLQBb3JPas encore d'évaluation
- Inguinal Abscess Following CastrationDocument2 pagesInguinal Abscess Following Castrationfahmi rosyadiPas encore d'évaluation
- Drug AddictionDocument4 pagesDrug AddictionManoz Thapa KajiPas encore d'évaluation
- Stress ManagementDocument106 pagesStress ManagementSanthosh SomaPas encore d'évaluation
- FY 2022 GAA ProvisionsDocument2 pagesFY 2022 GAA ProvisionsGamu DILGPas encore d'évaluation
- TPCL-2 Đề Tham Khảo Anh Văn 7 Học Kì 1Document2 pagesTPCL-2 Đề Tham Khảo Anh Văn 7 Học Kì 1Ms Đỗ HiếuPas encore d'évaluation
- Foreword: OIE Terrestrial Manual 2008 IIIDocument8 pagesForeword: OIE Terrestrial Manual 2008 IIIWormInchPas encore d'évaluation
- OkhlaDocument55 pagesOkhlaPoojit Popli50% (2)
- Health Vocabulary ListDocument7 pagesHealth Vocabulary ListClaudia MacariePas encore d'évaluation
- Budgeted Lesson.1st Quarter - PERDEVDocument3 pagesBudgeted Lesson.1st Quarter - PERDEVJonalyn Banez100% (1)
- Experiment: Analysis of Milk: Output by Christian James MataDocument2 pagesExperiment: Analysis of Milk: Output by Christian James MataSIJIPas encore d'évaluation
- Specific Lifting Pland - OHS-PR-009 - FM-01-051. Rv2Document2 pagesSpecific Lifting Pland - OHS-PR-009 - FM-01-051. Rv2cmrig74Pas encore d'évaluation
- J. Nat. Prod., 1994, 57 (4), 518-520Document4 pagesJ. Nat. Prod., 1994, 57 (4), 518-520Casca RMPas encore d'évaluation
- Jurnal Forensik 1Document7 pagesJurnal Forensik 1Rizky ErizkaPas encore d'évaluation
- Calculation in ApheresisDocument5 pagesCalculation in Apheresismilica cucuzPas encore d'évaluation
- Grounwater and Its Susceptability To DegradationDocument140 pagesGrounwater and Its Susceptability To DegradationJoseph KyeyunePas encore d'évaluation
- Prescribing in Dermatology - Polly BuchananDocument136 pagesPrescribing in Dermatology - Polly BuchananFarah Kurniasari100% (1)
- United Nations For Class 8Document36 pagesUnited Nations For Class 8zeeschool25% (4)
- Mapeh 8-2ND Semi QuarterDocument5 pagesMapeh 8-2ND Semi QuarterQueenie GamboaPas encore d'évaluation
- Urinary Tract Infections in ChildrenDocument16 pagesUrinary Tract Infections in ChildrenPraluki HerliawanPas encore d'évaluation