Vous aimerez peut-être aussi
- Principles and Practice of Clinical Trial MedicineD'EverandPrinciples and Practice of Clinical Trial MedicineÉvaluation : 4 sur 5 étoiles4/5 (1)
- Clinical Research OverviewDocument40 pagesClinical Research Overviewjyoti100% (1)
- The Sourcebook for Clinical Research: A Practical Guide for Study ConductD'EverandThe Sourcebook for Clinical Research: A Practical Guide for Study ConductÉvaluation : 5 sur 5 étoiles5/5 (1)
- Ethical Considerations When Preparing a Clinical Research ProtocolD'EverandEthical Considerations When Preparing a Clinical Research ProtocolPas encore d'évaluation
- Pharmacoepidemiology and Pharmacovigilance: Synergistic Tools to Better Investigate Drug SafetyD'EverandPharmacoepidemiology and Pharmacovigilance: Synergistic Tools to Better Investigate Drug SafetyÉvaluation : 4.5 sur 5 étoiles4.5/5 (3)
- A Comprehensive and Practical Guide to Clinical TrialsD'EverandA Comprehensive and Practical Guide to Clinical TrialsÉvaluation : 3 sur 5 étoiles3/5 (1)
- Clinical Data Management A Complete Guide - 2020 EditionD'EverandClinical Data Management A Complete Guide - 2020 EditionPas encore d'évaluation
- Essential Documents Required For Clinical TrialDocument5 pagesEssential Documents Required For Clinical Trialnicky02100% (6)
- SAS Clinical TrialsDocument25 pagesSAS Clinical Trialsnishu1212100% (5)
- Clinical Data Management and E-Clinical Trials (IPS)Document22 pagesClinical Data Management and E-Clinical Trials (IPS)api-3842711100% (5)
- The Monitoring ProcessDocument10 pagesThe Monitoring Processapi-3810976100% (2)
- Role and Responsibilities of CROs and SponsorsDocument33 pagesRole and Responsibilities of CROs and SponsorsShilpi Paliwal100% (2)
- Clinical Trial DocumentsDocument37 pagesClinical Trial Documentsapi-37446750% (1)
- Trial Master FileDocument2 pagesTrial Master Fileapi-3810976Pas encore d'évaluation
- Clinical Data Management Ensures Trial IntegrityDocument39 pagesClinical Data Management Ensures Trial IntegrityBhavana Alapati100% (4)
- Cra GuideDocument17 pagesCra Guidebitterlemon01Pas encore d'évaluation
- Clinical Trial MonitoringDocument14 pagesClinical Trial Monitoringsreeraj.guruvayoor100% (1)
- Annotated CRFDocument7 pagesAnnotated CRFSurbhi Gogar PandeyPas encore d'évaluation
- Designs of Clinical TrialDocument7 pagesDesigns of Clinical TrialSruthi100% (1)
- Global Clinical Trials Playbook: Capacity and Capability BuildingD'EverandGlobal Clinical Trials Playbook: Capacity and Capability BuildingMenghis BairuPas encore d'évaluation
- Clinical Trials Audit Preparation: A Guide for Good Clinical Practice (GCP) InspectionsD'EverandClinical Trials Audit Preparation: A Guide for Good Clinical Practice (GCP) InspectionsPas encore d'évaluation
- Interview Questions For PharmacovigilanceDocument11 pagesInterview Questions For PharmacovigilanceRumaisa Wasi100% (2)
- Clinical Data Management (Presentation by Sarma)Document30 pagesClinical Data Management (Presentation by Sarma)T V S Sarma100% (40)
- Developing and Writing CRFDocument23 pagesDeveloping and Writing CRFsuri333Pas encore d'évaluation
- Clinical Data Management Best Practices and ComponentsDocument5 pagesClinical Data Management Best Practices and Componentsmail4syedPas encore d'évaluation
- Clinical Trial Safety Data Management (Presentation by TVS Sarma)Document27 pagesClinical Trial Safety Data Management (Presentation by TVS Sarma)T V S Sarma100% (11)
- Kolman, Meng, Scott - Good Clinical Practice - SOP For Clinical Researchers (1998) PDFDocument188 pagesKolman, Meng, Scott - Good Clinical Practice - SOP For Clinical Researchers (1998) PDFjantoniohergut100% (1)
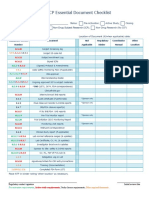
- ICH GCP Essential Document ChecklistDocument2 pagesICH GCP Essential Document ChecklistMohammed Yousffi50% (2)
- Clinical Trial ChecklistDocument3 pagesClinical Trial ChecklistIzzi FekratPas encore d'évaluation
- WWORTH SOP10ProjectManagementV2.2 140507Document21 pagesWWORTH SOP10ProjectManagementV2.2 140507Fery Alapola100% (1)
- Documentation of Clinical Trial Monitoring: A practical guide compliant with Good Clinical PracticeD'EverandDocumentation of Clinical Trial Monitoring: A practical guide compliant with Good Clinical PracticeÉvaluation : 5 sur 5 étoiles5/5 (1)
- Basic Clinical Trial Terms Explained With PicturesDocument1 pageBasic Clinical Trial Terms Explained With PicturesJanelle Bowden100% (5)
- Risk-Based Monitoring and Fraud Detection in Clinical Trials Using JMP and SASD'EverandRisk-Based Monitoring and Fraud Detection in Clinical Trials Using JMP and SASPas encore d'évaluation
- New Cro Audit FormDocument4 pagesNew Cro Audit FormSiragamSaikumar100% (1)
- Clinical trials budgeting methodsDocument52 pagesClinical trials budgeting methodsjlbabson100% (5)
- Stakeholders in Clinical ResearchDocument37 pagesStakeholders in Clinical Researchsuri33367% (3)
- Drug Regulatory Affairs Syllabus KUDocument11 pagesDrug Regulatory Affairs Syllabus KUsathyasrireddyPas encore d'évaluation
- Audit Manual Clinical TrialDocument22 pagesAudit Manual Clinical TrialnikjadhavPas encore d'évaluation
- SAS Interview Questions - ClinicalDocument9 pagesSAS Interview Questions - ClinicalDiku ShahPas encore d'évaluation
- The Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewD'EverandThe Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewPas encore d'évaluation
- Introduction of Clinical Data ManagementDocument21 pagesIntroduction of Clinical Data Managementapi-3842711100% (5)
- Audit and Inspection in Clinical TrialDocument57 pagesAudit and Inspection in Clinical TrialRanjeet Prasad100% (2)
- Clinical Trials Flow ProcessDocument77 pagesClinical Trials Flow ProcessAnonymous Qr9nZRb100% (2)
- Guide To Clinical Trial Protocol Content and FormatDocument8 pagesGuide To Clinical Trial Protocol Content and FormatRohit Manakchand ZawarPas encore d'évaluation
- Overview of E-CTD and Modules - v02Document39 pagesOverview of E-CTD and Modules - v02Swapnil YeolePas encore d'évaluation
- Tool Summary Sheet: Blue ItalicsDocument32 pagesTool Summary Sheet: Blue ItalicsAli FakihPas encore d'évaluation
- Sas Interview QuestionsDocument9 pagesSas Interview QuestionsPamukuntla Shyam ReddyPas encore d'évaluation
- Clinical Research AssociateDocument2 pagesClinical Research AssociatepalkybdPas encore d'évaluation
- Clinical Trials PDFDocument17 pagesClinical Trials PDFBin Hip100% (2)
- CLN-20 00 Investigational Product HandlingDocument4 pagesCLN-20 00 Investigational Product Handlingpopatlilo2Pas encore d'évaluation
- Quality Control and Assurance in Clinical ResearchDocument5 pagesQuality Control and Assurance in Clinical Researchvmreddi100% (4)
- Investigators Responsibilities With GCPDocument16 pagesInvestigators Responsibilities With GCPLlosa JunePas encore d'évaluation
- Clinical Research ManualDocument285 pagesClinical Research ManualAbhiram Banerjee100% (5)
- Essential Documents Checklist Clinical Trial InterventionalDocument3 pagesEssential Documents Checklist Clinical Trial InterventionalPunk Rombus LeePas encore d'évaluation
- Standard Operating Procedures For Clinical Research CoordinatorsDocument13 pagesStandard Operating Procedures For Clinical Research Coordinatorsmmohit_990% (1)
- The Study Protocol Part TwoDocument12 pagesThe Study Protocol Part TwoGerman LambogliaPas encore d'évaluation
- CDISCDocument18 pagesCDISCkiran3114100% (4)
- CDM Processes C1Document41 pagesCDM Processes C1api-3810976Pas encore d'évaluation
- Kids v. Cancer v. Kinds vs. Cancer - Trademark Complaint PDFDocument16 pagesKids v. Cancer v. Kinds vs. Cancer - Trademark Complaint PDFMark JaffePas encore d'évaluation
- State-by-State Provisions For Adding Qualifying ConditionsDocument5 pagesState-by-State Provisions For Adding Qualifying ConditionsMPPPas encore d'évaluation
- Enhancing The Diversity of Clinical Trial PopulationsDocument18 pagesEnhancing The Diversity of Clinical Trial PopulationsMelissa FassbenderPas encore d'évaluation
- CCD Producer Application Checklist 12.7.21 1Document4 pagesCCD Producer Application Checklist 12.7.21 1Gabriel BaezaPas encore d'évaluation
- Constitutional Law 2 Midterm Exam A.Y. 2021 2022Document8 pagesConstitutional Law 2 Midterm Exam A.Y. 2021 2022Jaime Luna100% (2)
- Module 5 PEDocument28 pagesModule 5 PEGauri GhulePas encore d'évaluation
- Medical Marijuana: Here Are The Things That You Should KnowDocument6 pagesMedical Marijuana: Here Are The Things That You Should KnowDiyonata KortezPas encore d'évaluation
- How COVID Is Reshaping Global Policy and What It Means For Market AccessDocument21 pagesHow COVID Is Reshaping Global Policy and What It Means For Market AccessMarti Aroa FamilyPas encore d'évaluation
- Ich E2f DsurDocument23 pagesIch E2f Dsurvinay patidarPas encore d'évaluation
- Psilocybin Study Report Final 022322Document28 pagesPsilocybin Study Report Final 022322Helen BennettPas encore d'évaluation
- Interview Question Clinical TrialsDocument20 pagesInterview Question Clinical Trialshruday100% (3)
- PHL 299Document11 pagesPHL 299Mustafa GOKERPas encore d'évaluation
- FLCCC Alliance Frequently Asked Questions On IvermectinDocument13 pagesFLCCC Alliance Frequently Asked Questions On IvermectinAlan NPas encore d'évaluation
- Compassionate UseDocument10 pagesCompassionate UseSarahPas encore d'évaluation
- TxMJPolicy Voter Guide - 2020 Primary Edition - Republican CandidatesDocument175 pagesTxMJPolicy Voter Guide - 2020 Primary Edition - Republican CandidatesinvictusatxPas encore d'évaluation
- CRI Annual Report 2006Document10 pagesCRI Annual Report 2006aptureincPas encore d'évaluation
- GMPs Workshop - Analytical Method Validation (Regulatory Perspective - Linda NG, FDA)Document31 pagesGMPs Workshop - Analytical Method Validation (Regulatory Perspective - Linda NG, FDA)Helena DordioPas encore d'évaluation
- Duke Rodriguez Petition For Writ of Mandamus DOHDocument198 pagesDuke Rodriguez Petition For Writ of Mandamus DOHNew Mexico Political ReportPas encore d'évaluation
- Right To Try Act - UsaDocument4 pagesRight To Try Act - UsaJessica MessaPas encore d'évaluation
- Latin America 2020 - FINAL PDFDocument52 pagesLatin America 2020 - FINAL PDFJose David Pedraza BallesterosPas encore d'évaluation
- DEA Psilocybin LawsuitDocument69 pagesDEA Psilocybin LawsuitMarijuana MomentPas encore d'évaluation
- Compassion Vs Control: FDA Investigational-Drug Regulation, Cato Policy AnalysisDocument19 pagesCompassion Vs Control: FDA Investigational-Drug Regulation, Cato Policy AnalysisCato InstitutePas encore d'évaluation
- Introduction To Market Access For Pharmaceuticals by Mondher ToumiDocument204 pagesIntroduction To Market Access For Pharmaceuticals by Mondher ToumiDhrithi100% (1)
- SB 3: Medical Marijuana BillDocument26 pagesSB 3: Medical Marijuana BillSteven DoylePas encore d'évaluation
- What Is A Clinical Trial?: BackgroundDocument8 pagesWhat Is A Clinical Trial?: BackgroundsenthilmnursePas encore d'évaluation
- Behandlingstudier - Overblik Over Planlagte Og Igangværende Studier Af Lægemidler Til Behandling Af COVID-19Document217 pagesBehandlingstudier - Overblik Over Planlagte Og Igangværende Studier Af Lægemidler Til Behandling Af COVID-19Ishan ShahPas encore d'évaluation
- 1 Early Access Application 14 May 2018 PDFDocument2 pages1 Early Access Application 14 May 2018 PDFArdat LiliPas encore d'évaluation
- Clinical Trial Audit FDA Reg OutlinesDocument12 pagesClinical Trial Audit FDA Reg OutlinesKatePas encore d'évaluation
- FDA Drug Review and Approval Process BasicsDocument8 pagesFDA Drug Review and Approval Process BasicsTawfeeq BA AbbadPas encore d'évaluation
- Clinical Research NotesDocument98 pagesClinical Research NotesToha Afreen100% (1)