Vous aimerez peut-être aussi
- Health Insurance Fronter Script 3.5Document3 pagesHealth Insurance Fronter Script 3.5Jolly Silastre100% (2)
- Med Surg FlashcardsDocument212 pagesMed Surg FlashcardsLaura Urieta100% (31)
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsD'EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsPas encore d'évaluation
- Medicare Part DDocument2 pagesMedicare Part DArnold VenturesPas encore d'évaluation
- Medical BillDocument1 pageMedical BillRabindra P.Singh50% (2)
- MedicaidDocument82 pagesMedicaiddrrskhan100% (2)
- Insurance Cheat Sheet CVSDocument2 pagesInsurance Cheat Sheet CVSTanyaTouché100% (5)
- Rapidcare Medical Billing ManualDocument93 pagesRapidcare Medical Billing Manualapi-19789919100% (3)
- Group Health, Inc. Part Iii: Actuarial Memorandum Healthpartners Individual Policies Policy Number: Con-103.5 Ghi IndDocument15 pagesGroup Health, Inc. Part Iii: Actuarial Memorandum Healthpartners Individual Policies Policy Number: Con-103.5 Ghi IndJill BurcumPas encore d'évaluation
- Announcement2019 PDFDocument270 pagesAnnouncement2019 PDFHarsha VipinPas encore d'évaluation
- Medicare Is Not BankruptDocument3 pagesMedicare Is Not BankruptMustaffah KabelyyonPas encore d'évaluation
- Department of Health & Human ServicesDocument31 pagesDepartment of Health & Human ServicesBrian AhierPas encore d'évaluation
- OACT Memorandum On Financial Impact of H R 3962 11-13-09 NoPWDocument31 pagesOACT Memorandum On Financial Impact of H R 3962 11-13-09 NoPWthecynicaleconomistPas encore d'évaluation
- AV Comment Letter On 2024 MA Advance Notice FINALDocument5 pagesAV Comment Letter On 2024 MA Advance Notice FINALArnold VenturesPas encore d'évaluation
- KPMG Macra Brief - FinalDocument6 pagesKPMG Macra Brief - FinalrsumnerwhitePas encore d'évaluation
- Projected Medicare Expenditures Under An Illustrative Scenario With Alternative Payment Updates To Medicare ProvidersDocument18 pagesProjected Medicare Expenditures Under An Illustrative Scenario With Alternative Payment Updates To Medicare ProvidersTed OkonPas encore d'évaluation
- Office of The Actuary DATE: April 22, 2010 FROM: Solomon M. Mussey SUBJECT: Estimated Effects of The "Patient Protection and Affordable Care Act,"Document3 pagesOffice of The Actuary DATE: April 22, 2010 FROM: Solomon M. Mussey SUBJECT: Estimated Effects of The "Patient Protection and Affordable Care Act,"api-25909546Pas encore d'évaluation
- Announcement 2020Document242 pagesAnnouncement 2020Saifuddin SidikiPas encore d'évaluation
- The Impact of The ACA and The Exchange On Minnesota: Updated EstimatesDocument25 pagesThe Impact of The ACA and The Exchange On Minnesota: Updated EstimatesMinnesota Public RadioPas encore d'évaluation
- Letter of Support For ACOs and MSSP NPRM Sign On 09202018Document3 pagesLetter of Support For ACOs and MSSP NPRM Sign On 09202018HLMeditPas encore d'évaluation
- What To Expect in Us Healthcare in 2023 and Beyond PDFDocument10 pagesWhat To Expect in Us Healthcare in 2023 and Beyond PDFSowmya MuraliPas encore d'évaluation
- 2018 Medicare Physician Fee Schedule SLPDocument14 pages2018 Medicare Physician Fee Schedule SLPAnonymous WpMUZCb935Pas encore d'évaluation
- CBO Correction of Long-Term Deficit SavingsDocument3 pagesCBO Correction of Long-Term Deficit SavingsMarkWarnerPas encore d'évaluation
- EL Star Ratings White Paper PDF DownloadDocument5 pagesEL Star Ratings White Paper PDF DownloadHarsh VardhanPas encore d'évaluation
- UntitledDocument16 pagesUntitledapi-227433089Pas encore d'évaluation
- HCC Computation ManualDocument195 pagesHCC Computation Manualykbhaumik123Pas encore d'évaluation
- Medigap John RadinDocument12 pagesMedigap John Radinjohnnyerstwild1393Pas encore d'évaluation
- Social Security Trustees Report 2010Document20 pagesSocial Security Trustees Report 2010Beverly TranPas encore d'évaluation
- Summary of 2020 Changes To The Medicare Physician Fee Schedule, Quality Payment Program, and Other Federal ProgramsDocument25 pagesSummary of 2020 Changes To The Medicare Physician Fee Schedule, Quality Payment Program, and Other Federal ProgramsJared DeraneyPas encore d'évaluation
- Medicaid: Health Policy BriefDocument2 pagesMedicaid: Health Policy BriefArnold VenturesPas encore d'évaluation
- Cost of The Future Newly Insured Under The Affordable Care ActDocument83 pagesCost of The Future Newly Insured Under The Affordable Care ActpoorrichardsnewsPas encore d'évaluation
- Trends in Healthcare Payments Annual Report 2015 PDFDocument38 pagesTrends in Healthcare Payments Annual Report 2015 PDFAnonymous Feglbx5Pas encore d'évaluation
- Ib 33 PDFDocument12 pagesIb 33 PDFLatinos Ready To VotePas encore d'évaluation
- Engaging Commercial Payers On Multi-Payer Alignment:: Key Issues For SIM StatesDocument8 pagesEngaging Commercial Payers On Multi-Payer Alignment:: Key Issues For SIM StatesSHADACPas encore d'évaluation
- Data Point: Individual Market Premium Changes: 2013 - 2017Document5 pagesData Point: Individual Market Premium Changes: 2013 - 2017ZerohedgePas encore d'évaluation
- Value Based ProgramsDocument8 pagesValue Based ProgramsPremium GeeksPas encore d'évaluation
- Cheat Sheet Series Medicare Part C Medicare AdvantageDocument2 pagesCheat Sheet Series Medicare Part C Medicare AdvantageGirish KaimalPas encore d'évaluation
- Mac Guineas Testimony Medicare Reform 12oct11Document12 pagesMac Guineas Testimony Medicare Reform 12oct11Committee For a Responsible Federal BudgetPas encore d'évaluation
- Jun 10 Data Book Sec 10Document12 pagesJun 10 Data Book Sec 10Nman12Pas encore d'évaluation
- Medicare Table of Reform Proposals 2 0518Document1 pageMedicare Table of Reform Proposals 2 0518mng1mng1Pas encore d'évaluation
- QMB Billing ProhibitionDocument6 pagesQMB Billing ProhibitionWill Blueotter AndersonPas encore d'évaluation
- Social Security and Medicare Trustees ReportDocument28 pagesSocial Security and Medicare Trustees ReportAustin DeneanPas encore d'évaluation
- 2023.justification - BCI .SGDocument2 pages2023.justification - BCI .SGRaja Churchill DassPas encore d'évaluation
- ActmemosmgrpDocument3 pagesActmemosmgrpapi-373105184Pas encore d'évaluation
- Hmo Msa OverviewDocument28 pagesHmo Msa Overviewmamatha mamtaPas encore d'évaluation
- MEABF Plan Design Scenarios - September 6, 2016Document8 pagesMEABF Plan Design Scenarios - September 6, 2016The Daily LinePas encore d'évaluation
- Trustees PaperDocument6 pagesTrustees PaperCommittee For a Responsible Federal BudgetPas encore d'évaluation
- Top Global Risks: Illuminating The IN 2020Document12 pagesTop Global Risks: Illuminating The IN 2020Mohammed OsmanPas encore d'évaluation
- Health Affairs Medicare's New Physician Payment System PDFDocument7 pagesHealth Affairs Medicare's New Physician Payment System PDFiggybauPas encore d'évaluation
- Fact Sheet - Health Care - FINALDocument6 pagesFact Sheet - Health Care - FINALsarahkliffPas encore d'évaluation
- Romney Budget Proposals Would Necessitate Very Large Cuts in Medicaid, Education, Health Research, and Other ProgramsDocument11 pagesRomney Budget Proposals Would Necessitate Very Large Cuts in Medicaid, Education, Health Research, and Other ProgramsJamie SandersonPas encore d'évaluation
- 2023 Medicare Fee Schedule For SlpsDocument23 pages2023 Medicare Fee Schedule For SlpsLeon DaleyPas encore d'évaluation
- ACOS An Eye On Washington Quarterly (SGR)Document3 pagesACOS An Eye On Washington Quarterly (SGR)acosurgeryPas encore d'évaluation
- GNYHA Memo New York State Budget 2012Document12 pagesGNYHA Memo New York State Budget 2012ahawkins2865Pas encore d'évaluation
- Transition To ValueDocument19 pagesTransition To ValueMark Philipp AbanPas encore d'évaluation
- Comparing Medicare Reform ProposalsDocument1 pageComparing Medicare Reform ProposalsDonald SjoerdsmaPas encore d'évaluation
- Preparing For The Next Generation of Managed Care ContractingDocument21 pagesPreparing For The Next Generation of Managed Care ContractingVaibhav RaiPas encore d'évaluation
- Centers For Medicare and Medicaid Services: Term PaperDocument20 pagesCenters For Medicare and Medicaid Services: Term PaperMatt SzybalskiPas encore d'évaluation
- Accenture Drowning in Bad DebtDocument4 pagesAccenture Drowning in Bad DebtAnna NguyenPas encore d'évaluation
- Final Report - New Jersey Pension and Health Benefit Study Commission - Dec. 6, 2017Document10 pagesFinal Report - New Jersey Pension and Health Benefit Study Commission - Dec. 6, 2017The (Bergen) RecordPas encore d'évaluation
- 2015 Anthem Small Group 4-1-2015 Rate Filing PDFDocument40 pages2015 Anthem Small Group 4-1-2015 Rate Filing PDFmoconsumerPas encore d'évaluation
- CBO Cost Estimate For H.R. 1628 Obamacare Repeal Reconciliation Act of 2017Document19 pagesCBO Cost Estimate For H.R. 1628 Obamacare Repeal Reconciliation Act of 2017CNBC.comPas encore d'évaluation
- Medicare Revolution: Profiting from Quality, Not QuantityD'EverandMedicare Revolution: Profiting from Quality, Not QuantityPas encore d'évaluation
- Summary, Analysis & Review of Philip Moeller’s Get What’s Yours for MedicareD'EverandSummary, Analysis & Review of Philip Moeller’s Get What’s Yours for MedicarePas encore d'évaluation
- Textbook of Urgent Care Management: Chapter 38, Audits by Managed-Care Organizations and Regulatory AgenciesD'EverandTextbook of Urgent Care Management: Chapter 38, Audits by Managed-Care Organizations and Regulatory AgenciesPas encore d'évaluation
- 50 Draude Klumbyte Luecking Treusch - 2020Document19 pages50 Draude Klumbyte Luecking Treusch - 2020khyati123Pas encore d'évaluation
- 18-Noble-Social Choice in Machine DesignDocument9 pages18-Noble-Social Choice in Machine Designkhyati123Pas encore d'évaluation
- 56 - Baumer Et Al.-On The Importance of Studying Technology Non UseDocument5 pages56 - Baumer Et Al.-On The Importance of Studying Technology Non Usekhyati123Pas encore d'évaluation
- ZuboffDocument20 pagesZuboffJosé Enrique Alcalá CamposPas encore d'évaluation
- 53 CampoloandCrawford2020Document19 pages53 CampoloandCrawford2020khyati123Pas encore d'évaluation
- 57 - Plaut 2015 - Technologies of Avoidance - The Swear Jar and The Cell PhoneDocument27 pages57 - Plaut 2015 - Technologies of Avoidance - The Swear Jar and The Cell Phonekhyati123Pas encore d'évaluation
- 35 - Kendall Etal. - Understanding - Technology - As - Situated - Practice - EverDocument22 pages35 - Kendall Etal. - Understanding - Technology - As - Situated - Practice - Everkhyati123Pas encore d'évaluation
- 4 Williams TechAndSociety TelevisionDocument7 pages4 Williams TechAndSociety Televisionkhyati123Pas encore d'évaluation
- 34 - Orlikowski-Sociomaterial PracticesDocument15 pages34 - Orlikowski-Sociomaterial Practiceskhyati123Pas encore d'évaluation
- Pci OthDocument100 pagesPci Othkhyati123Pas encore d'évaluation
- Ba Yes Intro Class Epi 515Document43 pagesBa Yes Intro Class Epi 515ruygarcia75Pas encore d'évaluation
- The Wealth Report 2014Document34 pagesThe Wealth Report 2014millian0987Pas encore d'évaluation
- Beracha Et Al-2018-Real Estate EconomicsDocument43 pagesBeracha Et Al-2018-Real Estate Economicskhyati123Pas encore d'évaluation
- Draft Task Force Report On Promoting Affordable HousingDocument100 pagesDraft Task Force Report On Promoting Affordable Housingkhyati123Pas encore d'évaluation
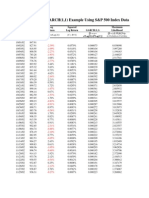
- GARCH (1,1) Example Using S&P 500 Index Data On 10/1/02 To 9/28/07Document54 pagesGARCH (1,1) Example Using S&P 500 Index Data On 10/1/02 To 9/28/07rdixit2Pas encore d'évaluation
- 3 Kenkel Hannah 2021 BS STSResearchPaperDocument16 pages3 Kenkel Hannah 2021 BS STSResearchPaperkhyati123Pas encore d'évaluation
- Bayes and Frequentism: Return of An Old Controversy: Louis LyonsDocument40 pagesBayes and Frequentism: Return of An Old Controversy: Louis Lyonskhyati123Pas encore d'évaluation
- House Price Indices in India - 2015Document48 pagesHouse Price Indices in India - 2015khyati123Pas encore d'évaluation
- Analysing Urban Growth Boundary Effects in The City of BengaluruDocument21 pagesAnalysing Urban Growth Boundary Effects in The City of Bengalurukhyati123Pas encore d'évaluation
- Garage On WebDocument174 pagesGarage On Webkhyati123Pas encore d'évaluation
- Garage On WebDocument174 pagesGarage On Webkhyati123Pas encore d'évaluation
- Urban Studies: Auctions and Land Values: An Experimental AnalysisDocument16 pagesUrban Studies: Auctions and Land Values: An Experimental Analysiskhyati123Pas encore d'évaluation
- BCA Sustainable MaterialDocument72 pagesBCA Sustainable MaterialSoo LingPas encore d'évaluation
- Mcgee 1986 SMJDocument21 pagesMcgee 1986 SMJkhyati123Pas encore d'évaluation
- INDIA - Key Indicators-HCE 66th Rd-ReportDocument191 pagesINDIA - Key Indicators-HCE 66th Rd-ReportmadhurimgPas encore d'évaluation
- Internet FraudDocument22 pagesInternet Fraudkhyati123Pas encore d'évaluation
- Human World Case Study Revision SessionDocument21 pagesHuman World Case Study Revision Sessionkhyati123Pas encore d'évaluation
- Bbmpfinal MTFPDocument46 pagesBbmpfinal MTFPkhyati123Pas encore d'évaluation
- Acornredecom 2010 OkelloDocument10 pagesAcornredecom 2010 Okellokhyati123Pas encore d'évaluation
- KombiglyzeXR Savings CardDocument1 pageKombiglyzeXR Savings CardRodolfo ArangoPas encore d'évaluation
- Face To Face Encounter Form PDFDocument2 pagesFace To Face Encounter Form PDFLisaPas encore d'évaluation
- Phoenix House Topcliffe Lane Tingley Wakefield WF3 1WEDocument7 pagesPhoenix House Topcliffe Lane Tingley Wakefield WF3 1WEfugzMabugzPas encore d'évaluation
- InstituitionalDocument12 pagesInstituitionalSamhitha Ayurvedic ChennaiPas encore d'évaluation
- Healthcare BasicsDocument57 pagesHealthcare BasicsManickavel Manoharan100% (2)
- Muthoot Health GuardDocument4 pagesMuthoot Health GuarddhavaldadhaniaPas encore d'évaluation
- ACO Advance Payment Factsheet ICN907403Document8 pagesACO Advance Payment Factsheet ICN907403pultPas encore d'évaluation
- Ismh Cutoff GenDocument4 pagesIsmh Cutoff GenAshutosh Singh ParmarPas encore d'évaluation
- 2013 Scope of Appointment Form - CORBINDocument2 pages2013 Scope of Appointment Form - CORBINCorbin LindseyPas encore d'évaluation
- Rakta MokshaDocument60 pagesRakta MokshaAswathy KumaranPas encore d'évaluation
- Discharge Planning ChecklistDocument6 pagesDischarge Planning ChecklistcutevivesPas encore d'évaluation
- Schneider 2017Document3 pagesSchneider 2017ali razaPas encore d'évaluation
- Medicare Part B Help ProgramDocument2 pagesMedicare Part B Help ProgramGemini JonesPas encore d'évaluation
- Ayushman BharatDocument19 pagesAyushman Bharatannu panchalPas encore d'évaluation
- Donut Hole LetterDocument2 pagesDonut Hole LetterPeter SullivanPas encore d'évaluation
- 3-04 Insurance Claims ProcessDocument13 pages3-04 Insurance Claims Processabraham_sse1594Pas encore d'évaluation
- Tobradex CouponDocument1 pageTobradex CouponHani AlmuftiPas encore d'évaluation
- Covered Lives SummaryDocument8 pagesCovered Lives Summarygaurav_johnPas encore d'évaluation
- Medical RealDocument1 pageMedical Realapi-252555369Pas encore d'évaluation
- Anthem Scope of App.Document2 pagesAnthem Scope of App.family-institutePas encore d'évaluation
- Michigan Inpatient Payment ReductionDocument7 pagesMichigan Inpatient Payment ReductionBeverly TranPas encore d'évaluation
- Suggestions For Health Care PolicyDocument1 pageSuggestions For Health Care PolicyMushtaq AhmadPas encore d'évaluation
- 1-15 A12060 HMO Manual PDFDocument460 pages1-15 A12060 HMO Manual PDFsyunamiPas encore d'évaluation
- Samaritan Summit Village Announces Leadership ChangesDocument1 pageSamaritan Summit Village Announces Leadership ChangesNewzjunkyPas encore d'évaluation