Vous aimerez peut-être aussi
- Historia Das Politicas de Saude No Brasil Uma Pequena Revisao Marcus Vinicius Polignano (16 200511 SES MT)Document35 pagesHistoria Das Politicas de Saude No Brasil Uma Pequena Revisao Marcus Vinicius Polignano (16 200511 SES MT)Marcelo Oliveira100% (1)
- Manual Orientações OESCE 2017Document3 pagesManual Orientações OESCE 2017Alcemir JúniorPas encore d'évaluation
- Manual Orientações OESCE 2017Document3 pagesManual Orientações OESCE 2017Alcemir JúniorPas encore d'évaluation
- Apostila de EspirometriaDocument19 pagesApostila de EspirometriaAlcemir JúniorPas encore d'évaluation
- Exercícios PonteirosDocument2 pagesExercícios PonteirosAlcemir JúniorPas encore d'évaluation
- Exercícios PonteirosDocument2 pagesExercícios PonteirosAlcemir JúniorPas encore d'évaluation
- Prepare O Seu Currículo: Saiba Como Ter Um Currículo Padrão-Ouro para Ser Requisitado Pelas Bancas de ResidênciaDocument49 pagesPrepare O Seu Currículo: Saiba Como Ter Um Currículo Padrão-Ouro para Ser Requisitado Pelas Bancas de ResidênciaAlcemir JúniorPas encore d'évaluation
- Prepare O Seu Currículo: Saiba Como Ter Um Currículo Padrão-Ouro para Ser Requisitado Pelas Bancas de ResidênciaDocument49 pagesPrepare O Seu Currículo: Saiba Como Ter Um Currículo Padrão-Ouro para Ser Requisitado Pelas Bancas de ResidênciaAlcemir JúniorPas encore d'évaluation
- Roteiro de Exame NeurológicoDocument2 pagesRoteiro de Exame NeurológicoAlcemir JúniorPas encore d'évaluation
- Reconhecimento Das Situações de Emergência Avaliação PediátricaDocument10 pagesReconhecimento Das Situações de Emergência Avaliação PediátricaviinysantosPas encore d'évaluation
- Doença Ulcerosa Péptica e DuodenalDocument6 pagesDoença Ulcerosa Péptica e DuodenalAlcemir JúniorPas encore d'évaluation
- Ginecoobstetrcia Espce 2009Document8 pagesGinecoobstetrcia Espce 2009teleotravesPas encore d'évaluation
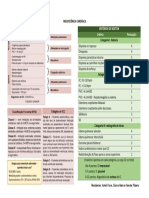
- Insuficiência CardíacaDocument1 pageInsuficiência CardíacaAlcemir JúniorPas encore d'évaluation
- Ginecoobstetrcia Espce 2009Document8 pagesGinecoobstetrcia Espce 2009teleotravesPas encore d'évaluation
- Síndrome de HipotireoidismoDocument4 pagesSíndrome de HipotireoidismoAlcemir JúniorPas encore d'évaluation
- Semiologia Do Aparelho RespiratorioDocument37 pagesSemiologia Do Aparelho RespiratorioAlcemir JúniorPas encore d'évaluation
- Manual Treinamento Vigilancia Sindromica WebDocument30 pagesManual Treinamento Vigilancia Sindromica WebAlcemir Júnior100% (1)
- 2877 Javascript BoaDocument39 pages2877 Javascript Boaphylip100% (1)
- LicenseDocument15 pagesLicensepprscamPas encore d'évaluation
- Fundação Nokia de EnsinoDocument4 pagesFundação Nokia de EnsinoAlcemir JúniorPas encore d'évaluation
- Apostila Completa de JavaScript (234 Páginas)Document234 pagesApostila Completa de JavaScript (234 Páginas)jeanbananaPas encore d'évaluation
- www.apostilaspdf.comDocument1 pagewww.apostilaspdf.comHv LaserPas encore d'évaluation