Vous aimerez peut-être aussi
- 2021-2022 Proposed Budget SummaryDocument2 pages2021-2022 Proposed Budget SummaryRiverheadLOCALPas encore d'évaluation
- Client Information SheetDocument2 pagesClient Information SheetElaine Joy O. ApostolPas encore d'évaluation
- Investor Presentation Dec 2018 GeneralitatDocument35 pagesInvestor Presentation Dec 2018 GeneralitatFernando HernandezPas encore d'évaluation
- Application Form: (Commercial/Office Spaces)Document1 pageApplication Form: (Commercial/Office Spaces)Chris John MaghanoyPas encore d'évaluation
- Riverhead Central School District 2021-2022 Budget Presentation No. 1Document38 pagesRiverhead Central School District 2021-2022 Budget Presentation No. 1RiverheadLOCALPas encore d'évaluation
- Medication Log Template-1Document1 pageMedication Log Template-1TItuSaAMI ShAHINPas encore d'évaluation
- Performance Measures Using Electronic Health Records Five Case StudiesDocument46 pagesPerformance Measures Using Electronic Health Records Five Case StudieswmhoggPas encore d'évaluation
- David Sm13e CN 12Document16 pagesDavid Sm13e CN 12Koki Mostafa100% (1)
- F-05 814 Pricing StrategyDocument24 pagesF-05 814 Pricing Strategydinosaur2512Pas encore d'évaluation
- Pharma SwotDocument4 pagesPharma SwotzeeshannaqviPas encore d'évaluation
- Health Prediction Using Data Mining - Scope DocumentDocument4 pagesHealth Prediction Using Data Mining - Scope DocumentHaris AhmedPas encore d'évaluation
- Director Sales Healthcare Pharmaceuticals in Columbus OH Resume Thomas KomendaDocument2 pagesDirector Sales Healthcare Pharmaceuticals in Columbus OH Resume Thomas KomendaThomasKomendaPas encore d'évaluation
- Prosthetic Knee SystemsDocument2 pagesProsthetic Knee SystemshppresarioPas encore d'évaluation
- The New Trends of Drug R&D Outsourcing in China and IndiaDocument20 pagesThe New Trends of Drug R&D Outsourcing in China and Indiajz9826Pas encore d'évaluation
- Price Analytics: Dr. Keerti Jain NIIT University, NeemranaDocument88 pagesPrice Analytics: Dr. Keerti Jain NIIT University, NeemranaTushar GoelPas encore d'évaluation
- Kotler Summary G-8Document3 pagesKotler Summary G-8Varun KumarPas encore d'évaluation
- Gen MatrixDocument36 pagesGen MatrixPrakash VadavadagiPas encore d'évaluation
- List of Low-Cost Spay & Neuter ClinicsDocument10 pagesList of Low-Cost Spay & Neuter Clinicsave marie maquintoPas encore d'évaluation
- Artificial Intelligence For Blood AnalysisDocument14 pagesArtificial Intelligence For Blood AnalysisKIPNGENO EMMANUELPas encore d'évaluation
- MN Res Home Energy Audit ReportDocument9 pagesMN Res Home Energy Audit ReportFarwa MalikPas encore d'évaluation
- RT MDocument6 pagesRT MShikhar NigamPas encore d'évaluation
- Medical Device Sales Representative in Buffalo NY Resume Stephen KleeDocument2 pagesMedical Device Sales Representative in Buffalo NY Resume Stephen KleeStephenKleePas encore d'évaluation
- Incident Report Template 01Document6 pagesIncident Report Template 01siva ramakrishnanPas encore d'évaluation
- Pharmaceutical Medical Sales Representative in Houston TX Resume Jennifer MillerDocument1 pagePharmaceutical Medical Sales Representative in Houston TX Resume Jennifer MillerJenniferMiller1Pas encore d'évaluation
- Sales-BioTech or Pharma or Medical Equipment SalesDocument3 pagesSales-BioTech or Pharma or Medical Equipment Salesapi-77973322Pas encore d'évaluation
- Evaluating The Marketing Performance (Audit Tools and Audit Process)Document2 pagesEvaluating The Marketing Performance (Audit Tools and Audit Process)affanPas encore d'évaluation
- Microprocessor-Controlled Prosthetic KneesDocument17 pagesMicroprocessor-Controlled Prosthetic KneesCTAFDocumentsPas encore d'évaluation
- GMP BioconDocument2 pagesGMP BioconDan StantonPas encore d'évaluation
- Diagnostic Imaging Global Market-Forecast To 2022Document4 pagesDiagnostic Imaging Global Market-Forecast To 2022VinayPas encore d'évaluation
- WP 1Document10 pagesWP 1Khyati B. ShahPas encore d'évaluation
- Product Demo TemplateDocument9 pagesProduct Demo Templateconnectadasgupta100% (1)
- Healthcast The Customisation of Diagnosis Care and Cure-Pwc-2010 PDFDocument58 pagesHealthcast The Customisation of Diagnosis Care and Cure-Pwc-2010 PDFEhli HibrePas encore d'évaluation
- Pulse OximeterDocument4 pagesPulse Oximeterjuliana valenciaPas encore d'évaluation
- Sales Account Manager Biotechnology in Boston MA Resume Cynthia SmithDocument2 pagesSales Account Manager Biotechnology in Boston MA Resume Cynthia SmithCynthiaSmith2Pas encore d'évaluation
- Components of Physical FitnessDocument8 pagesComponents of Physical Fitnessoli garkiPas encore d'évaluation
- Patient Satisfaction: Bhanu PrakashDocument8 pagesPatient Satisfaction: Bhanu PrakashAjlan AliPas encore d'évaluation
- Mobile App Survey ReportDocument18 pagesMobile App Survey ReportvictrrocksPas encore d'évaluation
- Glossary Health TeccnologyDocument4 pagesGlossary Health TeccnologyreneportilloPas encore d'évaluation
- Cecy JDDocument4 pagesCecy JDClash ClashhPas encore d'évaluation
- Sales Territory Concept Designing & Functions and Qualities of Sales ExecutivesDocument22 pagesSales Territory Concept Designing & Functions and Qualities of Sales ExecutivesStany D'melloPas encore d'évaluation
- Remote Patient Monitoring System With Focused Research On Vital Signs Through Sensors BS (CS) 13 BatchDocument10 pagesRemote Patient Monitoring System With Focused Research On Vital Signs Through Sensors BS (CS) 13 BatchBaSit ALi DharejoPas encore d'évaluation
- Base Slides - Pricing PDFDocument58 pagesBase Slides - Pricing PDFvitrahulPas encore d'évaluation
- Customer Lifetime Value: OriginsDocument4 pagesCustomer Lifetime Value: OriginsSumit RathiPas encore d'évaluation
- Health Monitoring Using Mobile Phones: Course:-Mobile Networking Instructor: - Dr. Helmy AhmedDocument40 pagesHealth Monitoring Using Mobile Phones: Course:-Mobile Networking Instructor: - Dr. Helmy AhmedsmritiPas encore d'évaluation
- Face Mask QuotationDocument2 pagesFace Mask QuotationSirPas encore d'évaluation
- The Growth of Non-State Hospitals in Vietnam (WP15)Document20 pagesThe Growth of Non-State Hospitals in Vietnam (WP15)Nossal Institute for Global HealthPas encore d'évaluation
- ForYourIrisOnly Brochure - Identity Management With Iris Recognition TechnologyDocument7 pagesForYourIrisOnly Brochure - Identity Management With Iris Recognition TechnologyIriTechIncPas encore d'évaluation
- Portfolio ExampleDocument34 pagesPortfolio ExampleAlin TuvicPas encore d'évaluation
- Apex Institute of Engineering Department of Ait - Cse: B.E. CSE With Specialization in BDADocument13 pagesApex Institute of Engineering Department of Ait - Cse: B.E. CSE With Specialization in BDARitika MakhariaPas encore d'évaluation
- SFDC Lightning Training Basic 01Document79 pagesSFDC Lightning Training Basic 01kadek wijayaPas encore d'évaluation
- DC Proforma - Usg, CT, MriDocument2 pagesDC Proforma - Usg, CT, MriDhanusu PrincePas encore d'évaluation
- Humber Extramural Registration Form 2011-2012: A. Contact InformationDocument2 pagesHumber Extramural Registration Form 2011-2012: A. Contact InformationThushanth ChandrakumarPas encore d'évaluation
- Volunteer Application Care Beyond The BoulevardDocument2 pagesVolunteer Application Care Beyond The BoulevardAlisa Marie Buob JohnsonPas encore d'évaluation
- Patient/Client Information Form - Animal Medical ClinicDocument1 pagePatient/Client Information Form - Animal Medical ClinicArchetype ProductionsPas encore d'évaluation
- IDR Seminar Feb 2011 - Registration FormDocument1 pageIDR Seminar Feb 2011 - Registration Formvidhi8954Pas encore d'évaluation
- DHL EXPRESS Credit Application: CustomerDocument1 pageDHL EXPRESS Credit Application: CustomerpowerPas encore d'évaluation
- Choral Audition Form: Please Present This Form To The Instructor Upon Entering The Audition RoomDocument2 pagesChoral Audition Form: Please Present This Form To The Instructor Upon Entering The Audition RoomrobertcolbournePas encore d'évaluation
- Iadc / SPE Paper Information Form: 2018 SPE/IADC Middle East Drilling Technology Conference and ExhibitionDocument3 pagesIadc / SPE Paper Information Form: 2018 SPE/IADC Middle East Drilling Technology Conference and Exhibitionahmalisha2Pas encore d'évaluation
- Brand Evaluation Questionnaire SampleDocument3 pagesBrand Evaluation Questionnaire Samplevikash_anand3Pas encore d'évaluation
- Bid Document 1Document132 pagesBid Document 1ManojPas encore d'évaluation
- Blood Sugar Management in IcuDocument10 pagesBlood Sugar Management in IcuManojPas encore d'évaluation
- Variation FormatDocument23 pagesVariation FormatManojPas encore d'évaluation
- Procurement Management SlidesDocument14 pagesProcurement Management SlidesManojPas encore d'évaluation
- Case Presentation On Scrub TyphusDocument31 pagesCase Presentation On Scrub TyphusManojPas encore d'évaluation
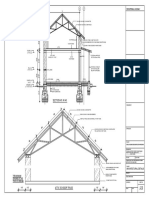
- Report-Metal Truss in Attic - FinalDocument43 pagesReport-Metal Truss in Attic - FinalManojPas encore d'évaluation
- Advance Module Unit 7 Infectious DiseasesDocument55 pagesAdvance Module Unit 7 Infectious DiseasesManojPas encore d'évaluation
- Standard Form of Contract 1Document24 pagesStandard Form of Contract 1ManojPas encore d'évaluation
- Metal Truss With AtticDocument2 pagesMetal Truss With AtticManojPas encore d'évaluation
- EQ EQ EQ EQ A B C: Roof Framing PlanDocument2 pagesEQ EQ EQ EQ A B C: Roof Framing PlanManojPas encore d'évaluation
- Room 1 9'-0"X9'-0" Room 2 9'-0"X9'-0": S.No Symbol Size NumberDocument3 pagesRoom 1 9'-0"X9'-0" Room 2 9'-0"X9'-0": S.No Symbol Size NumberManojPas encore d'évaluation
- Studies On Properties of TMT Steels For Structural Applications IJERTV2IS80657Document5 pagesStudies On Properties of TMT Steels For Structural Applications IJERTV2IS80657ManojPas encore d'évaluation
- Procurement Management: Weatherization Assistance ProgramDocument49 pagesProcurement Management: Weatherization Assistance ProgramManojPas encore d'évaluation
- Bidding and Contract DocumentDocument45 pagesBidding and Contract DocumentManojPas encore d'évaluation
- CSR FR HarjotoDocument36 pagesCSR FR HarjotoManojPas encore d'évaluation
- CSR & Corporate FraudDocument18 pagesCSR & Corporate FraudManojPas encore d'évaluation
- Fat Burn ConceptDocument31 pagesFat Burn ConceptManoj100% (1)
- Market Integration and Price Transmission in Selected Food and Cash Crop Markets of Developing CountriesDocument26 pagesMarket Integration and Price Transmission in Selected Food and Cash Crop Markets of Developing CountriesManojPas encore d'évaluation
- PP 90264 LIMS Integration Compliance ArabLab2017 PP90264 enDocument25 pagesPP 90264 LIMS Integration Compliance ArabLab2017 PP90264 enPaten PisanPas encore d'évaluation
- Public Records Report by Alameda County Grand JuryDocument6 pagesPublic Records Report by Alameda County Grand JuryTerry FranckePas encore d'évaluation
- The Research Proposal CH 1Document7 pagesThe Research Proposal CH 1Kamar FayezPas encore d'évaluation
- Energies 12 00446Document35 pagesEnergies 12 00446Vimal SamPas encore d'évaluation
- Auditing Database Auditing Database System System: Chapter 4-HallDocument35 pagesAuditing Database Auditing Database System System: Chapter 4-HallElyssaPas encore d'évaluation
- Acceptable Use AgreementDocument2 pagesAcceptable Use Agreementapi-325973069Pas encore d'évaluation
- Thesis Margins WordDocument8 pagesThesis Margins Wordjpcbobkef100% (2)
- Multistage Coil Gun Project ProposalDocument8 pagesMultistage Coil Gun Project ProposalAbdullah ArifPas encore d'évaluation
- Book Name Authors Publisher Amazon LinkDocument2 pagesBook Name Authors Publisher Amazon LinkOmar ShahidPas encore d'évaluation
- Computer Engineering Orientation - Module 02Document11 pagesComputer Engineering Orientation - Module 02Joel ManacmulPas encore d'évaluation
- Pat Load Moment IndicatorDocument79 pagesPat Load Moment IndicatorWilson torresPas encore d'évaluation
- MclustDocument57 pagesMclustfilip_nenadicPas encore d'évaluation
- Hola Compañero Aregla La Letra y Mandas Chao Conversation B Pair Work. DialogueDocument3 pagesHola Compañero Aregla La Letra y Mandas Chao Conversation B Pair Work. DialogueEly SaráuzPas encore d'évaluation
- Plug in DevelopmentDocument46 pagesPlug in DevelopmentJean claude onanaPas encore d'évaluation
- AmpliTube X-GEAR User ManualDocument84 pagesAmpliTube X-GEAR User ManualToriano LampkinPas encore d'évaluation
- Micro Sim TemplateDocument1 pageMicro Sim TemplateNikhil GargPas encore d'évaluation
- GSM GPRS GNSS HAT User Manual ENDocument32 pagesGSM GPRS GNSS HAT User Manual ENvinod kumarPas encore d'évaluation
- Ad Guard DNSDocument867 pagesAd Guard DNSDaniel RafaelPas encore d'évaluation
- Manual - Outland TechnologyDocument34 pagesManual - Outland TechnologyibrahimPas encore d'évaluation
- Electronics: Serial Expansion Using 74HC4052Document4 pagesElectronics: Serial Expansion Using 74HC4052Leonel FonsecaPas encore d'évaluation
- Cloud Native AttitudeDocument28 pagesCloud Native AttitudeRaghu VeerPas encore d'évaluation
- DimensioningDocument14 pagesDimensioningpaulo_rieloffPas encore d'évaluation
- RULE7-8 ProblemAnalysis PDFDocument109 pagesRULE7-8 ProblemAnalysis PDFMhae Torres100% (1)
- Tower of HanoiDocument2 pagesTower of Hanoiapi-281272453Pas encore d'évaluation
- Case - Breeden (B) - Recomputation of CostsDocument6 pagesCase - Breeden (B) - Recomputation of CostsRaviteja VeluvoluPas encore d'évaluation
- Smart Differential Pressure Transmitter Hdpm-41: PD Type PZ Type PZ316 Type PM12 TypeDocument3 pagesSmart Differential Pressure Transmitter Hdpm-41: PD Type PZ Type PZ316 Type PM12 TypemuhammetnaberPas encore d'évaluation
- Departmental Models 641a UpgradeDocument13 pagesDepartmental Models 641a UpgradeKrish NarajPas encore d'évaluation
- La Ideologia de Genero Jesus Trillo FigueroaDocument122 pagesLa Ideologia de Genero Jesus Trillo FigueroajcPas encore d'évaluation
- Nikon F6Document8 pagesNikon F6eternal_harpyPas encore d'évaluation
- Accounting Information Systems 7th Edition Hall Test BankDocument14 pagesAccounting Information Systems 7th Edition Hall Test Bankmisstepmonocarp1b69100% (27)