Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- ScienceGeography3ResourceSample PDFDocument9 pagesScienceGeography3ResourceSample PDFmargantoniPas encore d'évaluation
- Hemorrhagic Conditions of Late Pregnancy Other Related Problems 1Document5 pagesHemorrhagic Conditions of Late Pregnancy Other Related Problems 1imnasPas encore d'évaluation
- IB Biology HL: 11.1 Antibody Production and VaccinationDocument7 pagesIB Biology HL: 11.1 Antibody Production and VaccinationpetraPas encore d'évaluation
- Immunology in Pregnancy & Coagulation Failure in PregnancyDocument30 pagesImmunology in Pregnancy & Coagulation Failure in PregnancySrikutty DevuPas encore d'évaluation
- Thyroglossal Duct Cysts: Anatomy, Embryology and TreatmentDocument7 pagesThyroglossal Duct Cysts: Anatomy, Embryology and TreatmentTasia RozakiahPas encore d'évaluation
- Unit 1 Anatomy, Physiology and The Human Body: Learning OutcomesDocument91 pagesUnit 1 Anatomy, Physiology and The Human Body: Learning OutcomesDeolita BadiangPas encore d'évaluation
- Connective TissuesDocument4 pagesConnective TissuesLAKHASTH JAYASILANPas encore d'évaluation
- Multiple MyelomaDocument28 pagesMultiple Myelomamedical notes100% (1)
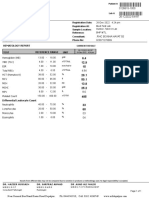
- BILAL FARID, 1 Year(s) /male: Registration Date: M.R. No: Registration At: Sample LocationDocument1 pageBILAL FARID, 1 Year(s) /male: Registration Date: M.R. No: Registration At: Sample LocationsaifPas encore d'évaluation
- Anatomy Chapters 6&7Document17 pagesAnatomy Chapters 6&7Tamara IdalyPas encore d'évaluation
- Rujukan OktoberDocument15 pagesRujukan Oktoberendang sunarmPas encore d'évaluation
- 1 Крок 1 ЛС KROK 2007 2017 English BiochemistryDocument480 pages1 Крок 1 ЛС KROK 2007 2017 English BiochemistryAbhani MøhitPas encore d'évaluation
- Homeostasis Support and Movement UHS PAST PAPERSDocument5 pagesHomeostasis Support and Movement UHS PAST PAPERSAhmad RafiquePas encore d'évaluation
- Structure of Teeth: Khushi Desai III BDS 808Document36 pagesStructure of Teeth: Khushi Desai III BDS 808Khushi DesaiPas encore d'évaluation
- Science ReviewerDocument13 pagesScience ReviewerLenie MatanguihanPas encore d'évaluation
- The Ruminant Digestive System Day 2Document18 pagesThe Ruminant Digestive System Day 2Yanyan PaydaPas encore d'évaluation
- Effect of Respiratory Obstruction On The Arterial and Venous Circulation in Animals and ManDocument11 pagesEffect of Respiratory Obstruction On The Arterial and Venous Circulation in Animals and ManlaughAndCry72Pas encore d'évaluation
- Module 5 HomeworkDocument4 pagesModule 5 HomeworkCj LincePas encore d'évaluation
- English For MedicineDocument52 pagesEnglish For MedicineRoya NaderiPas encore d'évaluation
- Embriologi Tumbuhan - Materi 2Document21 pagesEmbriologi Tumbuhan - Materi 2gahanPas encore d'évaluation
- Female Genitalia and RectumDocument3 pagesFemale Genitalia and Rectumadrian lozanoPas encore d'évaluation
- Biology IGCSE Pearson Edexcel NotesDocument11 pagesBiology IGCSE Pearson Edexcel NotesShoag Al ArakzehPas encore d'évaluation
- 5 - The Visual System and Mechanisms of PerceptionDocument13 pages5 - The Visual System and Mechanisms of PerceptionElmer SalazarPas encore d'évaluation
- Menstrual Cycle PhasesDocument2 pagesMenstrual Cycle PhasesPatricia G ChiuPas encore d'évaluation
- Chapter 35 Plant Structure Growth and DevelopmentDocument3 pagesChapter 35 Plant Structure Growth and DevelopmentmokeymonkeyPas encore d'évaluation
- Cervical and Shoulder 2020Document14 pagesCervical and Shoulder 2020Eduardo OlivaPas encore d'évaluation
- Reproductive SystemDocument49 pagesReproductive SystemAyro Business CenterPas encore d'évaluation
- Health Psychology 9th Edition Taylor Test BankDocument25 pagesHealth Psychology 9th Edition Taylor Test BankTylerDavisbzmjy100% (64)
- Human Biology - Final ProjectDocument10 pagesHuman Biology - Final Projectapi-521705699Pas encore d'évaluation
- Kuliah Biokimia-Imunokimia FK UNDIPDocument19 pagesKuliah Biokimia-Imunokimia FK UNDIPPutri HapsariPas encore d'évaluation