Vous aimerez peut-être aussi
- Rhinosin Cuurent Concepts JadiDocument64 pagesRhinosin Cuurent Concepts JadiElsa OctaviaPas encore d'évaluation
- Diagnosis & Classification of Periodontal DiseasesDocument19 pagesDiagnosis & Classification of Periodontal DiseasesMatthew SenyahPas encore d'évaluation
- Aggressive Periodontitis GoodDocument99 pagesAggressive Periodontitis GoodDr.Manisha DeolPas encore d'évaluation
- Periodontic - EndodonticDocument86 pagesPeriodontic - EndodonticPiyusha SharmaPas encore d'évaluation
- Oral Medicine Questions: Causes, Symptoms and ManagementDocument7 pagesOral Medicine Questions: Causes, Symptoms and ManagementAhmed HusseinPas encore d'évaluation
- Classification of Periodontal DiseasesDocument27 pagesClassification of Periodontal DiseasesbenazirghaniPas encore d'évaluation
- Classification of Periodental LesionsDocument6 pagesClassification of Periodental LesionsAsia IbraheemPas encore d'évaluation
- Presented by DR Ekta Garg Mds 1 Year Department of Conservative Dentistry & EndodonticsDocument107 pagesPresented by DR Ekta Garg Mds 1 Year Department of Conservative Dentistry & Endodonticsjibin kareemPas encore d'évaluation
- Classification Diagnosis and Clinical Manifestatio PDFDocument20 pagesClassification Diagnosis and Clinical Manifestatio PDFdzakki saragihPas encore d'évaluation
- Principles of Periodontology: A D, S L, J M & A F. HDocument38 pagesPrinciples of Periodontology: A D, S L, J M & A F. Hmaribel suarezPas encore d'évaluation
- Introduction To PeriodontologyDocument88 pagesIntroduction To PeriodontologyHina MahmoodPas encore d'évaluation
- Classification of Periodontal Disease 1Document54 pagesClassification of Periodontal Disease 1violaPas encore d'évaluation
- Classification of Periodontal Diseases PerioDocument42 pagesClassification of Periodontal Diseases PerioFourthMolar.comPas encore d'évaluation
- Causes and Effects of Periodontal DiseasesDocument17 pagesCauses and Effects of Periodontal DiseasesFatima Habib JajjaPas encore d'évaluation
- Endo-Perio Continuum A Review From Cause To CureDocument4 pagesEndo-Perio Continuum A Review From Cause To CureRiezaPas encore d'évaluation
- CYSTSDocument12 pagesCYSTSGowriPas encore d'évaluation
- AggressiveDocument55 pagesAggressiveSaima KhanPas encore d'évaluation
- Oral Medicine - Update For The Dental PractitionerDocument8 pagesOral Medicine - Update For The Dental PractitionernavyaPas encore d'évaluation
- Endodonticsurgery - FinalDocument70 pagesEndodonticsurgery - FinalSurya Jayaprakash100% (1)
- Classification of Periodontal DiseasesDocument20 pagesClassification of Periodontal DiseasesDhinda AuliaPas encore d'évaluation
- Dental Caries and Its Management-1Document111 pagesDental Caries and Its Management-1Anushriya Dutta71% (7)
- Classification of Periodontal Diseases: DR Prateek ShresthaDocument28 pagesClassification of Periodontal Diseases: DR Prateek ShresthaHimalayawandererPas encore d'évaluation
- Periodontal conditions in the Australian Defence ForceDocument5 pagesPeriodontal conditions in the Australian Defence ForceGreg MendozaPas encore d'évaluation
- Screenshot 2021-12-22 at 1.54.50 PMDocument9 pagesScreenshot 2021-12-22 at 1.54.50 PMSilky GroverPas encore d'évaluation
- Aggressive Periodontitis: Case Definition and Diagnostic CriteriaDocument15 pagesAggressive Periodontitis: Case Definition and Diagnostic Criteriadileep9002392Pas encore d'évaluation
- Diagnosis and Classification of Periodontal DiseasesDocument97 pagesDiagnosis and Classification of Periodontal DiseasesAssssssPas encore d'évaluation
- NDB II ReviewDocument76 pagesNDB II ReviewHanin AbukhiaraPas encore d'évaluation
- M1 Lesson 1 Intro to PeriodontologyDocument15 pagesM1 Lesson 1 Intro to PeriodontologytriciaPas encore d'évaluation
- Lingual Bony Protruberances - A Retrospective AnalysisDocument2 pagesLingual Bony Protruberances - A Retrospective AnalysisAgustin BiagiPas encore d'évaluation
- CLASSIFICATION OF PERIODONTAL DISEASES - 3rd YearDocument54 pagesCLASSIFICATION OF PERIODONTAL DISEASES - 3rd Yearapi-3775747100% (11)
- 1 - Natural History of Periodontal DiseaseDocument42 pages1 - Natural History of Periodontal DiseasejazzPas encore d'évaluation
- Periodontal Diseases in Children PedoDocument34 pagesPeriodontal Diseases in Children PedoFourthMolar.comPas encore d'évaluation
- Endo PerioDocument41 pagesEndo Periovishrutha purushothamPas encore d'évaluation
- Pulp & Periapical Lesions Lecture on OsteomyelitisDocument77 pagesPulp & Periapical Lesions Lecture on OsteomyelitisAMIT GUPTAPas encore d'évaluation
- Aggressive Periodontitis Guide for Dental StudentsDocument12 pagesAggressive Periodontitis Guide for Dental StudentsPatriciaXavier100% (1)
- Classification and Types of Periodontal DiseasesDocument20 pagesClassification and Types of Periodontal DiseasesMadinah ZainalPas encore d'évaluation
- The Relationship Between Periodontal and Pulpal DiseaseDocument15 pagesThe Relationship Between Periodontal and Pulpal DiseaseLigia LoaizaPas encore d'évaluation
- Cyst Theory ClassDocument310 pagesCyst Theory ClasswakoPas encore d'évaluation
- PATH-261 (SPO) L2SII Theory (Full)Document174 pagesPATH-261 (SPO) L2SII Theory (Full)Shakil MahmodPas encore d'évaluation
- AGGRESSIVE PERIODONTITIS: AN INTRODUCTIONDocument101 pagesAGGRESSIVE PERIODONTITIS: AN INTRODUCTIONdileep900Pas encore d'évaluation
- Controversies in PeriodonticsDocument56 pagesControversies in PeriodonticsReshmaa Rajendran100% (1)
- Austin: An Unusual Manifestation of Cutaneous Sarcoidosis in The Oral CavityDocument2 pagesAustin: An Unusual Manifestation of Cutaneous Sarcoidosis in The Oral CavityRENITA USWATUN HASANAH 1Pas encore d'évaluation
- OsteomaDocument4 pagesOsteomaAnjungAdelPas encore d'évaluation
- Periodontics PDFDocument195 pagesPeriodontics PDFدينا حسن نعمة100% (1)
- Diagnosis and Classification of Periodontal Diseases 1Document37 pagesDiagnosis and Classification of Periodontal Diseases 1AssssssPas encore d'évaluation
- Classification of DiseasesDocument20 pagesClassification of Diseasesarun perioPas encore d'évaluation
- Casereport SevereinfraocclDocument6 pagesCasereport SevereinfraocclElisabeth FransiskaPas encore d'évaluation
- DX of Pulpal N Apical Dis. NICEDocument29 pagesDX of Pulpal N Apical Dis. NICEnoreenmyanmarPas encore d'évaluation
- Abscess of THE PeriodontiumDocument57 pagesAbscess of THE PeriodontiumSandeep SunilPas encore d'évaluation
- PericoronitisAugSept09 PDFDocument11 pagesPericoronitisAugSept09 PDFDiana FitriPas encore d'évaluation
- Oral and Perioral Piercing ComplicationsDocument4 pagesOral and Perioral Piercing ComplicationsGabrielle CorreiaPas encore d'évaluation
- Periodontology SeqDocument17 pagesPeriodontology SeqsarahPas encore d'évaluation
- ENDO PerioDocument39 pagesENDO PerioapbhalodiPas encore d'évaluation
- Periodontitis: DR - Nael Almasri PeriodontistDocument55 pagesPeriodontitis: DR - Nael Almasri PeriodontistDentist AymanPas encore d'évaluation
- Non Cervical Lesions Meena MamDocument120 pagesNon Cervical Lesions Meena Mamanshida v pPas encore d'évaluation
- Controversies IN Periodontics: BY K. Shiva Charan YadavDocument122 pagesControversies IN Periodontics: BY K. Shiva Charan YadavShiva renu08Pas encore d'évaluation
- Chronic Periodontitis GuideDocument80 pagesChronic Periodontitis GuideDrRahat SaleemPas encore d'évaluation
- Aggressive Periodontitis GuideDocument54 pagesAggressive Periodontitis GuideDrMahendra SagarPas encore d'évaluation
- Awareness of Oral Manifestations Related To Systemic DiseasesDocument5 pagesAwareness of Oral Manifestations Related To Systemic DiseasesInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Untitled 5Document1 pageUntitled 5rindu dinantiPas encore d'évaluation
- G Oralsurgery PDFDocument8 pagesG Oralsurgery PDFAinun Nur ArifahPas encore d'évaluation
- Effect of Immediate Periodontal Surgical Treatment On Periodontal Healing inDocument8 pagesEffect of Immediate Periodontal Surgical Treatment On Periodontal Healing inrindu dinantiPas encore d'évaluation
- Transcript of Academic Records Rindu IVDocument11 pagesTranscript of Academic Records Rindu IVrindu dinantiPas encore d'évaluation
- The 2 Dialogue of Fantastic Group Electra English CourseDocument1 pageThe 2 Dialogue of Fantastic Group Electra English Courserindu dinantiPas encore d'évaluation
- Aetiology of Root Canal Treatment Failure - Why Well-Treated Teeth Can FailDocument10 pagesAetiology of Root Canal Treatment Failure - Why Well-Treated Teeth Can FailFlorin IonescuPas encore d'évaluation
- Vocab 1Document9 pagesVocab 1rindu dinantiPas encore d'évaluation
- 1Document1 page1rindu dinantiPas encore d'évaluation
- English Course Student RankingsDocument1 pageEnglish Course Student Rankingsrindu dinantiPas encore d'évaluation
- Untitled 2Document1 pageUntitled 2rindu dinantiPas encore d'évaluation
- Fantastic Group English Course Top StudentsDocument1 pageFantastic Group English Course Top Studentsrindu dinantiPas encore d'évaluation
- Untitled 6Document1 pageUntitled 6rindu dinantiPas encore d'évaluation
- KJFSFDGSKLDocument1 pageKJFSFDGSKLrindu dinantiPas encore d'évaluation
- Untitled 7Document1 pageUntitled 7rindu dinantiPas encore d'évaluation
- Untitled 7Document1 pageUntitled 7rindu dinantiPas encore d'évaluation
- Untitled 1Document1 pageUntitled 1rindu dinantiPas encore d'évaluation
- Untitled 12Document1 pageUntitled 12rindu dinantiPas encore d'évaluation
- AsasasDocument2 pagesAsasasrindu dinantiPas encore d'évaluation
- Untitled 2Document1 pageUntitled 2rindu dinantiPas encore d'évaluation
- Untitled 9Document1 pageUntitled 9rindu dinantiPas encore d'évaluation
- Untitled 5Document1 pageUntitled 5rindu dinantiPas encore d'évaluation
- Untitled 6Document1 pageUntitled 6rindu dinantiPas encore d'évaluation
- AsasasDocument2 pagesAsasasrindu dinantiPas encore d'évaluation
- Conclusion 6 (Wisdom Teeth)Document1 pageConclusion 6 (Wisdom Teeth)rindu dinantiPas encore d'évaluation
- Paper Kel 1Document6 pagesPaper Kel 1NatAsyaPas encore d'évaluation
- Space Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillDocument8 pagesSpace Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillAnonymous JR1VNCPas encore d'évaluation
- PULP TESTS-converted EndodonticsDocument12 pagesPULP TESTS-converted EndodonticsWajeeha Khan KhattakPas encore d'évaluation
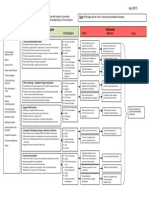
- Appendicitis AlgorithmDocument3 pagesAppendicitis AlgorithmErlanggaPrasamyaPas encore d'évaluation
- Iridology Is NonsenseDocument4 pagesIridology Is NonsenseJonas Sunshine Callewaert25% (4)
- EPIPENDocument2 pagesEPIPENLana MohPas encore d'évaluation
- Endo Don TicDocument8 pagesEndo Don TicArmareality Armareality100% (1)
- Psycho-Oncology - 2018 - Die Trill - Jimmie Holland The Founder Developer and The Soul of The InternationalDocument3 pagesPsycho-Oncology - 2018 - Die Trill - Jimmie Holland The Founder Developer and The Soul of The InternationalReginaPas encore d'évaluation
- OTDCP: Herpes Simplex: Case History and FindingsDocument4 pagesOTDCP: Herpes Simplex: Case History and FindingsMaggie DuttaPas encore d'évaluation
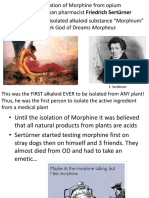
- Appendix1 MorphineDocument75 pagesAppendix1 Morphine민규강Pas encore d'évaluation
- Cpi PortfolioDocument9 pagesCpi Portfolioapi-621459006Pas encore d'évaluation
- Nursing Care For Special Groups:Children, Adolescents, Adult, Woman and ElderlyDocument10 pagesNursing Care For Special Groups:Children, Adolescents, Adult, Woman and Elderlypramod kumawatPas encore d'évaluation
- Promoting Immunization Program Logic ModelDocument1 pagePromoting Immunization Program Logic ModelPheresPas encore d'évaluation
- Vaccines For Corona Virus Project-1Document28 pagesVaccines For Corona Virus Project-1Ananya PuhanPas encore d'évaluation
- CAT Bedah Plastik - JokoDocument10 pagesCAT Bedah Plastik - JokoOtto NaftariPas encore d'évaluation
- The Book 2016Document144 pagesThe Book 2016Calder JohnsonPas encore d'évaluation
- What Is Uterine ProlapseDocument4 pagesWhat Is Uterine Prolapsestoopid08Pas encore d'évaluation
- KLE Pharmacy - NPC Brochure 2022Document13 pagesKLE Pharmacy - NPC Brochure 2022Bhaskar PandeyPas encore d'évaluation
- 03 MFDS Regulations & Syllabus 2011Document15 pages03 MFDS Regulations & Syllabus 2011FarahMohammed1Pas encore d'évaluation
- Lecture 4 - IUGR, Dr. Dr. Diah Rumekti H SP - OG (K) (2021)Document59 pagesLecture 4 - IUGR, Dr. Dr. Diah Rumekti H SP - OG (K) (2021)ofa daniPas encore d'évaluation
- PreviewpdfDocument23 pagesPreviewpdfKhaalid AbdirahmanPas encore d'évaluation
- Certified Nurse Anesthetist (CRNA)Document4 pagesCertified Nurse Anesthetist (CRNA)api-78920101Pas encore d'évaluation
- Type of Article: Bibliometric Analysis of Articles Published in Physical Therapy, 1980 - 2009Document6 pagesType of Article: Bibliometric Analysis of Articles Published in Physical Therapy, 1980 - 2009Naveen KumarPas encore d'évaluation
- Amira - Malaysia Healthcare Financing SystemDocument21 pagesAmira - Malaysia Healthcare Financing SystemJKN RSUB100% (1)
- Snakebite First Aid PosterDocument1 pageSnakebite First Aid Postervet mhmdPas encore d'évaluation
- Drug Study Activity ErythromycinDocument2 pagesDrug Study Activity ErythromycinNELL JOSHUA PANTIGPas encore d'évaluation
- Helping Our Seniors Get The Covid 19 VaccineDocument1 pageHelping Our Seniors Get The Covid 19 VaccineNews-PressPas encore d'évaluation
- Letter of RecommendationDocument2 pagesLetter of RecommendationpgregorybubblesPas encore d'évaluation
- Management of MedicationDocument40 pagesManagement of MedicationKannu SharmaPas encore d'évaluation
- 2023 07 11 12-08-57 PMDocument1 page2023 07 11 12-08-57 PMlokman hossenPas encore d'évaluation