Vous aimerez peut-être aussi
- Controversies and Challenges of Vaccination: An Interview With Elizabeth MillerDocument7 pagesControversies and Challenges of Vaccination: An Interview With Elizabeth MillerShasha IkaPas encore d'évaluation
- Vaccines: Making the Right Choice for Your ChildD'EverandVaccines: Making the Right Choice for Your ChildÉvaluation : 5 sur 5 étoiles5/5 (2)
- Vaccines: Does herd immunity justify permanent impairment for a few?D'EverandVaccines: Does herd immunity justify permanent impairment for a few?Pas encore d'évaluation
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionD'EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionPas encore d'évaluation
- Are Vaccines SafeDocument3 pagesAre Vaccines SafeJun Kai Ong100% (1)
- Vaccine Research SAADDocument5 pagesVaccine Research SAADAHS100% (7)
- Could Parents Be Held Liable For Not Immunizing Their Children?Document26 pagesCould Parents Be Held Liable For Not Immunizing Their Children?Nathan RaabPas encore d'évaluation
- Restoring Confidence in Vaccines in The COVID-19 Era: Expert Review of VaccinesDocument4 pagesRestoring Confidence in Vaccines in The COVID-19 Era: Expert Review of VaccinesRaquel CostaPas encore d'évaluation
- Should I Vaccinate My Child Kindred Article AustraliaDocument9 pagesShould I Vaccinate My Child Kindred Article AustraliaKCSPas encore d'évaluation
- Vaccines: A Second Opinion by Gary Null, PHD (Oct. 18, 2009)Document45 pagesVaccines: A Second Opinion by Gary Null, PHD (Oct. 18, 2009)humanati100% (4)
- Research PaperDocument13 pagesResearch Paperapi-546731047Pas encore d'évaluation
- Thesis Statement On Autism and VaccinesDocument7 pagesThesis Statement On Autism and VaccinesPaperHelperUK100% (2)
- VaccinationsDocument13 pagesVaccinationsapi-548389172Pas encore d'évaluation
- V VV Vvaccine Accine Accine Accine Accine Safety Safety Safety Safety SafetyDocument12 pagesV VV Vvaccine Accine Accine Accine Accine Safety Safety Safety Safety SafetyJandre ShancezPas encore d'évaluation
- Summary of Vax-Unvax by Robert F. Kennedy Jr.: Let the Science Speak (Children’s Health Defense)D'EverandSummary of Vax-Unvax by Robert F. Kennedy Jr.: Let the Science Speak (Children’s Health Defense)Pas encore d'évaluation
- Swine Flu White PaperDocument94 pagesSwine Flu White Paperlocopr1100% (1)
- Research Paper Vaccines EssayDocument8 pagesResearch Paper Vaccines Essayapi-235445707100% (4)
- A Position Paper About Vaccines To Fight Infectious DiseasesDocument6 pagesA Position Paper About Vaccines To Fight Infectious DiseasesJonas Belen PerezPas encore d'évaluation
- Research Paper On Childhood VaccinesDocument7 pagesResearch Paper On Childhood Vaccinesafnkjdhxlewftq100% (1)
- Literature Review MMR VaccineDocument7 pagesLiterature Review MMR Vaccineafmzmxkayjyoso100% (1)
- Paper 3 Argumentative Essay Alexis-2Document9 pagesPaper 3 Argumentative Essay Alexis-2api-314832012Pas encore d'évaluation
- Research Paper On Childhood VaccinationsDocument8 pagesResearch Paper On Childhood Vaccinationsefjr9yx3100% (1)
- Research Paper On Child VaccinationsDocument7 pagesResearch Paper On Child Vaccinationspwvgqccnd100% (1)
- 7 Reasons Not To VaccinateDocument4 pages7 Reasons Not To VaccinateMiri Ch67% (3)
- Research Paper Outline VaccinesDocument9 pagesResearch Paper Outline Vaccinessvgkjqbnd100% (1)
- The Awareness Level On The Benefit1Document12 pagesThe Awareness Level On The Benefit1Joshua ValledorPas encore d'évaluation
- AddddDocument14 pagesAddddapi-547718836Pas encore d'évaluation
- Influenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?D'EverandInfluenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?Pas encore d'évaluation
- Value Paper Assignment Comm 1270Document8 pagesValue Paper Assignment Comm 1270api-346605656Pas encore d'évaluation
- Public Trust and Vaccine Acceptance-International PerspectivesDocument6 pagesPublic Trust and Vaccine Acceptance-International PerspectivesSara MarzoukPas encore d'évaluation
- San Diego Measles Outbreak of 2008Document8 pagesSan Diego Measles Outbreak of 2008karisa wulandariPas encore d'évaluation
- Vaccine HesitancyDocument12 pagesVaccine HesitancyMhd HidayattullahPas encore d'évaluation
- phsc002 Video ScriptDocument4 pagesphsc002 Video Scriptapi-301372772Pas encore d'évaluation
- Local Studies and LiteratureDocument9 pagesLocal Studies and LiteratureKarl GutierrezPas encore d'évaluation
- Nursing Research PaperDocument15 pagesNursing Research Paperapi-502994344Pas encore d'évaluation
- The Awareness Level On The Benefit1Document10 pagesThe Awareness Level On The Benefit1Joshua ValledorPas encore d'évaluation
- Vaccine CoercionDocument8 pagesVaccine Coercionmarkclaus89Pas encore d'évaluation
- The Plausible Link Between Vaccines and Autism Has Not Been DebunkedDocument7 pagesThe Plausible Link Between Vaccines and Autism Has Not Been DebunkedSofia marisa fernandesPas encore d'évaluation
- Final PaperDocument44 pagesFinal PaperForshia Antonette BañaciaPas encore d'évaluation
- DCM05 Vaccination MythsDocument11 pagesDCM05 Vaccination MythsNOE100% (1)
- Literature Review On Childhood ImmunizationDocument4 pagesLiterature Review On Childhood Immunizationc5e4jfpn100% (1)
- RRL 01 07 22Document9 pagesRRL 01 07 22Ponce GuerreroPas encore d'évaluation
- Eng 1201 Research EssayDocument13 pagesEng 1201 Research Essayapi-583927558Pas encore d'évaluation
- Mandatory VaccinationsDocument7 pagesMandatory Vaccinationsapi-487208181Pas encore d'évaluation
- Literature Review On Knowledge of ImmunizationDocument7 pagesLiterature Review On Knowledge of Immunizationtwdhopwgf100% (1)
- Vaccine Hesitancy Outbreaks' Using Epidemiological Modeling of The Spread of Ideas To Understand The Effects of Vaccine Related Events On Vaccine HesitancyDocument25 pagesVaccine Hesitancy Outbreaks' Using Epidemiological Modeling of The Spread of Ideas To Understand The Effects of Vaccine Related Events On Vaccine HesitancyHosam GomaaPas encore d'évaluation
- Final Program ProposalDocument8 pagesFinal Program Proposalotienocliff7Pas encore d'évaluation
- Theoretical FrameworkDocument2 pagesTheoretical FrameworkljgerzonPas encore d'évaluation
- MCRPDocument6 pagesMCRPapi-302997678Pas encore d'évaluation
- Debunking The Stigma Around VaccinationsDocument10 pagesDebunking The Stigma Around Vaccinationsapi-534368432Pas encore d'évaluation
- HMP Research ProjectDocument8 pagesHMP Research Projectapi-738698091Pas encore d'évaluation
- Vaccines EssayDocument12 pagesVaccines Essayapi-233200175Pas encore d'évaluation
- KAP ImmunizationDocument6 pagesKAP ImmunizationSherwin Buluran100% (1)
- Immunisation Journal ReferencesDocument44 pagesImmunisation Journal ReferencesFiona Arnott100% (1)
- Research Paper ImmunizationDocument9 pagesResearch Paper Immunizationk0wyn0tykob3100% (1)
- Fisip 2019 Essay 2Document2 pagesFisip 2019 Essay 2Aldrista AulitamariPas encore d'évaluation
- Literature Review VaccinesDocument7 pagesLiterature Review Vaccinesigmitqwgf100% (1)
- Definisi InfrastrukturDocument7 pagesDefinisi InfrastrukturClarita BangunPas encore d'évaluation
- Desain Perhitungan IpalDocument2 pagesDesain Perhitungan IpalClarita BangunPas encore d'évaluation
- Vibrio Vulnificus: SymptomsDocument3 pagesVibrio Vulnificus: SymptomsClarita BangunPas encore d'évaluation
- Laporan Aktualisasi: by Raymond Mangapultua Janius JansenDocument12 pagesLaporan Aktualisasi: by Raymond Mangapultua Janius JansenClarita BangunPas encore d'évaluation
- Proposal and Marketing Plan: Subtitle Text HereDocument2 pagesProposal and Marketing Plan: Subtitle Text HereClarita BangunPas encore d'évaluation
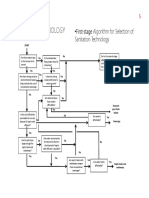
- FlowChart SeleksiTeknologiSANITASI PDFDocument3 pagesFlowChart SeleksiTeknologiSANITASI PDFClarita BangunPas encore d'évaluation
- The Germ Theory of DiseaseDocument5 pagesThe Germ Theory of DiseaseClarita BangunPas encore d'évaluation
- English ConjunctionDocument8 pagesEnglish ConjunctionClarita BangunPas encore d'évaluation
- What's Protectionism?: OutlineDocument4 pagesWhat's Protectionism?: OutlineClarita BangunPas encore d'évaluation
- Grafik X (Jarak) Terhadap Y (Kedalaman)Document18 pagesGrafik X (Jarak) Terhadap Y (Kedalaman)Clarita BangunPas encore d'évaluation
- Academic WritingDocument88 pagesAcademic WritingClarita BangunPas encore d'évaluation
- John Snow (1813-1858) and CholeraDocument3 pagesJohn Snow (1813-1858) and CholeraClarita BangunPas encore d'évaluation
- 08 Gaya GayaDocument22 pages08 Gaya GayaClarita BangunPas encore d'évaluation
- NAME: Clarita MONTH: November: SundayDocument2 pagesNAME: Clarita MONTH: November: SundayClarita BangunPas encore d'évaluation
- v2 - Headloss Gate ValveDocument8 pagesv2 - Headloss Gate ValveClarita BangunPas encore d'évaluation
- Arca Majora 2 LicenseDocument1 pageArca Majora 2 LicenseClarita BangunPas encore d'évaluation
- Presentation SkillDocument107 pagesPresentation SkillClarita BangunPas encore d'évaluation
- A Study On Assessment of Effect of Samyoga Viruddha Ahara Consumption On Metabolic Syndrome in 35 - 50 Year Old Men and Women of MumbaiDocument11 pagesA Study On Assessment of Effect of Samyoga Viruddha Ahara Consumption On Metabolic Syndrome in 35 - 50 Year Old Men and Women of MumbaiIJAR JOURNALPas encore d'évaluation
- Disease DetectivesDocument2 pagesDisease DetectivesbkberkowitzPas encore d'évaluation
- (Asking-Reporting Health Problem and Diagnosing)Document10 pages(Asking-Reporting Health Problem and Diagnosing)nilanPas encore d'évaluation
- Systemic Inflammatory Response Syndrome (SIRS) PrognosisDocument16 pagesSystemic Inflammatory Response Syndrome (SIRS) PrognosisIPGDx100% (1)
- WHO 2011 Typhoid Fever PDFDocument39 pagesWHO 2011 Typhoid Fever PDFNatasha ChandraPas encore d'évaluation
- Kerangka Kerja Sistem Kesehatan (Who)Document15 pagesKerangka Kerja Sistem Kesehatan (Who)LipatriPas encore d'évaluation
- Thesis PDFDocument50 pagesThesis PDFapi-349572960100% (1)
- Emmanuel Rivers SlidesDocument91 pagesEmmanuel Rivers SlidescarlodapPas encore d'évaluation
- Patient's ProfileDocument1 pagePatient's ProfilehsiriaPas encore d'évaluation
- Vitamin C in Health and Disease PDFDocument300 pagesVitamin C in Health and Disease PDFNany Caroline100% (1)
- Health System PresentationDocument15 pagesHealth System PresentationChristine Rodriguez-Guerrero100% (1)
- Midterm Evaluation - ClinicalDocument7 pagesMidterm Evaluation - Clinicalapi-240864098Pas encore d'évaluation
- 5 Reptile Medicine and Surgery - Mader - 2nd EditionDocument1 258 pages5 Reptile Medicine and Surgery - Mader - 2nd EditionJoão Gabriel M. Alkmim100% (1)
- Add Risk Min MeasDocument12 pagesAdd Risk Min MeasVladimir KostovskiPas encore d'évaluation
- GE Healthcare Versana Essential DatasheetDocument5 pagesGE Healthcare Versana Essential Datasheetbashir019Pas encore d'évaluation
- Hematology Course SyllabusDocument2 pagesHematology Course Syllabusmohamedali991706Pas encore d'évaluation
- Fields of NursingDocument8 pagesFields of NursingOmie TumanguilPas encore d'évaluation
- Communication Flow Chart For Symptomatic Personnel: TTMF-Temporary Treatment and Monitoring FacilityDocument7 pagesCommunication Flow Chart For Symptomatic Personnel: TTMF-Temporary Treatment and Monitoring FacilityBrynard GarbosaPas encore d'évaluation
- County Assembly of MombasaDocument11 pagesCounty Assembly of MombasaDavis MitchelPas encore d'évaluation
- Revisi STANDAR PELAYANAN LABORATORIUM EditDocument47 pagesRevisi STANDAR PELAYANAN LABORATORIUM EditMuhamad SetoPas encore d'évaluation
- Mental Health ACT Terms and AbbreviationsDocument2 pagesMental Health ACT Terms and AbbreviationsAsha ColmanPas encore d'évaluation
- Development PlanDocument2 pagesDevelopment Planapi-531834240Pas encore d'évaluation
- Overview of Treatment Approaches For Hepatocellular Carcinoma - UpToDateDocument66 pagesOverview of Treatment Approaches For Hepatocellular Carcinoma - UpToDateJoyce SumagaysayPas encore d'évaluation
- Cataract PTDocument9 pagesCataract PTPreeti SharmaPas encore d'évaluation
- Journalistic WritingDocument2 pagesJournalistic Writingeugenia certezaPas encore d'évaluation
- Advert Gender and Defence 25.04.2023Document18 pagesAdvert Gender and Defence 25.04.2023kingPas encore d'évaluation
- FortisDocument47 pagesFortisKshitiz KadamPas encore d'évaluation
- KidAssure GIO Rider BrochureDocument4 pagesKidAssure GIO Rider BrochureCC KosPas encore d'évaluation
- Un Sustainable Development GoalsDocument3 pagesUn Sustainable Development GoalsChampyPas encore d'évaluation
- Practice - English Lesson - Fira Yuniar - 200704009Document5 pagesPractice - English Lesson - Fira Yuniar - 200704009Fira YuniarPas encore d'évaluation