Vous aimerez peut-être aussi
- Healers Versus Stealers: How to Outsmart the Thief in Your Dental PracticeD'EverandHealers Versus Stealers: How to Outsmart the Thief in Your Dental PracticePas encore d'évaluation
- An Ounce of Prevention Is Worth A Pound of Cure: Ergonomics in Dental PracticeDocument6 pagesAn Ounce of Prevention Is Worth A Pound of Cure: Ergonomics in Dental Practicetri wahyuniPas encore d'évaluation
- Operator Chair PositionsDocument21 pagesOperator Chair PositionsParidhi GargPas encore d'évaluation
- Caries and Quality of Life in Portuguese Adolescents: Impact of Diet and Behavioural Risk FactorsDocument6 pagesCaries and Quality of Life in Portuguese Adolescents: Impact of Diet and Behavioural Risk FactorsCristian OneaPas encore d'évaluation
- Common Mistakes in Clinical Dental PracticeDocument80 pagesCommon Mistakes in Clinical Dental PracticeRohit ShahPas encore d'évaluation
- Seminar 6 Preventive Prosthodontics in CD WordDocument29 pagesSeminar 6 Preventive Prosthodontics in CD Wordketaki kuntePas encore d'évaluation
- Info Immediate DenturesDocument4 pagesInfo Immediate DenturesDyah Wulan RamadhaniPas encore d'évaluation
- 2014 Table Clinic InstructionsDocument19 pages2014 Table Clinic InstructionsMaria Mercedes LeivaPas encore d'évaluation
- Ethical Challenges in Aesthetic DentistryDocument21 pagesEthical Challenges in Aesthetic DentistryMkPas encore d'évaluation
- Periodontal Office Report GutierrezDocument5 pagesPeriodontal Office Report Gutierrezapi-673363347Pas encore d'évaluation
- Dental PhotographyDocument29 pagesDental Photographyali50% (2)
- Diagnosis and Treatment Planning of Fixed ProsthodonticDocument15 pagesDiagnosis and Treatment Planning of Fixed ProsthodonticM.R PsychopathPas encore d'évaluation
- Working Length DeterminationDocument97 pagesWorking Length Determinationrolly_jatinPas encore d'évaluation
- TRANSFER INSTRUMENT FHD PDFDocument12 pagesTRANSFER INSTRUMENT FHD PDFRadikaPas encore d'évaluation
- Dental Foundation Training Curriculum 2016Document46 pagesDental Foundation Training Curriculum 2016Rajitha Dilhan100% (1)
- Guide To Writing Good MCQs-1Document4 pagesGuide To Writing Good MCQs-1Ambika Suwal100% (1)
- Dental - Manikin Manual 2021Document35 pagesDental - Manikin Manual 2021AmariesaPas encore d'évaluation
- CDT 2011 Chapter5Document45 pagesCDT 2011 Chapter5Asadulla KhanPas encore d'évaluation
- Dental InformaticsDocument13 pagesDental Informaticsho laPas encore d'évaluation
- Partial Dentures PDFDocument1 pagePartial Dentures PDFGabriela ArgeseanuPas encore d'évaluation
- Digital Smile Design: A Tool For Treatment Planning and Communication in Esthetic DentistryDocument10 pagesDigital Smile Design: A Tool For Treatment Planning and Communication in Esthetic Dentistrygilberto69Pas encore d'évaluation
- Cosmetic Dentistry & Aesthetic Restorative Dentistry: Comprehensive One-Year CourseDocument21 pagesCosmetic Dentistry & Aesthetic Restorative Dentistry: Comprehensive One-Year CourseMariusNOPas encore d'évaluation
- Dental Lab CommunicationDocument3 pagesDental Lab Communicationkhaled alahmad100% (1)
- Oral Diagnosis and Treatment Plannin PDFDocument8 pagesOral Diagnosis and Treatment Plannin PDFTeguh CaninusPas encore d'évaluation
- Dental Hygiene ProposalDocument9 pagesDental Hygiene Proposalmoses njengaPas encore d'évaluation
- TR Dental Laboratory Technology Services (Removable) NC IIDocument70 pagesTR Dental Laboratory Technology Services (Removable) NC IIFrancis Rico Mutia RufonPas encore d'évaluation
- Clinical Practice Guidelines Approved 2021 HODDocument57 pagesClinical Practice Guidelines Approved 2021 HODNovaira WaseemPas encore d'évaluation
- Dentalmanpower 161116120715Document67 pagesDentalmanpower 161116120715tannguyen1103Pas encore d'évaluation
- CAD CAmDocument62 pagesCAD CAmAlex Iliescu0% (1)
- Smile Design GuideDocument13 pagesSmile Design Guideartwrk80Pas encore d'évaluation
- A A D W - Up: N Dvanced Iagnostic AxDocument4 pagesA A D W - Up: N Dvanced Iagnostic AxjoephinPas encore d'évaluation
- Dental Office Specialty Observation Brianna MeyersDocument4 pagesDental Office Specialty Observation Brianna Meyersapi-499228834100% (1)
- IMPLANTOLOGI Compressed Compressed (1) - MinDocument122 pagesIMPLANTOLOGI Compressed Compressed (1) - MinNayafilahPas encore d'évaluation
- Dental Assisting ProgramsDocument4 pagesDental Assisting ProgramsJuan EstebanPas encore d'évaluation
- Dental Lab ReportDocument10 pagesDental Lab ReportAbdu AbdoulayePas encore d'évaluation
- Goldstein Re Esthetics in DentistryDocument3 pagesGoldstein Re Esthetics in DentistryMichaelPas encore d'évaluation
- ANKYLOS Laboratory ManualDocument100 pagesANKYLOS Laboratory ManualheycoolalexPas encore d'évaluation
- Dental Foundation Training Portfolio User GuideDocument56 pagesDental Foundation Training Portfolio User GuideEdgar PalmaPas encore d'évaluation
- Occupational Hazzard in Dental Office PDFDocument3 pagesOccupational Hazzard in Dental Office PDFtifaniPas encore d'évaluation
- Dental Assistants in OrthodonticsDocument2 pagesDental Assistants in Orthodonticsmaryam fatimaPas encore d'évaluation
- Cracked Tooth PresentationDocument36 pagesCracked Tooth Presentationmirfanulhaq100% (1)
- Adex Dental Exam Series: Fixed Prosthodontics and EndodonticsDocument36 pagesAdex Dental Exam Series: Fixed Prosthodontics and EndodonticsmeethaileyyyPas encore d'évaluation
- Teaching Clinically Relevant Dental Anatomy in The Dental CurriculumDocument9 pagesTeaching Clinically Relevant Dental Anatomy in The Dental CurriculumEmanuel VallejoPas encore d'évaluation
- 5 Steps To A Successful Dental PracticeDocument22 pages5 Steps To A Successful Dental PracticeVasile FlorinPas encore d'évaluation
- Dental Auxiliary: Presented By-Sneha Patil (Final Year BDS Student)Document36 pagesDental Auxiliary: Presented By-Sneha Patil (Final Year BDS Student)Mumin RashidPas encore d'évaluation
- Erosion Abrasion Attrition and Abfrcation1Erosion Abrasion Attrition and Abfrcation1Document82 pagesErosion Abrasion Attrition and Abfrcation1Erosion Abrasion Attrition and Abfrcation1Madalina A DobrePas encore d'évaluation
- Causes of Endodontic FailuresDocument8 pagesCauses of Endodontic Failuresizeldien5870Pas encore d'évaluation
- Ethics Lec 1Document9 pagesEthics Lec 1Prince AhmedPas encore d'évaluation
- Bonnick - 2011 - Dental Clinics of North America PDFDocument14 pagesBonnick - 2011 - Dental Clinics of North America PDFKranti PrajapatiPas encore d'évaluation
- 1 s2.0 S0022391302002998 MainDocument5 pages1 s2.0 S0022391302002998 MainManjeev GuragainPas encore d'évaluation
- Infection Prevention Checklist For Dental Setting - CDCDocument20 pagesInfection Prevention Checklist For Dental Setting - CDCDewi Ratna Sari100% (1)
- CHAPTER 1 Manual OperativeDocument27 pagesCHAPTER 1 Manual OperativeCassie Von PeenqPas encore d'évaluation
- Vsip - Info - Anterior Wax Up PDF Free PDFDocument3 pagesVsip - Info - Anterior Wax Up PDF Free PDFMekideche dental officePas encore d'évaluation
- Instrument Processing, Work Flow and Sterility Assurance: 4 CE CreditsDocument12 pagesInstrument Processing, Work Flow and Sterility Assurance: 4 CE Creditsdruzair007Pas encore d'évaluation
- Dental Laboratory Infection ControlDocument6 pagesDental Laboratory Infection ControlDrShweta SainiPas encore d'évaluation
- 3501029Document5 pages3501029Anil NepalPas encore d'évaluation
- Emergency Drugs Poster - Layout 1 in Dental PracticeDocument1 pageEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefPas encore d'évaluation
- Geriatric Dentistry: Caring for Our Aging PopulationD'EverandGeriatric Dentistry: Caring for Our Aging PopulationPas encore d'évaluation
- Set Furtun Easy Garden 1Document2 pagesSet Furtun Easy Garden 1manupopPas encore d'évaluation
- Directions RetetaDocument1 pageDirections RetetamanupopPas encore d'évaluation
- Model MacaraDocument34 pagesModel Macaravoicumarian1958Pas encore d'évaluation
- Welcome Friends FaDocument3 pagesWelcome Friends FamanupopPas encore d'évaluation
- Harta RomanieiDocument1 pageHarta RomanieiCatalin Craciun100% (3)
- Produse Noi Micromot 2010Document6 pagesProduse Noi Micromot 2010manupopPas encore d'évaluation
- Scroll SawDocument14 pagesScroll SawmanupopPas encore d'évaluation
- Calendar Mic Triptic Spiralat 55x105Document13 pagesCalendar Mic Triptic Spiralat 55x105manupopPas encore d'évaluation
- Acdsee Pro 5 End User License AgreementDocument7 pagesAcdsee Pro 5 End User License AgreementlesmosPas encore d'évaluation
- STDocument1 pageSTAdhitya NugrahaPas encore d'évaluation
- STDocument1 pageSTAdhitya NugrahaPas encore d'évaluation
- Post Crossing Post Crossing Is A ProjectDocument1 pagePost Crossing Post Crossing Is A Projectapi-25917760Pas encore d'évaluation
- PDFSigQFormalRep PDFDocument1 pagePDFSigQFormalRep PDFJim LeePas encore d'évaluation
- A History of Fish Glue As An Artist's MaterialDocument6 pagesA History of Fish Glue As An Artist's Materialmanupop100% (1)
- Detoxifier e ADocument1 pageDetoxifier e AmanupopPas encore d'évaluation
- Efficiency Energy: Technical SpecificationsDocument2 pagesEfficiency Energy: Technical SpecificationsmanupopPas encore d'évaluation
- Home Made Scroll Saw Part 1Document10 pagesHome Made Scroll Saw Part 1Randall A Jara ArroyoPas encore d'évaluation
- Familia PDFDocument85 pagesFamilia PDFKatherine BlakePas encore d'évaluation
- Capturing HeatDocument36 pagesCapturing HeatOrto di Carta100% (9)
- Life in The Backwoods A Guide To Successful Hunting Trapping 1875Document36 pagesLife in The Backwoods A Guide To Successful Hunting Trapping 1875manupopPas encore d'évaluation
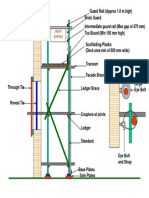
- Construction Independent Tied ScaffoldDocument1 pageConstruction Independent Tied ScaffoldBogdan-Gabriel SchiopuPas encore d'évaluation
- Post Crossing Post Crossing Is A ProjectDocument1 pagePost Crossing Post Crossing Is A Projectapi-25917760Pas encore d'évaluation
- Post Crossing Post Crossing Is A ProjectDocument1 pagePost Crossing Post Crossing Is A Projectapi-25917760Pas encore d'évaluation
- Life in The Backwoods A Guide To Successful Hunting Trapping 1875Document36 pagesLife in The Backwoods A Guide To Successful Hunting Trapping 1875manupopPas encore d'évaluation
- Advanced Organizer Chapter 2Document2 pagesAdvanced Organizer Chapter 2manupopPas encore d'évaluation
- UntitledDocument6 pagesUntitledapi-132400463Pas encore d'évaluation
- Cool FrostDocument39 pagesCool FrostmanupopPas encore d'évaluation
- Principles of Management and Organisation BehaviourDocument329 pagesPrinciples of Management and Organisation Behaviourapi-1975688692% (62)
- Harta RomanieiDocument1 pageHarta RomanieiCatalin Craciun100% (3)
- Green Smoothie Recipe EbookDocument12 pagesGreen Smoothie Recipe EbookMichael PippettPas encore d'évaluation
- 03 Orlando D. Garcia, JR., Et Al. vs. Ranida Salvador, Et Al.Document2 pages03 Orlando D. Garcia, JR., Et Al. vs. Ranida Salvador, Et Al.Raj AtmanPas encore d'évaluation
- Slides Ethical Considerations of Pharma MarketingDocument31 pagesSlides Ethical Considerations of Pharma Marketingkhizer iqbalPas encore d'évaluation
- Ethics Gtu 301 Final Exam.14.15 1Document2 pagesEthics Gtu 301 Final Exam.14.15 1JebatAl-KelantaniPas encore d'évaluation
- 10 Critical Care PDF FreeDocument3 pages10 Critical Care PDF FreeAdnene TouatiPas encore d'évaluation
- Anatomy ObeDocument13 pagesAnatomy ObeRodel AgapitoPas encore d'évaluation
- Dosage Lec - Unit 2 Drug DiscoveryDocument8 pagesDosage Lec - Unit 2 Drug DiscoveryJohn Lorenz BordadorPas encore d'évaluation
- Sickle CellDocument21 pagesSickle CellLeon0% (1)
- Lecture Notes For Internal MedicineDocument3 pagesLecture Notes For Internal MedicineMedical Lectures100% (1)
- InterRAI Community Health Assessment (CHA)Document10 pagesInterRAI Community Health Assessment (CHA)Mike F MartelliPas encore d'évaluation
- Rashtriya Bal Swasthya Karykram (RBSK) : Answer All QuestionsDocument4 pagesRashtriya Bal Swasthya Karykram (RBSK) : Answer All Questionspvaibhav08Pas encore d'évaluation
- Principles of Capture - PrintableDocument51 pagesPrinciples of Capture - PrintableNguyen Thi Phuong NhiPas encore d'évaluation
- Universal Free Reiki PDFDocument4 pagesUniversal Free Reiki PDFSabiduria Pura100% (1)
- Platinum Gazette 11 JuneDocument16 pagesPlatinum Gazette 11 JuneAnonymous w8NEyXPas encore d'évaluation
- AntihistaminesDocument2 pagesAntihistaminesmercywicherPas encore d'évaluation
- Medical Ethics More Than Hundred CasesDocument33 pagesMedical Ethics More Than Hundred Caseskrebkreb100% (4)
- Shock Study Guide NursingDocument4 pagesShock Study Guide NursingKory Christina100% (2)
- FY10 ICD-9-CM Procedure Codes Linked To NHSN Operative Procedure CategoriesDocument22 pagesFY10 ICD-9-CM Procedure Codes Linked To NHSN Operative Procedure CategoriesYohan Julian Mega NandaPas encore d'évaluation
- 940514-000021 Urology 1605 PDF-only PDFDocument72 pages940514-000021 Urology 1605 PDF-only PDFYuanita PurnamiPas encore d'évaluation
- MCB 11 Lab HW Kinds of PlatingDocument1 pageMCB 11 Lab HW Kinds of PlatingMaria Isabelle VillacortePas encore d'évaluation
- New International Society of Hypertension (Ish) Guidelines 2020 - January 17TH 2021Document35 pagesNew International Society of Hypertension (Ish) Guidelines 2020 - January 17TH 2021Rhama Patria100% (1)
- Producing Vibrato Naturally: How To Sing VibratoDocument4 pagesProducing Vibrato Naturally: How To Sing VibratoMarilyn MastilleroPas encore d'évaluation
- (MRCP Study Guides) S. Hughes - Complete Data Interpretation For The MRCP-Churchill Livingstone (2001)Document2 pages(MRCP Study Guides) S. Hughes - Complete Data Interpretation For The MRCP-Churchill Livingstone (2001)basocdovnch0% (1)
- Hamza DissertDocument108 pagesHamza DissertMobin Ur Rehman KhanPas encore d'évaluation
- Pharmaceuticals 11 00094Document14 pagesPharmaceuticals 11 00094CindyGaniPas encore d'évaluation
- Intro To HematologyDocument9 pagesIntro To HematologyDayledaniel SorvetoPas encore d'évaluation
- Mindray BS-120 / BS-200 / BS-300 / BS-380 / BS-400: MTD Diagnostics, SRLDocument40 pagesMindray BS-120 / BS-200 / BS-300 / BS-380 / BS-400: MTD Diagnostics, SRLCarlos SoutoPas encore d'évaluation
- Paul Krebaum Skunk Odor Removal RecipeDocument2 pagesPaul Krebaum Skunk Odor Removal Recipeozzaib100% (1)
- Timetable 1Document1 pageTimetable 1sunilbijlaniPas encore d'évaluation
- 51 Diseases of Ruminants - Dr. SulaDocument92 pages51 Diseases of Ruminants - Dr. SulaCholid MawardiPas encore d'évaluation
- EU Physiotherapy Guideline For Parkinson's DiseaseDocument29 pagesEU Physiotherapy Guideline For Parkinson's DiseaseAulia Zerlinda SyihabPas encore d'évaluation