Vous aimerez peut-être aussi
- Ericksonian Approaches To Pain ManagementDocument6 pagesEricksonian Approaches To Pain Managementosher2650% (2)
- The Ultimate Gastric Sleeve Bariatric Diet Cookbook:The Essential Nutrition Guide For Every Phase Of Recovery After Weight Loss Surgery With Delectable And Nutritious RecipesD'EverandThe Ultimate Gastric Sleeve Bariatric Diet Cookbook:The Essential Nutrition Guide For Every Phase Of Recovery After Weight Loss Surgery With Delectable And Nutritious RecipesPas encore d'évaluation
- The Wonder of Probiotics: A 30-Day Plan to Boost Energy, Enhance Weight Loss, Heal GI Problems, Prevent Disease, and Slow AgingD'EverandThe Wonder of Probiotics: A 30-Day Plan to Boost Energy, Enhance Weight Loss, Heal GI Problems, Prevent Disease, and Slow AgingPas encore d'évaluation
- Cardiovascular Pathology: Risks, Heart Failure, AMIDocument5 pagesCardiovascular Pathology: Risks, Heart Failure, AMIbmhsh100% (2)
- Diverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesD'EverandDiverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesÉvaluation : 1 sur 5 étoiles1/5 (1)
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesD'EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesÉvaluation : 5 sur 5 étoiles5/5 (2)
- Nursing Care Plan ConstipationDocument3 pagesNursing Care Plan Constipationbmrose3783% (12)
- Cystitis, A Simple Guide To The Condition Treatment And Urinary DiseasesD'EverandCystitis, A Simple Guide To The Condition Treatment And Urinary DiseasesPas encore d'évaluation
- JNC 8 Guideline Algorithm for Treating HypertensionDocument2 pagesJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- JNC 8 Guideline Algorithm for Treating HypertensionDocument2 pagesJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- Nursing Care Plan Urinary Tract Infection (UTI)Document2 pagesNursing Care Plan Urinary Tract Infection (UTI)deric95% (97)
- The Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesD'EverandThe Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesPas encore d'évaluation
- Prostatitis, A Simple Guide to the Condition, Treatment and Related DiseasesD'EverandProstatitis, A Simple Guide to the Condition, Treatment and Related DiseasesÉvaluation : 3 sur 5 étoiles3/5 (1)
- The Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesD'EverandThe Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesPas encore d'évaluation
- Medical Surgical NursingDocument21 pagesMedical Surgical Nursingicy431Pas encore d'évaluation
- UTI Treatment Algorithm - Sharp Mesa Vista 2Document3 pagesUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997Pas encore d'évaluation
- Acute sinusitis antibiotic guidelinesDocument2 pagesAcute sinusitis antibiotic guidelinesHana Liska DenitaPas encore d'évaluation
- UTI Guideline Example 2 Appendix B PDFDocument4 pagesUTI Guideline Example 2 Appendix B PDFamira catriPas encore d'évaluation
- UroGenital Infections GuideDocument5 pagesUroGenital Infections GuideDrashty DesaiPas encore d'évaluation
- Visual Summary PDF 4656316717Document2 pagesVisual Summary PDF 4656316717BhavyaPas encore d'évaluation
- NICE Otitis Media GuidelineDocument2 pagesNICE Otitis Media GuidelinerjPas encore d'évaluation
- Nosocomial Pneumonia RXDocument3 pagesNosocomial Pneumonia RXCHETAN SOMUPas encore d'évaluation
- Drugn Study 2 0Document15 pagesDrugn Study 2 0Ken ChavezPas encore d'évaluation
- CPG UtiDocument4 pagesCPG UtiNomar NonatoPas encore d'évaluation
- Uti PDFDocument1 pageUti PDFKurouSakiPas encore d'évaluation
- Cystitis symptoms, causes and treatmentDocument2 pagesCystitis symptoms, causes and treatmentIgri Septian Risky DiaanPas encore d'évaluation
- Management of Urinary Tract Infections (Utis) in Non-Catheterized Long-Term Care Home ResidentsDocument29 pagesManagement of Urinary Tract Infections (Utis) in Non-Catheterized Long-Term Care Home Residentsnz chuksPas encore d'évaluation
- Treating Your Infection UtiDocument1 pageTreating Your Infection UtiJames 'jps' SimanjuntakPas encore d'évaluation
- Antibiotics 2Document8 pagesAntibiotics 2makondotakundaPas encore d'évaluation
- Bacteria 1. Cystitis - Is An Signs: Urinary System: Disease and Causes Manifestation Treatment PreventionDocument16 pagesBacteria 1. Cystitis - Is An Signs: Urinary System: Disease and Causes Manifestation Treatment PreventionMc MagtibayPas encore d'évaluation
- Diabetic Foot NICEDocument3 pagesDiabetic Foot NICEBosco WoodsPas encore d'évaluation
- Pharmacology Coursework on GIT Drugs Including Antacids and Mucosal ProtectantsDocument7 pagesPharmacology Coursework on GIT Drugs Including Antacids and Mucosal ProtectantsTrisha Isobel DavePas encore d'évaluation
- Educational Module For Nursing Assistants in Long-Term Care Facilities: Urinary Tract Infections and Asymptomatic BacteriuriaDocument35 pagesEducational Module For Nursing Assistants in Long-Term Care Facilities: Urinary Tract Infections and Asymptomatic BacteriuriaPH Ph GnsoPas encore d'évaluation
- UTI TreatmentDocument3 pagesUTI TreatmentMaria RezitadinaPas encore d'évaluation
- Pamphlet Jan 8 PDFDocument2 pagesPamphlet Jan 8 PDFRouetchen AshleePas encore d'évaluation
- Medsurg: 6.3 Urinary DisordersDocument5 pagesMedsurg: 6.3 Urinary DisordersIvy VillalobosPas encore d'évaluation
- Oxacillin Nursing ConsiderationsDocument1 pageOxacillin Nursing Considerationsnerissa_villanueva3523Pas encore d'évaluation
- Nursing Care Plan Urinary Tract Infection UTIDocument2 pagesNursing Care Plan Urinary Tract Infection UTITrida Hermano CabansagPas encore d'évaluation
- Urinary Tract PDFDocument2 pagesUrinary Tract PDFVette Angelikka Dela CruzPas encore d'évaluation
- Cefuroxime Drug Study Rosemarie Llanillo BSN Ii eDocument3 pagesCefuroxime Drug Study Rosemarie Llanillo BSN Ii eFernandez, Florence NicolePas encore d'évaluation
- Antibiotic Guidelines For Adults 2018 PDFDocument58 pagesAntibiotic Guidelines For Adults 2018 PDFAhmad RizqiPas encore d'évaluation
- F. Drug Study: Drug Dosage Action Indication/ Contraindications Adverse Effects Nursing ResponsibilitiesDocument2 pagesF. Drug Study: Drug Dosage Action Indication/ Contraindications Adverse Effects Nursing ResponsibilitiesTracy Megan RusillonPas encore d'évaluation
- Megan Culata - GIT Drugs CourseworkDocument18 pagesMegan Culata - GIT Drugs CourseworkMegshiePas encore d'évaluation
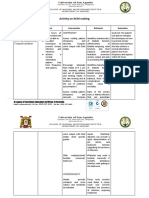
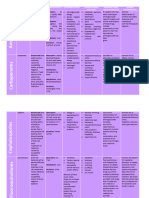
- Activity On NCM MakingDocument4 pagesActivity On NCM MakingJollan Marie BuenvenidaPas encore d'évaluation
- Is Antibiotic Treatment Indicated in A Patient With A Positive Urine Culture But No SymptomsDocument4 pagesIs Antibiotic Treatment Indicated in A Patient With A Positive Urine Culture But No Symptomstsiko111Pas encore d'évaluation
- Table of AntibioticsDocument5 pagesTable of AntibioticsBerenese DiannePas encore d'évaluation
- Pharma AntibioticsDocument4 pagesPharma Antibioticsvaldez.adler.lPas encore d'évaluation
- Lecture 12 Chapter 52Document5 pagesLecture 12 Chapter 52Duran JustinePas encore d'évaluation
- Gonorrhea Treatment Guidelines SummaryDocument1 pageGonorrhea Treatment Guidelines SummaryJoe DettPas encore d'évaluation
- Funda Sample ScenarioDocument2 pagesFunda Sample ScenarioGadez JeanpelPas encore d'évaluation
- لمى الشهري نيرس كير بلان تو بيييDocument8 pagesلمى الشهري نيرس كير بلان تو بيييلمى الشهريPas encore d'évaluation
- Byron - Recurrent Resistant Urinary Tract InfectionsDocument8 pagesByron - Recurrent Resistant Urinary Tract InfectionsC GPas encore d'évaluation
- NCP - Impaired Urinary EliminationDocument3 pagesNCP - Impaired Urinary EliminationFretzgine Lou ManuelPas encore d'évaluation
- Nursing Care Plan - Uti Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesNursing Care Plan - Uti Assessment Diagnosis Inference Planning Intervention Rationale Evaluationmark327Pas encore d'évaluation
- CAUTI Prevention in The Continuum of Care Teleclass Slides, Mar.29.17Document49 pagesCAUTI Prevention in The Continuum of Care Teleclass Slides, Mar.29.17NilakusumaPas encore d'évaluation
- Uti ProphylaxisDocument9 pagesUti ProphylaxisaPas encore d'évaluation
- Catheter-Associated Urinary Tract Infection (CAUTI) : Prevention Diagnosis and ManagementDocument6 pagesCatheter-Associated Urinary Tract Infection (CAUTI) : Prevention Diagnosis and ManagementTamil SelvaPas encore d'évaluation
- UTI Leaflet V16 PDFDocument1 pageUTI Leaflet V16 PDFPrecious SorianoPas encore d'évaluation
- Prudent Use of AntibioticsDocument47 pagesPrudent Use of AntibioticsJuwita Pratiwi100% (1)
- Bacteriuria Asintomatica. IDSA PDFDocument12 pagesBacteriuria Asintomatica. IDSA PDFpatricia SilvaPas encore d'évaluation
- Consumer World Amr Awareness Week 2023 Power Point PresentationDocument29 pagesConsumer World Amr Awareness Week 2023 Power Point PresentationSoha GalalPas encore d'évaluation
- A Simple Guide to Pancreatitis, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Pancreatitis, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- Post-cholecystectomy Bile Duct InjuryD'EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorPas encore d'évaluation
- Harga ObatDocument43 pagesHarga ObatAmaliahPas encore d'évaluation
- Absen AlzarDocument3 pagesAbsen AlzarAmaliahPas encore d'évaluation
- Epo TR IV Blud Rs KonselDocument48 pagesEpo TR IV Blud Rs KonselAmaliahPas encore d'évaluation
- FDocument21 pagesFFrancisco RiveraPas encore d'évaluation
- The Effect of Citicolin in Motoric Improvement of Acute Ischemic Stroke Patients in Siti Khodijah Sepanjang Hospital Original ArticleDocument7 pagesThe Effect of Citicolin in Motoric Improvement of Acute Ischemic Stroke Patients in Siti Khodijah Sepanjang Hospital Original ArticleAmaliahPas encore d'évaluation
- UTI (Catheter) : Antimicrobial PrescribingDocument3 pagesUTI (Catheter) : Antimicrobial PrescribingAmaliahPas encore d'évaluation
- Tugas Teknologi Reproduksi Ternak COVERDocument1 pageTugas Teknologi Reproduksi Ternak COVERAmaliahPas encore d'évaluation
- Daftar Harga Obat Pt. Infion 2019 Oral NO Produk Komposisi Kemasan HNA Hna+PpnDocument1 pageDaftar Harga Obat Pt. Infion 2019 Oral NO Produk Komposisi Kemasan HNA Hna+PpnAmaliahPas encore d'évaluation
- Epo TR IV Blud Rs KonselDocument48 pagesEpo TR IV Blud Rs KonselAmaliahPas encore d'évaluation
- Lion Air Eticket Itinerary / Receipt: Fauziah/Amaliah MsDocument4 pagesLion Air Eticket Itinerary / Receipt: Fauziah/Amaliah MsAmaliahPas encore d'évaluation
- Window ('Google - Empty - Script - Included') TrueDocument1 pageWindow ('Google - Empty - Script - Included') TrueAmaliahPas encore d'évaluation
- Guia Canadiense HtaDocument20 pagesGuia Canadiense HtaLuis H. NarváezPas encore d'évaluation
- Guideline HIV PDFDocument430 pagesGuideline HIV PDFReza Affandi MohamadPas encore d'évaluation
- Persediaan Dan Distribusi Obat Anti Virus Daerah PandemikDocument9 pagesPersediaan Dan Distribusi Obat Anti Virus Daerah PandemikSiti Zamilatul AzkiyahPas encore d'évaluation
- Typhoid Fever (Salmonella Typhi) Investigation GuidelineDocument15 pagesTyphoid Fever (Salmonella Typhi) Investigation GuidelineAmaliahPas encore d'évaluation
- Persediaan Dan Distribusi Obat Anti Virus Daerah PandemikDocument9 pagesPersediaan Dan Distribusi Obat Anti Virus Daerah PandemikSiti Zamilatul AzkiyahPas encore d'évaluation
- Typhoid Fever Disease Investigation GuidelineDocument7 pagesTyphoid Fever Disease Investigation GuidelineAmaliahPas encore d'évaluation
- Typhoid Fever (Salmonella Typhi) Investigation GuidelineDocument15 pagesTyphoid Fever (Salmonella Typhi) Investigation GuidelineAmaliahPas encore d'évaluation
- UTI (Lower) : Antimicrobial Prescribing: Non-Pregnant WomanDocument3 pagesUTI (Lower) : Antimicrobial Prescribing: Non-Pregnant WomanAmaliahPas encore d'évaluation
- Urinary TR Urinary Tract Infection (Recurrent) : Act Infection (Recurrent) : Antimicrobial Prescribing Antimicrobial PrescribingDocument32 pagesUrinary TR Urinary Tract Infection (Recurrent) : Act Infection (Recurrent) : Antimicrobial Prescribing Antimicrobial PrescribingAmaliahPas encore d'évaluation
- S 055 LBLDocument14 pagesS 055 LBLFranz Josef TariganPas encore d'évaluation
- UTI (Catheter) : Antimicrobial PrescribingDocument3 pagesUTI (Catheter) : Antimicrobial PrescribingAmaliahPas encore d'évaluation
- India Immunization Chart 2010Document1 pageIndia Immunization Chart 2010Sarath Nageshwaran SujathaPas encore d'évaluation
- Curriculum Vitae of Professor Francesco RiaDocument9 pagesCurriculum Vitae of Professor Francesco RianoncanimussurdisPas encore d'évaluation
- PTSD and Special Operations ForcesDocument4 pagesPTSD and Special Operations ForcessolsysPas encore d'évaluation
- FFT Neuroma Morton PDFDocument6 pagesFFT Neuroma Morton PDFdasamoroPas encore d'évaluation
- ACG and CAG Clinical GuidelineDocument2 pagesACG and CAG Clinical GuidelineNabila IsnainiPas encore d'évaluation
- Dialog Roleplay Bahasa Inggris: Disusun Oleh Kelompok 3Document4 pagesDialog Roleplay Bahasa Inggris: Disusun Oleh Kelompok 3Desma LindaPas encore d'évaluation
- Laminectomy Definition: Spine Surgery to Relieve Pressure on Spinal Cord or NervesDocument9 pagesLaminectomy Definition: Spine Surgery to Relieve Pressure on Spinal Cord or NervesEdmarie AmistadPas encore d'évaluation
- Biosensors 12 00985 v2Document30 pagesBiosensors 12 00985 v2aqsa javedPas encore d'évaluation
- OtrivinDocument12 pagesOtrivinkanika sengarPas encore d'évaluation
- File PDFDocument6 pagesFile PDFJulenda CintarinovaPas encore d'évaluation
- Crystalloid and Colloid TherapyDocument11 pagesCrystalloid and Colloid TherapyAlexa UGPas encore d'évaluation
- Poster PresentationDocument1 pagePoster PresentationVency KatiraPas encore d'évaluation
- Sanaani, Wallie Jr.Document10 pagesSanaani, Wallie Jr.Nur SetsuPas encore d'évaluation
- Cam4 5 1239Document12 pagesCam4 5 1239kadiksuhPas encore d'évaluation
- Bipolar Versus Borderline Difference Matter Acta PsychDocument2 pagesBipolar Versus Borderline Difference Matter Acta PsychSalud Mental SantiagoPas encore d'évaluation
- RADIOLOGYDocument3 pagesRADIOLOGYwendy carinoPas encore d'évaluation
- 2016 - Byk FotoDocument7 pages2016 - Byk FotoSyifa IKPas encore d'évaluation
- The Microbial World & You: NomenclatureDocument9 pagesThe Microbial World & You: NomenclatureApryll DarlinePas encore d'évaluation
- 9503 Duodenal AtresiaDocument2 pages9503 Duodenal Atresiamudasir61Pas encore d'évaluation
- Abdominal Distension: Supervised BY: Done BYDocument4 pagesAbdominal Distension: Supervised BY: Done BYŽäíñäb ÄljaÑabìPas encore d'évaluation
- NG Pháp Trang 8Document4 pagesNG Pháp Trang 8Thithanhkieu TranPas encore d'évaluation
- Secretin Hormone Activates Satiation by Triggering Brown FatDocument1 pageSecretin Hormone Activates Satiation by Triggering Brown FatTalal ZariPas encore d'évaluation
- Addiction CaseDocument4 pagesAddiction CasePooja VarmaPas encore d'évaluation
- Arthrogryposis Multiplex Congenita (AMC) in Siblings - Case Report. First DCMS Annual Research Day, April 7, 2018Document8 pagesArthrogryposis Multiplex Congenita (AMC) in Siblings - Case Report. First DCMS Annual Research Day, April 7, 2018Razi MohdPas encore d'évaluation
- Bill Receipt for Super Extn Health Male TestDocument1 pageBill Receipt for Super Extn Health Male TestSiddhant choudharyPas encore d'évaluation
- Anti-Allergy Drug GuidelinesDocument8 pagesAnti-Allergy Drug GuidelinesYojna PatilPas encore d'évaluation
- Antimicrobial Mouthwash - Google SearchDocument1 pageAntimicrobial Mouthwash - Google Searchbruce kPas encore d'évaluation