Vous aimerez peut-être aussi
- Words of Radiance: Book Two of The Stormlight Archive - Brandon SandersonDocument6 pagesWords of Radiance: Book Two of The Stormlight Archive - Brandon Sandersonxyrytepa0% (3)
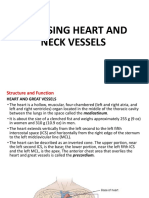
- Cardiovascular System: Mungcal, Dharlynette RTRPDocument77 pagesCardiovascular System: Mungcal, Dharlynette RTRPDharlyn MungcalPas encore d'évaluation
- Servo Motor Interfacing With 8051 Using Keil CompilerDocument11 pagesServo Motor Interfacing With 8051 Using Keil Compilertazeb100% (1)
- Civics and Ethics Edited Module, PDFDocument107 pagesCivics and Ethics Edited Module, PDFtazeb82% (11)
- CII Sohrabji Godrej GreenDocument30 pagesCII Sohrabji Godrej GreenRITHANYAA100% (2)
- HeartDocument36 pagesHeartSoovendran VaradarajanPas encore d'évaluation
- Cardiovascular SystemDocument12 pagesCardiovascular SystemDevendra RawatPas encore d'évaluation
- Cardiovascular System - Lecture IDocument4 pagesCardiovascular System - Lecture IpragantraPas encore d'évaluation
- 81: Mammalian Heart and Its RegulationDocument75 pages81: Mammalian Heart and Its RegulationIt's Ika100% (1)
- Chapter I - Cardiovascular System: HeartDocument2 pagesChapter I - Cardiovascular System: HeartIndranil SinhaPas encore d'évaluation
- Charter College: T.Miller - 7/2017Document28 pagesCharter College: T.Miller - 7/2017Waqar AhmedPas encore d'évaluation
- CardiovascularDocument30 pagesCardiovascularBeverly LavillaPas encore d'évaluation
- Functions of Cardiovascular System:: The Gross AnatomyDocument6 pagesFunctions of Cardiovascular System:: The Gross AnatomyShreyasi PatankarPas encore d'évaluation
- CardiovascularDocument30 pagesCardiovascularKristine Joy Librando EscalantePas encore d'évaluation
- Anatomy & Physiology of Heart: BY: Mr. Anurag Lecturer College of Nursing DMC & H, LudhianaDocument56 pagesAnatomy & Physiology of Heart: BY: Mr. Anurag Lecturer College of Nursing DMC & H, Ludhianapreet kaurPas encore d'évaluation
- Cardiovascular SystemDocument34 pagesCardiovascular Systemurooj100% (1)
- Cardiovascular System: Presented by DR Aparna Ramachandran Mds 1 Dept of Public Health DentistryDocument73 pagesCardiovascular System: Presented by DR Aparna Ramachandran Mds 1 Dept of Public Health DentistryAparna RamachandranPas encore d'évaluation
- HeartDocument6 pagesHeartAhmed OmaarPas encore d'évaluation
- Cardiovascular System - Transportation 1Document28 pagesCardiovascular System - Transportation 1Louise Mica Lee100% (1)
- Cardiogenic ShockDocument14 pagesCardiogenic ShockZellanien hdPas encore d'évaluation
- The Cardiac System LOBDocument3 pagesThe Cardiac System LOBbdhhuhddPas encore d'évaluation
- Module Cardiovascular System Anatomy and PhysiologyDocument9 pagesModule Cardiovascular System Anatomy and PhysiologyPATRICIA KAYE RIOPas encore d'évaluation
- Cardiovascular SystemDocument32 pagesCardiovascular SystemAugustus Alejandro ZenitPas encore d'évaluation
- Oral RevDocument6 pagesOral RevjjolaguerPas encore d'évaluation
- Chapter 20 Heart and Neck VesselsDocument10 pagesChapter 20 Heart and Neck Vesselsannoja selvaPas encore d'évaluation
- Anatomy of The HeartDocument8 pagesAnatomy of The HeartAbigail BrillantesPas encore d'évaluation
- Cardiovascular Physiology - Dra. ValerioDocument16 pagesCardiovascular Physiology - Dra. ValerioAlexandra Duque-David100% (2)
- Management of Clients With Problems of The Cardiovascular SystemDocument7 pagesManagement of Clients With Problems of The Cardiovascular Systemjerry smatt dumtoPas encore d'évaluation
- Heart: StructureDocument11 pagesHeart: StructureKert trocioPas encore d'évaluation
- Components of The Cardiovascular SystemDocument23 pagesComponents of The Cardiovascular SystemMr. DummyPas encore d'évaluation
- Internal Structure of HeartDocument1 pageInternal Structure of Heartmbudhathoki3000Pas encore d'évaluation
- Animal Physiolgy. Lec4Document22 pagesAnimal Physiolgy. Lec4ao868598Pas encore d'évaluation
- Cardiovascular System: K. Hariharan Iv Eee - 'B'Document33 pagesCardiovascular System: K. Hariharan Iv Eee - 'B'Hari Haran100% (1)
- Cardiac PhysiologyDocument102 pagesCardiac PhysiologyPeter Larsen100% (1)
- Lecture 5 (Heart)Document10 pagesLecture 5 (Heart)Άγγελος ΧαβέλαςPas encore d'évaluation
- Cardiovascular System BSN 1Document16 pagesCardiovascular System BSN 1Arianne Jen GenotivaPas encore d'évaluation
- Assignment On Anatomy and Physiology of Heart: Submitted By: Submitted To: Jayita Gayen Madam S. PoddarDocument10 pagesAssignment On Anatomy and Physiology of Heart: Submitted By: Submitted To: Jayita Gayen Madam S. PoddarJayita Gayen DuttaPas encore d'évaluation
- The HeartDocument65 pagesThe HeartMichael SamaniegoPas encore d'évaluation
- Anatomy of The HeartDocument28 pagesAnatomy of The HeartHerman DjawaPas encore d'évaluation
- Chapter 13 - HeartDocument5 pagesChapter 13 - Heartbussniesm05Pas encore d'évaluation
- Concept On Oxygenation: Gas TransportDocument135 pagesConcept On Oxygenation: Gas TransportNikko MelencionPas encore d'évaluation
- HeartDocument7 pagesHeartKaryll AguilaPas encore d'évaluation
- CVS McqsDocument5 pagesCVS McqsNishanthy PirabakarPas encore d'évaluation
- HUMAN ANATOMY AND PHYSIOLOGY LABORATORY Cardiovascular SystemDocument12 pagesHUMAN ANATOMY AND PHYSIOLOGY LABORATORY Cardiovascular SystemZaira MangalimanPas encore d'évaluation
- H.A. Assessing Heart and Neck VesselsDocument55 pagesH.A. Assessing Heart and Neck VesselsMc Ramil B. PraderoPas encore d'évaluation
- Circulatory SystemDocument25 pagesCirculatory SystemadnanPas encore d'évaluation
- Cardiac Diseases and Cardiac RehabilitationDocument49 pagesCardiac Diseases and Cardiac RehabilitationHenri Benedict VillafloresPas encore d'évaluation
- Anatomy and Physiolog1Document5 pagesAnatomy and Physiolog1Isabel Barredo Del MundoPas encore d'évaluation
- Anatomy and Histology of The Cardiovascular SystemDocument16 pagesAnatomy and Histology of The Cardiovascular SystemTasmiah HossainPas encore d'évaluation
- Cardiovascular System Kelmpk 1Document15 pagesCardiovascular System Kelmpk 1Arif WahyuPas encore d'évaluation
- Anatomy and Physiology ASCVDDocument9 pagesAnatomy and Physiology ASCVDAlvheen JoaquinPas encore d'évaluation
- Cardio & LymphaticDocument13 pagesCardio & LymphaticJoan GalarcePas encore d'évaluation
- The HeartDocument11 pagesThe HeartElisa TapalesPas encore d'évaluation
- Anatomy Lecture Notes Unit 7 Circulatory System - The HeartDocument7 pagesAnatomy Lecture Notes Unit 7 Circulatory System - The Heartrapunzel777Pas encore d'évaluation
- Chapter 20-Cardiovascular System The HeartDocument44 pagesChapter 20-Cardiovascular System The HeartleoPas encore d'évaluation
- Cardiovascular and Syrculation System, 2013Document92 pagesCardiovascular and Syrculation System, 2013Santi Purnama SariPas encore d'évaluation
- Anatomy of The HeartDocument5 pagesAnatomy of The HeartxXjhmXxPas encore d'évaluation
- 3 Circulation in ManDocument7 pages3 Circulation in ManAnasatcia Mcpherson 9c FPas encore d'évaluation
- Heart PathophysiologyDocument20 pagesHeart PathophysiologyDoctorDrapion100% (2)
- Cardiovascular System - The HeartDocument77 pagesCardiovascular System - The HeartZiraili VidalPas encore d'évaluation
- CardiovascularsystemDocument8 pagesCardiovascularsystemAkshaya SrinivasanPas encore d'évaluation
- MS Wrep IIDocument51 pagesMS Wrep IIiana-almocera-6970Pas encore d'évaluation
- Riya Arya - 21msc1279 - Biology For ChemistsDocument13 pagesRiya Arya - 21msc1279 - Biology For ChemistsSwadesh SenPas encore d'évaluation
- DocumentationDocument86 pagesDocumentationtazebPas encore d'évaluation
- Conventional Chapter 5Document58 pagesConventional Chapter 5tazebPas encore d'évaluation
- For Construction Technology and Management: Instructor: Amsalu ADocument200 pagesFor Construction Technology and Management: Instructor: Amsalu AtazebPas encore d'évaluation
- PWM Based DC Motor Speed Control Using MicrocontrollerDocument8 pagesPWM Based DC Motor Speed Control Using MicrocontrollertazebPas encore d'évaluation
- Boston University African Studies Center The International Journal of African Historical StudiesDocument4 pagesBoston University African Studies Center The International Journal of African Historical StudiestazebPas encore d'évaluation
- 1 s2.0 S0142941801000897 Main PDFDocument5 pages1 s2.0 S0142941801000897 Main PDFtazebPas encore d'évaluation
- Unit - 5: Microwave Passive Devices - Lecture 4 Wave Guide Tee JunctionsDocument5 pagesUnit - 5: Microwave Passive Devices - Lecture 4 Wave Guide Tee JunctionstazebPas encore d'évaluation
- Servo Motor Speed and Direction ControlDocument7 pagesServo Motor Speed and Direction Controltazeb100% (1)
- Chapter 2-1 PDFDocument70 pagesChapter 2-1 PDFtazeb100% (2)
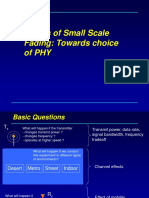
- Basics of Small Scale Fading: Towards Choice of PHYDocument18 pagesBasics of Small Scale Fading: Towards Choice of PHYtazebPas encore d'évaluation
- CH 03Document39 pagesCH 03tazebPas encore d'évaluation
- Mechanical Property 2Document33 pagesMechanical Property 2tazebPas encore d'évaluation
- CH 01Document60 pagesCH 01tazebPas encore d'évaluation
- Basics of Telecom Networks: Chapter-2Document17 pagesBasics of Telecom Networks: Chapter-2tazebPas encore d'évaluation
- Atomic Theory CH-1Document64 pagesAtomic Theory CH-1tazebPas encore d'évaluation
- Mekelle University: Eit-MDocument40 pagesMekelle University: Eit-MtazebPas encore d'évaluation
- Yared PDFDocument1 pageYared PDFtazebPas encore d'évaluation
- TazebDocument1 pageTazebtazebPas encore d'évaluation
- Worksheet On Chapter One and TwoDocument6 pagesWorksheet On Chapter One and TwotazebPas encore d'évaluation
- Cardio Vascular SystemDocument56 pagesCardio Vascular SystemtazebPas encore d'évaluation
- B.cement IndustriesDocument6 pagesB.cement IndustriestazebPas encore d'évaluation
- ADocument54 pagesActyvtePas encore d'évaluation
- Pediatrics: The Journal ofDocument11 pagesPediatrics: The Journal ofRohini TondaPas encore d'évaluation
- The New Order of BarbariansDocument39 pagesThe New Order of Barbariansbadguy100% (1)
- Mfin 7002 Investment Analysis and Portfolio ManagementDocument5 pagesMfin 7002 Investment Analysis and Portfolio ManagementjessiePas encore d'évaluation
- VRPIN 01843 PsychiatricReportDrivers 1112 WEBDocument2 pagesVRPIN 01843 PsychiatricReportDrivers 1112 WEBeverlord123Pas encore d'évaluation
- Victor 2Document30 pagesVictor 2EmmanuelPas encore d'évaluation
- Research FinalDocument55 pagesResearch Finalkieferdem071908Pas encore d'évaluation
- Healthy Apps Us New VarDocument9 pagesHealthy Apps Us New VarJESUS DELGADOPas encore d'évaluation
- AIIMS 2015 Solved PaperDocument436 pagesAIIMS 2015 Solved PaperSurya TejaPas encore d'évaluation
- DCS800ServiceManual RevADocument96 pagesDCS800ServiceManual RevAElinplastPas encore d'évaluation
- Generation III Sonic Feeder Control System Manual 20576Document32 pagesGeneration III Sonic Feeder Control System Manual 20576julianmataPas encore d'évaluation
- Pioneer 1019ah-K Repair ManualDocument162 pagesPioneer 1019ah-K Repair ManualjekPas encore d'évaluation
- Chapter 1 - Main Hydrological ConceptsDocument16 pagesChapter 1 - Main Hydrological ConceptsWhy Merah0% (1)
- Sale Counter List JuneDocument9 pagesSale Counter List Junep6a4nduPas encore d'évaluation
- KLA28 ProductsapplicationpresetDocument2 pagesKLA28 ProductsapplicationpresetcarxmozPas encore d'évaluation
- Best Mutual Funds For 2023 & BeyondDocument17 pagesBest Mutual Funds For 2023 & BeyondPrateekPas encore d'évaluation
- Safety Bulletin 09 - Emergency Escape Breathing Device - Product RecallDocument2 pagesSafety Bulletin 09 - Emergency Escape Breathing Device - Product RecallMuhammadPas encore d'évaluation
- I. Learning Objectives / Learning Outcomes: Esson LANDocument3 pagesI. Learning Objectives / Learning Outcomes: Esson LANWilliams M. Gamarra ArateaPas encore d'évaluation
- China Training WCDMA 06-06Document128 pagesChina Training WCDMA 06-06ryanz2009Pas encore d'évaluation
- KDE11SSDocument2 pagesKDE11SSluisgomezpasion1Pas encore d'évaluation
- ABARI-Volunteer Guide BookDocument10 pagesABARI-Volunteer Guide BookEla Mercado0% (1)
- Highlights ASME Guides Preheat PWHT IDocument4 pagesHighlights ASME Guides Preheat PWHT IArul Edwin Vijay VincentPas encore d'évaluation
- SEILDocument4 pagesSEILGopal RamalingamPas encore d'évaluation
- Magic Bullet Theory - PPTDocument5 pagesMagic Bullet Theory - PPTThe Bengal ChariotPas encore d'évaluation
- Introduction CompilerDocument47 pagesIntroduction CompilerHarshit SinghPas encore d'évaluation
- DirectionDocument1 pageDirectionJessica BacaniPas encore d'évaluation
- PD3 - Strategic Supply Chain Management: Exam Exemplar QuestionsDocument20 pagesPD3 - Strategic Supply Chain Management: Exam Exemplar QuestionsHazel Jael HernandezPas encore d'évaluation
- Kissoft 15,69,0.4Document10 pagesKissoft 15,69,0.4Daggupati PraveenPas encore d'évaluation