Vous aimerez peut-être aussi
- National Guidelines For Rabies Prophylaxis and Management in Nepal NewDocument57 pagesNational Guidelines For Rabies Prophylaxis and Management in Nepal NewNeha AmatyaPas encore d'évaluation
- Overview of EPI MyanmarDocument77 pagesOverview of EPI MyanmarSoe Htike0% (1)
- 1 - CEA - UAS Juni 2020Document9 pages1 - CEA - UAS Juni 2020astri rahayuPas encore d'évaluation
- COVID-19 Vaccine Daily Bulletin No. 253Document21 pagesCOVID-19 Vaccine Daily Bulletin No. 253Charlie ManilaPas encore d'évaluation
- The Vacinómetro® Initiative - An Eleven-Year Monitorization of Influenza Vaccination Coverage Rates Among Risk Groups in PortugalDocument4 pagesThe Vacinómetro® Initiative - An Eleven-Year Monitorization of Influenza Vaccination Coverage Rates Among Risk Groups in PortugalSofiaPas encore d'évaluation
- VAPP Assessment in Nigeria - Training - SODocument41 pagesVAPP Assessment in Nigeria - Training - SOTella AdedamolaPas encore d'évaluation
- Circulating Vaccine-Derived Polioviruses in The Extreme North RegionDocument4 pagesCirculating Vaccine-Derived Polioviruses in The Extreme North Regionxiongmao2389Pas encore d'évaluation
- Malaria Entomology and Vector Control: Guide For ParticipantsDocument192 pagesMalaria Entomology and Vector Control: Guide For Participantsakulianus AdiiPas encore d'évaluation
- Progress Toward Poliomyelitis Eradication - Afghanistan, January 2022-June 2023Document25 pagesProgress Toward Poliomyelitis Eradication - Afghanistan, January 2022-June 2023worksheetbookPas encore d'évaluation
- A Crosssectional Study On Caregivers Knowledge Attitudes and Practices About The Routine Immunisation Program in Tshwane SubdistriDocument11 pagesA Crosssectional Study On Caregivers Knowledge Attitudes and Practices About The Routine Immunisation Program in Tshwane SubdistriFortune JournalsPas encore d'évaluation
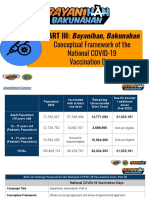
- Presentation For Governors and Mayors 02022022Document25 pagesPresentation For Governors and Mayors 02022022RANDY BAOGBOGPas encore d'évaluation
- COVID-19 Situational Report in The ASEAN Region: ASEAN Biodiaspora Virtual Center (ABVC)Document17 pagesCOVID-19 Situational Report in The ASEAN Region: ASEAN Biodiaspora Virtual Center (ABVC)Yati SPas encore d'évaluation
- Covid 19 Aefi ReportDocument32 pagesCovid 19 Aefi ReportIrenePas encore d'évaluation
- National Guidelines For RabiesDocument33 pagesNational Guidelines For RabiesNoahPas encore d'évaluation
- Preliminary Report of The Favipiravir Observational Study in JapanDocument6 pagesPreliminary Report of The Favipiravir Observational Study in JapanJosé PerníaPas encore d'évaluation
- Perbedaan IPV Dan OPVDocument9 pagesPerbedaan IPV Dan OPVIntan SaraswatiPas encore d'évaluation
- Rabies 2Document7 pagesRabies 2Nawal RaiPas encore d'évaluation
- Education Session For Trainers, Observers and Health-Care WorkersDocument116 pagesEducation Session For Trainers, Observers and Health-Care Workersseiguerly acosta montielPas encore d'évaluation
- Update 19 - EPI-WIN - COVID 19Document9 pagesUpdate 19 - EPI-WIN - COVID 19Karol AltamiranoPas encore d'évaluation
- Fvets 07 00477Document24 pagesFvets 07 00477Annisa YohanesPas encore d'évaluation
- Hicc For Nursing Excellence-Smh Sept 2018Document25 pagesHicc For Nursing Excellence-Smh Sept 2018RakshaPas encore d'évaluation
- The Value of Rotavirus Vaccination in Europe A Call For ActionDocument21 pagesThe Value of Rotavirus Vaccination in Europe A Call For ActionYELYMARPas encore d'évaluation
- Ppe 27Document3 pagesPpe 27Sajin AlexanderPas encore d'évaluation
- Addressing The Challenges and Opportunities of The Polio Endgame: Lessons For The FutureDocument8 pagesAddressing The Challenges and Opportunities of The Polio Endgame: Lessons For The Futuremuhfajar1_42539617Pas encore d'évaluation
- Assessment of Sars-Cov-2 Reinfection 1 Year After Primary Infection in A Population in Lombardy, ItalyDocument3 pagesAssessment of Sars-Cov-2 Reinfection 1 Year After Primary Infection in A Population in Lombardy, ItalyJimmy A. Camones ObregonPas encore d'évaluation
- Monkeypox External Sitrep FinalDocument11 pagesMonkeypox External Sitrep FinalAkshat SharmaPas encore d'évaluation
- Coronavirus Disease (COVID-19) : Situation Report - 185Document20 pagesCoronavirus Disease (COVID-19) : Situation Report - 185CityNewsTorontoPas encore d'évaluation
- MR Surveillance Guidelines IndiaDocument112 pagesMR Surveillance Guidelines IndiaHanumant NPas encore d'évaluation
- Monkeypox External SitrepDocument11 pagesMonkeypox External SitrepEsty Saehaebath KaengendPas encore d'évaluation
- PolioPipeline 08Document8 pagesPolioPipeline 08Subhajit BhattacharjeePas encore d'évaluation
- RGLC Mission Report India 2019Document25 pagesRGLC Mission Report India 2019dr satnam kaurPas encore d'évaluation
- Immunization in The Philippines:: Current Trends and The Way ForwardDocument22 pagesImmunization in The Philippines:: Current Trends and The Way ForwardFrance TorresPas encore d'évaluation
- Dark - Field Microscopic Analysis On The Blood of 1,006 Symptomatic Persons After Anti-Covid Mrna Injections From Pfizer/Biontech or ModernaDocument60 pagesDark - Field Microscopic Analysis On The Blood of 1,006 Symptomatic Persons After Anti-Covid Mrna Injections From Pfizer/Biontech or Modernasum wunPas encore d'évaluation
- EPHI - PHEOC - COVID-19 - Daily - SITREP-219 - English - 09032020Document14 pagesEPHI - PHEOC - COVID-19 - Daily - SITREP-219 - English - 09032020Abdulkerim Sultan TemmamPas encore d'évaluation
- Revising Wastage Concept NoteDocument6 pagesRevising Wastage Concept NoteNanda L PrasetyaPas encore d'évaluation
- UniversalDocument32 pagesUniversalRubina MasihPas encore d'évaluation
- Foot-And-: Vaccination Sample Testing of FMD Disease Within PakistanDocument14 pagesFoot-And-: Vaccination Sample Testing of FMD Disease Within PakistanQuratulainPas encore d'évaluation
- SURABAYA TB UPDATE DR - Asik SuryaDocument71 pagesSURABAYA TB UPDATE DR - Asik Suryawidya vannesaPas encore d'évaluation
- NAP (Harry P.) PDFDocument29 pagesNAP (Harry P.) PDFaldyPas encore d'évaluation
- Rafi Ullah Topic Covid 19 Microbiology 6 SemesterDocument7 pagesRafi Ullah Topic Covid 19 Microbiology 6 SemesterBalach ShahwaniPas encore d'évaluation
- Malaria Entomology and Vector Control: Guide For TutorsDocument50 pagesMalaria Entomology and Vector Control: Guide For TutorsSyed Sajid KamalPas encore d'évaluation
- Surveillance Guide For Vaccine-Preventable Diseases in The WHO South-East Asia RegionDocument28 pagesSurveillance Guide For Vaccine-Preventable Diseases in The WHO South-East Asia RegionDebPas encore d'évaluation
- Neurological Complications After First Dose of Covid-19 Vaccines and Sars-Cov-2 InfectionDocument20 pagesNeurological Complications After First Dose of Covid-19 Vaccines and Sars-Cov-2 InfectionJezreel ZaragosaPas encore d'évaluation
- 411 1828 1 PB PDFDocument5 pages411 1828 1 PB PDFednihsPas encore d'évaluation
- Core Health Indicators in The WHO European Region 2022Document18 pagesCore Health Indicators in The WHO European Region 2022IANCU ANDREI-RARESPas encore d'évaluation
- Pokusne Myši - DokumentDocument25 pagesPokusne Myši - DokumenthctagsPas encore d'évaluation
- Wsava 2010-3 PDFDocument34 pagesWsava 2010-3 PDFNasc710Pas encore d'évaluation
- COVIDDocument4 pagesCOVIDjoeyPas encore d'évaluation
- Pratik Singh 2101020551-ELDocument12 pagesPratik Singh 2101020551-ELHero PratikPas encore d'évaluation
- Antibiotic Guidelines - 2018 PDFDocument80 pagesAntibiotic Guidelines - 2018 PDFarnaldops333Pas encore d'évaluation
- Refkas2 1Document7 pagesRefkas2 1Frishia DidaPas encore d'évaluation
- This Content Downloaded From 85.186.63.198 On Wed, 29 Sep 2021 09:36:56 UTCDocument26 pagesThis Content Downloaded From 85.186.63.198 On Wed, 29 Sep 2021 09:36:56 UTCKollar RolandPas encore d'évaluation
- Maternal Sepsis 2022Document13 pagesMaternal Sepsis 2022Erika RosasPas encore d'évaluation
- jn.1 Ire CleanDocument6 pagesjn.1 Ire CleanKabakçı HüsnüPas encore d'évaluation
- E Cacy of Emergency Severity Index (ESI) in Early Identi Cation of Patients With Sepsis and Septic Shock at TriageDocument10 pagesE Cacy of Emergency Severity Index (ESI) in Early Identi Cation of Patients With Sepsis and Septic Shock at Triageputujunidtd13Pas encore d'évaluation
- Dark - Field Microscopic Analysis On The Blood of 1,006 Symptomatic Persons After Anti-COVID mRNA Injections From Pfizer/BioNtech or ModernaDocument60 pagesDark - Field Microscopic Analysis On The Blood of 1,006 Symptomatic Persons After Anti-COVID mRNA Injections From Pfizer/BioNtech or ModernaJim Hoft100% (2)
- Vaccination HealthDocument44 pagesVaccination HealthCtPas encore d'évaluation
- Potential Antiviral Agents for Coronaviruses: Compounds, Herbal Products, and Drug TargetsD'EverandPotential Antiviral Agents for Coronaviruses: Compounds, Herbal Products, and Drug TargetsPas encore d'évaluation
- Botany AssignmentDocument21 pagesBotany Assignmentabdul hadiPas encore d'évaluation
- National Polio Eradication ProgramDocument36 pagesNational Polio Eradication Programayushi rainaPas encore d'évaluation
- Social Pharmacy Practical 1Document35 pagesSocial Pharmacy Practical 1Devam VanjariPas encore d'évaluation
- Des 2014Document6 pagesDes 2014HisokagenPas encore d'évaluation
- Global Polio Survilance Action Plan 2022-2024Document90 pagesGlobal Polio Survilance Action Plan 2022-2024monoluPas encore d'évaluation
- بحث عن مرض شلل الاطفالDocument20 pagesبحث عن مرض شلل الاطفالahmed_samy_3Pas encore d'évaluation
- Monitoring Format HTH RI + MI - Apr2017Document3 pagesMonitoring Format HTH RI + MI - Apr2017Anonymous WgPzfGKR50% (2)
- Virology: EnterovirusesDocument40 pagesVirology: EnterovirusesMeevie ToledoPas encore d'évaluation
- Afp Surveillance 21st Century 0Document25 pagesAfp Surveillance 21st Century 0cavmichaelPas encore d'évaluation
- Polio Facts and FiguresDocument6 pagesPolio Facts and FiguresAmaka Cecilia0% (1)
- Oral Polio Vaccine Product Insert by GlaxoSmithKlineDocument7 pagesOral Polio Vaccine Product Insert by GlaxoSmithKlineHeather X RhodesPas encore d'évaluation
- Current Affairs IASBABADocument180 pagesCurrent Affairs IASBABAGPT SURPURPas encore d'évaluation
- General Recommendation On ImmunizationDocument19 pagesGeneral Recommendation On ImmunizationRickyNoviantoPas encore d'évaluation
- The EPI Routine Schedule of Immunization in The PhillippinesDocument21 pagesThe EPI Routine Schedule of Immunization in The PhillippinesJesse Martin100% (1)
- Customer Satisfactionarticlepage 36Document85 pagesCustomer Satisfactionarticlepage 36horaezPas encore d'évaluation
- Animal Cell Culture Animal Biotech: Name-Rahul Verma Roll. No.-26Document12 pagesAnimal Cell Culture Animal Biotech: Name-Rahul Verma Roll. No.-26Rahul VermaPas encore d'évaluation
- Vaccine Illusion GMIDocument117 pagesVaccine Illusion GMIPepe100% (4)
- EPI Vaccines HandoutsDocument14 pagesEPI Vaccines HandoutsStephen Pilar PortilloPas encore d'évaluation
- MR-OPV Webinar For Vaccination Teams 8 OctDocument101 pagesMR-OPV Webinar For Vaccination Teams 8 OctBrai Ən100% (1)
- Booklet-Health Centre Simple Guide For Reaching Every PurokDocument38 pagesBooklet-Health Centre Simple Guide For Reaching Every PurokchatePas encore d'évaluation
- Adverse Event Following Immunization (AEFI) Manual of Procedures, 2014Document106 pagesAdverse Event Following Immunization (AEFI) Manual of Procedures, 2014Jezza Jonah AclanPas encore d'évaluation
- Introduction To Community Health and Environmental SanitationDocument44 pagesIntroduction To Community Health and Environmental Sanitationbayenn100% (3)
- Doctor Interviews Documentaries & Research QuotesDocument32 pagesDoctor Interviews Documentaries & Research QuotesjdhPas encore d'évaluation
- Immunization Program of The PhilippinesDocument9 pagesImmunization Program of The Philippinesnelar MacabalitaoPas encore d'évaluation
- Gajdos 2015Document9 pagesGajdos 2015Rafa NaufalinPas encore d'évaluation
- HHS & Fda 1984Document4 pagesHHS & Fda 1984Heather X Rhodes100% (1)
- Orthopaedic MX PolioDocument6 pagesOrthopaedic MX Polioloka jananiPas encore d'évaluation
- Bibliography MaiyaDocument5 pagesBibliography Maiyame1929Pas encore d'évaluation
- A4 Size MC3 Midterms ReviewerDocument9 pagesA4 Size MC3 Midterms ReviewerEl Grace EligedoPas encore d'évaluation
- Scientific American 1993-2013 Article IndexDocument147 pagesScientific American 1993-2013 Article IndexamlferreiraPas encore d'évaluation